The study entitled "Effects of inhaled Xe and N2O on brain activity recorded using EEG and MEG" was approved (approval number: 260/12) by the Alfred Hospital and Swinburne University of Technology Ethics Committee and met the requirements of the National Statement on Ethical Conduct in Human Research (2007).
1. Participant Selection and Pre-Study Requirements
- Conduct an interview to select healthy, right handed, adult males between the ages of 20 and 40 years old.
- Confirm a good general health status by obtaining the participant's Body Mass Index (BMI) and the lack of contraindications to MRI or MEG (such as implanted metallic foreign bodies), as well as collecting a detailed medical history including any previous surgeries, importantly any unfavorable reactions to general anesthesia which would result in exclusion from the study.
- Specifically exclude any recent intake of psychoactive or other prescribed medication as well as ensuring the absence of any recreational drug use and the lack of any neurological disorder, epilepsy, heart conditions, sleep apnea, motion sickness and claustrophobia. As it will be subsequently important to obtain a good seal with an anesthetic face mask exclude participants who have large beards, unless they are willing to shave.
NOTE: Exclude females due to the documented effects of menstruation57 and/or age extremes on the resting MEG/EEG signal as well as the increased propensity to nausea and vomiting58.
- Follow the day stay general anesthesia procedure as designated in the Australia and New Zealand College of Anaesthetists (ANZCA) guidelines (Document PS15).
- In line with these guidelines, ask the subjects to fast for at least 6 hours and consume no liquids for at least 2 hours prior to the start of the experiment. Confirm compliance by having the anesthesiologist contacting the participant the day before the testing takes place.
- After the completion of the experiment, have subjects undergo standard post anesthesia care monitoring by instructing them not to operate any heavy machinery or make important decisions within 24 hours of the experiment (due to the possibility of residual low level cognitive impairment from Xe and N2O).
2. Facilities and Equipment
NOTE: The facilities are in accordance with ANZCA requirements for the delivery of anesthesia outside a normal surgical operating suite (http://www.anzca.edu.au/resources/professional-documents. Document PS55). Specifically, the room satisfies engineering regulations for electrical safety and gas medical administration.
- Run the experiment at the Swinburne Advanced Technology Centre's Brain Imaging laboratory, namely the MEG room which contains a magnetically shielded room (MSR) that houses the MEG scanner. The shielded room sits on a floating floor isolated from environmental movements such as passing trains.
- Deliver anesthesia gases using an anesthesia machine, located outside the MSR, capable of delivery and monitoring gaseous xenon. This anesthesia machine is specially designed to administer closed-loop low flow Xe gas and to measure end-tidal Xe concentrations using katharometry (thermal conductivity; ± 1% accuracy), in addition to providing standard-of-care patient monitoring. This includes end-tidal O2, CO2, N2O measurement (where appropriate), pulse oximetry, 3-lead ECG, and non-invasive blood pressure measurement (NIBP) as per ANZCA Guideline Document PS18. Measure end-tidal N2O concentrations using infrared spectroscopy implemented in the anesthesia machine.
- Pipe the gases to participants using extended 22 mm diameter breathing hoses passing through MSR conduits.
- Provide standard-of-care patient monitoring as per ANZCA Guideline Document PS18. This includes end-tidal O2, CO2, N2O measurement (where appropriate), pulse oximetry, 3-lead ECG, and non-invasive blood pressure measurement (NIBP).
- Monitor blood pressure as per ANZCA Guideline Document PS18 using a non-invasive blood pressure monitor located outside the MSR and connected by a long inflation tube to a cuff placed on the upper arm.
- Throughout the experiment, record and document all physiological parameters at 1 min intervals in addition to an automated recording of all parameters every 30 s.
- Make sure that the gases are piped to participants using extended 22 mm diameter breathing hoses passing through MSR conduits. A suction system is located outside the MSR and a long delivery tube, connected to a Yankauer suction wand is passed through a conduit to be placed close to both the patient and clinical observer.
- In addition, ensure emesis basins are located close by within the MSR to enable their rapid positioning by the observer upon occurrence of emesis. The clinical observer within the MSR will need to remain vigilant to any airway obstruction, responding initially with a chin lift or jaw thrust and immediately discontinue the protocol if impending emesis is signaled by excessive swallowing or retching or airway obstruction is not resolved by the chin life or jaw thrust.
- Record EEG using an MEG compatible 64-channel Ag/AgCl electrode cap attached to a battery powered amplifier within the MSR. The amplifier is connected via a fiber-optic cable and a suitable media converter to a laptop running a compatible acquisition software.
