On average, we could obtain 200-300 µg endotoxin-free expression plasmid NR1-GFP and GFP from 250 mL bacterial culture following the procedures described in section 1 of the protocol. An amount of 100 ng/well of the expression plasmid was used for the transfection of the HEK293 cells cultured in the 48-well plate as described in the section 2 of the protocol. 24-30 h after transfection, the cells expressed the NR1-GFP, and GFP recombinant proteins could be detected under fluorescent microscope. Figure 1A shows the image of the host cells that express the NR1-GFP, while Figure 1D shows the cells expressing GFP. The green signal can be used as a quality controller of the assay: approximately 30% of the cells had the green signals under the fluorescent microscope. Figure 1A and 1D show the image of the host cells that express the NR1-GFP. The green signal can be used as a quality controller of the assay: approximately 30% of the cells had the green signals under the fluorescent microscope. The cells expressing NR1-GFP were used for screening the presence of anti-NMDA receptor autoantibodies in the human plasma sample.
In the cell-based immunofluorescence assay as described in the section 3 of the protocol, the positive control sample (obtained from a commercial source, see Table of Materials) was added to the pooled plasma in 1:10 dilution according to the manufacturer's instructions. The pooled plasma was prepared from 5 adult males and 5 adult females. Figure 1B is the Alexa Fluor-594 image of positive control sample after incubation with the cells expression NR1-GFP, while Figure 1E is the Alexa Fluor-594 image of positive control sample after incubation with the cells expression GFP. Figure 1C is the merged image of Figure 1A and Figure 1B: there are significant overlaps of green signals and red signals in the same cell, indicating the co-localization of NR1-GFP and the antibodies against the NR1 subunit of NMDA receptor (arrows). A plasma sample that shows greater than 30% overlaps of green and red signals will be interpreted as positive in this case. Figure 1F is the merged image from Figure 1D and Figure 1E that serves as the negative control for Figure 1C. The weak red color is background fluorescence of the Alexa Fluor-594 image. There is little overlap of green and red signals, indicating no binding of the anti-NMDA receptor autoantibody against the recombinant protein.
During the establishment of the experimental procedures, we observed a low signal-to-noise ratio of the Alexa Fluor-594 image when the plasma samples were tested. We attempted to optimize the signal-to-noise ratio by conducting a serial dilution of the plasma form 1:10, 1:50, 1:100, and 1:200, and testing different concentrations of Alex Fluor-594 labeled secondary antibody from 1:500 to 1:2,000. We found that 1:100 dilution of the plasma and 1:1,000 or 1:2,000 dilution of the Alexa Fluor-594 were the optimal conditions for the interpretation of the data.
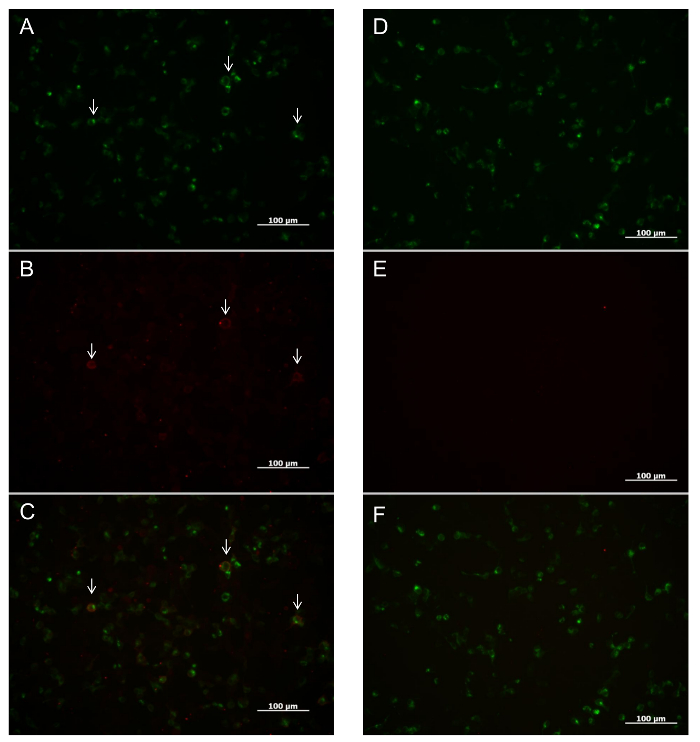
Figure 1: Representative images of the cell-based immunofluorescence assay to detect anti-NMDA receptor autoantibody. (A) Image of the HEK293 cells that express NR1-GFP. (B) The Alexa Fluor-594 image taken from the same field of A after incubation with the positive control sample. Red signal indicates the binding of the anti-NMDA receptor autoantibodies to the NR1 expressed in the HEK293 cells. (C) The merged image of A and B. Yellow color indicates the co-localization of the NR1 (green signal) and the anti-NMDA receptor autoantibodies (red signal). Arrows indicate examples of some prominent cells showing co-localization of NR1-GFP and anti-NMDA receptor autoantibodies. (D) Image of the HEK293 cells expressing NR1-GFP. (E) The Alexa Fluor-594 image taken from the same field of D after incubation with the positive control sample. Weak red signal indicates the background noise of Alexa Fluor-594 image. (F) The merged image of D and E. This image serves as a negative control, as there is little yellow signal observed. The negative control image shows the specific binding of the anti-NMDA receptor antibodies to the NR1-GFP in the assay. All the images were taken under 10X eye lens and 20X lens objective. Please click here to view a larger version of this figure.