- Record brain magnetic field activity (MEG) at a sampling rate of 1000 Hz using an MEG system that has whole brain coverage and has well defined arrays of sensors that may include magnetometers and axial/planar gradiometers; the present study utilizing a system comprised of 102 magnetometers and 204 planar gradiometers. To avoid complexities not directly relevant to the protocol or the MEG system configuration, example data from the magnetometers alone is reported, although both magnetometer and gradiometer data is acquired as part of the protocol.
- Track head position continuously using 5 head position indicator (HPI) coils. Digitize the location of the head coils, EEG electrodes and fiducial markers (nasion and left and right preauricular points) before MEG scanning using appropriate digitizing equipment.
- Because the aim is to obtain results in source space, disable any internal active shielding system employed by the MEG system for three-dimensional noise cancellations, in order to make the processing pipeline flexible with regards to the use of signal space separation (SSS) methods that are typically employed.
- Use an MRI scanner to obtain corresponding T1-weighted structural brain scans for later co-registration with M/EEG recordings.
3. Study Design and Protocol
NOTE: A two-way crossover experimental protocol is followed. Perform two separate testing sessions for each subject separated by a maximum of four weeks between testing sessions. One arm of the study consists of Xe administration while N2O is given in the second arm. Participants are blind to the type of gas being administered while the medical staff and researchers are not due to the slight differences in the procedure followed for their administration.
- After informed consent is obtained, confirm participant eligibility with an extensive medical history interview and vital sign measurements which include blood pressure, heart rate, body temperature and peak expiratory flow. After participant eligibility is confirmed, the subject undergoes a brief measurement in the MEG to ensure that there are no unanticipated sources of noise.
- Place the EEG cap on the subject's head and gel all electrodes. Attach the 5 HPI coils on the cap to continuously record head position in the MEG.
- Digitize the EEG-channels, HPI coil positions and extra points on the subject's nose and store all locations using the MEG's accompanying software package.
- Move the subject to the MSR, connect the electrode cap to the EEG amplifier and re-gel electrodes if required to ensure that their electrical contact impedances are below 5 kΩ.
- In addition to the MEG and EEG, make three additional bipolar bio-channel recordings.
- Because anesthetic agent administration is associated with changes in muscle tone, record the electromyogram (EMG) using a pair of single-use Ag/AgCl electrodes placed submentally to record the activity of the mylohyoid and digastric (anterior belly) muscles.
- Record the electro-oculogram (EOG) by attaching a pair of electrodes above one of the eyes, near the brow, and near the corresponding lateral canthus and perform three-lead electrocardiogram (ECG) recordings using electrodes on each wrist and an elbow ground (see Figure 1).
- Ask participants to keep the eyes closed during all recording phases of the experiment.
- Perform clinical management of the subject with an anesthesiologist and an anesthetic nurse or other suitably trained clinical observer. Have the nurse/observer sit with the subject in the MSR in order to continuously monitor the participant's condition (in particular the face mask seal and subject's airway) and the anesthesiologist, located in the control room to manage gas delivery and electronic monitoring.
- Collect data in a team of three: one member monitoring and controlling the acquisition of the MEG signal, another monitoring and controlling the acquisition of the EEG and another starting and stopping the computerized auditory continuous performance task while monitoring the subjects' responses, coordinating all experimental timings and recording minute blood pressure, and end-tidal gas concentrations and gas flow rate as provided by the anesthesiologist.
- Continuously visually monitor the participant in the MSR via a suitable camera, which also records all stages of the experiment for subsequent assessment and review.
- Behaviorally measure the ongoing level of responsiveness throughout the experiment using an auditory continuous performance task (aCPT). Use MEG compatible headphones to deliver a binaural auditory tone of either 1 or 3 kHz frequency of fixed stereo amplitude (approx. 76 dBA), with an inter-stimulus interval of between 2 to 4 seconds drawn from a uniform distribution.
- Ask the participant to respond as quickly as possible using two separate button boxes held in each hand. Use the left and right buttons on each box correspond to a low or high frequency tone, respectively, and the left and right button boxes, respectively, for the participant to indicate the absence or presence of nausea.
- Closely monitor responsiveness throughout the experiment. The reaction time latency and accuracy (percentage of tones correctly classified) of the responses are automatically recorded as well as displayed on a monitor outside the MSR for the researchers to obtain a real time indication of the participants' behavioral state.
- Following multiple sequential right button box responses (indicating nausea), alert the observer in the MSR and the administering anesthesiologist that gas administration may need to be abruptly terminated to avoid emesis.
- Record eyes closed resting EEG and MEG for 5 min followed by a 5 min eyes closed baseline EEG/MEG recording with the subject performing the aCPT task.
- Remove the subject from the MSR and allow for a 20 gauge intravenous cannula to be placed in the left antecubital fossa by the anesthesiologist. Anti-emetic administration, occurring slowly over a period of 1 – 2 minutes, consisting of 4 mg dexamethasone and 4 mg ondansetron59, follows to prevent any emesis caused by anesthetic gas inhalation, which is often observed with N2O at the higher concentrations used60.
- Attach the face mask and breathing circuit to the subject using a modified sleep apnea continuous positive airways pressure (CPAP) harness, and assess for subject comfort and the absence of any leakage at 5 cm H2O positive pressure.
- Return the subject to the MSR to remain seated in the MEG for the remainder of the study.
- Take a number of preventative steps to ensure limited subject movement during the simultaneous MEG and EEG recordings, since head and body movement can cause large artifacts in electromagnetic recordings and are expected to occur during the administration of the dissociative anesthetic agents due to their well-known propensity to induce psychomotor agitation.
- Place a custom-built cap made of a low density uncolored foam on the head which secures the head position inside the MEG dewar helmet irrespective of head size and shape.
- Further, use a cloth harness wrapped around the thighs and the gluteal muscles and secured to the back of the MEG chair to minimize any sagging/slouching that occurs in the participant's vertical position (see Figure 1).
- During the recording, track the head position continuously using the HPI coils, to view offline after completion of the experiment (see data analysis section for further details).
- Once the participant is securely positioned, administer 100% inspired O2 and continue this for up to 30 minutes until their end-tidal O2 concentration is >90% indicating they are effectively de-nitrogenated, a process necessary to ensure accurate measurements of end-tidal anesthetic gas concentrations.
- During the last 5 minutes of denitrogenation, perform a final 5 minute eyes closed resting EEG/MEG aCPT recording to ensure that any effects anti-emetic administration and denitrogenation may have on brain activity can subsequently be determined and controlled for.
- Compare this third baseline recording to the previous baselines (rest eyes closed without anti-emetic and task eyes closed without anti-emetic) to determine the effects that antiemetic and aCPT have on spontaneous/resting M/EEG. The baselines are referred to as baselines 1, 2 and 3 in the manuscript for rest eyes closed without anti-emetic, task eyes closed without anti-emetic and task eyes closed with anti-emetic, respectively.
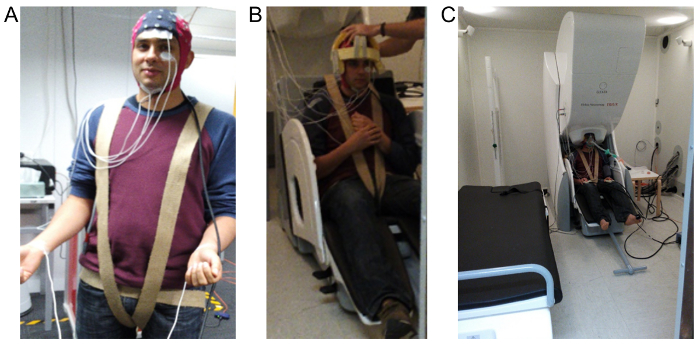
Figure 1: Images demonstrating EEG, EOG, EMG and ECG electrode layout and the overall set up within the MSR. (A) shows the 64-channel MEG compatible cap used to record the EEG, EOG is recorded using the two electrodes shown placed above and below the left eye, EMG is recorded using the two electrodes placed below the jaw and ECG is recorded using two electrodes placed on the wrist. (B) shows the custom-made foam cap and harness used to minimize subject movement during recording. (C) demonstrates the final configuration required for anesthetic administration which includes positioning the head within the MEG and attaching a tight fitting gas-mask. Please click here to view a larger version of this figure.
4. Gas Administration Protocol
NOTE: The gas administration protocol varies slightly depending on the arm of the study.
- Administer Xe at four step-wise increasing levels and N2O at three step-wise increasing levels. The first three gas levels for each gas correspond to equi-MAC-awake levels of 0.25 (level 1), 0.5 (level 2) and 0.75 (level 3) times the MAC-awake concentration. These concentrations are 8%, 16%, 24% and 16%, 32%, 47% concentrations for Xe/O2 and N2O/O2, respectively.
NOTE: The 4th level for Xe corresponds to 1.3 times the MAC-awake concentration. - Choose the 4th gas level for Xe such that 95% of participants are expected to lose consciousness at this level (all subjects studied to date have achieved full loss of responsiveness during the aCPT task). Because of the well documented propensity of N2O to induce nausea and vomiting at high concentrations, do not include a N2O level at a concentration sufficient to induce loss of consciousness in 95% of participants (~75%). Figure 2 summarizes the gas administration profiles.
- Follow the same experimental procedure for all equi-MAC Xe and N2O levels with the exception of 42% Xe/O2, which will require a slightly different methodology (see 4.4. below).
- At the start of each level, inform the subject and anesthetic nurse/clinical observer that gas administration will commence and begin recording the EEG and MEG, signal to the administering anesthesiologist to begin gas administration and start the aCPT task. Gas wash-in then occurs for a period of 10 minutes such that the target end-tidal gas concentration is reached at the end of this period and maintained for 5 minutes (the assumed steady-state phase).
- At the end of this 5 minute steady-state period, perform the wash-out with the administration of 100% O2 over a period of 10 minutes during which end-tidal gas concentration returns to 0.
- Repeat the procedure for the next step gas level.
NOTE: Loss of responsiveness (LOR) for Xe is expected to be achieved in 95% of participants at a concentration of 42% Xe/O261. The administration of this level occurs as for the lower levels until both the anesthetic nurse/clinical observer and the loss of button responses indicate LOR.
- Once LOR is achieved, maintain the Xe gas level for 10 minutes or until the anesthesiologist or anesthetic nurse/clinical observer consider it unsafe to continue after which wash-out with 100% O2 takes places. Instances in which the anesthesiologist may consider it unsafe to continue include frequent pressing of the right button box indicating nausea, glottal noises, signs of emesis such as excessive salivation or swallowing and vaso-vagal reactions.
NOTE: At this highest level, exercise significant caution and set a low clinical threshold for discontinuing Xe gas administration. The authors' experience suggests that this level can be associated with a reduction in swallowing, the build-up of saliva and the appearance of retching-like behavior, that if allowed to continue may foreshadow regurgitation into the mask. Naturally, the consequences of this could include life threatening aspiration. It is also possible that less intense responses may occur at lower gas levels and thus exercise a high level of vigilance during the administration of all step-wise gas levels. In addition to these potential airway issues, be aware of the potential for vasovagal syncope, particularly in the younger male participants. Their age and the temporary fluid and food restrictions are all risk factors62.
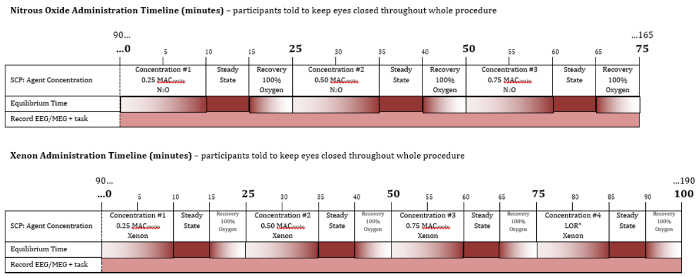
Figure 2: Summary of gas administration profiles for Xe and N 2O. Timeline and gas concentrations during the course of drug administration for N2O (top) and Xe (bottom). The numbers above each timeline indicate the time in minutes since the start of the first gas delivery. Each level of peak equilibrated gas concentration is reached through a 10 minute equilibrating period, followed by a 5 minute steady state during which the peak equilibrated gas concentration is maintained, and then a 10 minute washout. The peak equilibrated gas concentrations increase sequentially over time. Note that the timeline of preparation for the experiment as well as the period after gas administration are not shown. Please click here to view a larger version of this figure.
5. Structural Scan
- Before the MRI, place vitamin E capsules on the participant's head to be used as markers to highlight the digitized fiducial points for the nasal apex and left and right preauricular points. This ensures a better co-registration of the MEG/EEG sensors and MRI brain scans when attempting to relate MEG/EEG source imaging to MRI-based neuroanatomy.
- Obtain a single structural T1-weighted MRI scan, either after the completion of an arm of the study if the participant is feeling well, otherwise ask them to return on a separate day for the structural brain scan.
6. Participant Follow-up
NOTE: The subject is free to leave when accompanied by a friend or relative.
- Upon discharge, ask the participant to complete a truncated version of the 5-Dimensional Altered States of Consciousness Rating Scale (5D-ASC); a questionnaire designed to access individual differences by comparing normal and altered consciousness status by means of a visual analogue scale63,64.
- In addition, ask for the submission of a short narrative of their overall experience during the experiment as well as specific details about level dependent qualitative effects.
- Have both of these documents completed and sent to the researchers 24 hours after each recording session.
7. Data Analysis
NOTE: This section describes basic data analysis at the MEG/EEG sensor level covering the steps involved in generating examples of preprocessed MEG/EEG data, spectral topography, head movements, responsiveness scoring, and auditory evoked responses. The focus of this article is on the illustration of typical examples so that the reader can understand the important features of the recorded data. No intra-individual or group-wise statistical analyses are performed as the principle aim in this analysis section is to detail important pre-processing steps that attest to the quality and integrity of the data collected. No details are provided for the myriad analyses that could be performed on this data55,56 as they fall outside the scope of the description of the method.
- Complete offline data analysis on a desktop computer using appropriate data analysis software and use relevant toolboxes for both EEG and MEG data processing. In the authors' pipeline, use version 20160801 of the Fieldtrip toolbox65 .
- Compute head movement during each MEG recording by first obtaining the continuous head positions as a sequence of quaternion co-ordinates by analyzing the 5 HPI coil signals saved as part of each of the level dependent and baseline MEG recordings. Convert head positions from quaternion into Cartesian co-ordinates.
- Assemble the 6 and 7 recordings for N2O and Xe study arms (baselines 1, 2 and 3, gas levels 1 to 3 or 1 to 4 respectively). Time shift raw EEG relative to MEG data in order to synchronize the two signal types based on a common trigger channel. This form of synchronization arises from the choice of EEG recording system.
NOTE: Many MEG systems contain a built in EEG system that offers very accurate electronic level synchronization of the MEG & EEG, but often have low resolution DAC quantization of 16 bits. For this reason, utilize an external EEG system (see 2.3) having higher 24-bit EEG amplitude resolution to enable a higher tolerance to electrode offset potentials, the measurement of low frequency information and a flat frequency response across all channels. - For all recordings involving gas delivery and aCPT performance, redefine time zero to the commencement of aCPT task/gas delivery.
- Visually inspect raw MEG data and exclude any bad channels from further analysis. Next, filter the data using a temporal signal-space separation algorithm76 implemented in the MEG-system software. The algorithm suppresses sources of magnetic interference outside the sensor array and hence results in a reduction of external or rigid body movement artifacts. Import the output data set into the data analysis software to be used with the magnetometers (102 channels) selected for further processing.
- Band-pass filter the MEG at 2 to 50 Hz and apply line noise filters at 50, 100 and 150 Hz. Visual artifact detection and an automatic artifact detection procedure implemented in the Fieldtrip software allow for the removal of any artifactual elements. Visually inspect any segments containing eye blinks, heart beats or muscular artifacts and exclude from the data, as well as any segments correlated with significant changes in head movement greater than 5 mm (see below).
NOTE: Movements of greater than 5 mm with respect to the beginning of each 5 minute baseline or gas equilibrated period are used to reject continuously acquired MEG data since MEG source imaging typically has a spatial resolution of the order of 5 mm (e.g. for MEG/EEG beamformers55). It is however possible to perform movement compensation of the MEG data66 rather than rejecting data segments correlated with significant head movement, however such methods are beyond the scope of this paper. - As with MEG data, visually inspect the 64-channel raw EEG and exclude any bad channels from further data analysis. Band-pass filter the data using the same frequency ranges as for the MEG. Re-reference the EEG to a common average as is standard for source imaging approaches. Finally, remove any segments containing artifacts contemporaneous with those of the corresponding MEG.
- To visualize the spectral properties of the MEG/EEG data, compute single-sided amplitude spectra along the anterior-posterior midline for the EEG channels FPz, Cz and Oz and for midline frontal, central and occipital MEG magnetometer channels ( Figure 3).
- Calculate the sensor-level topographic map of alpha band (8-13 Hz) power for MEG/EEG, given that strong alpha band changes have been observed previously for N2O and GABAergic anesthetics25,31,67.
- For EEG data, use the FPz channel as the reference to calculate the topographic alpha band power in order to better highlight alpha power changes.
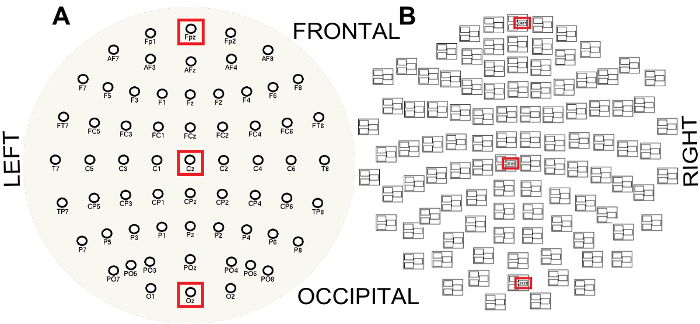
Figure 3: EEG (A) and MEG (B) sensor layouts viewed from the top of the head and flattened into a plane. Note the MEG triplet structure where sensors ending in ###1 are magnetometers and sensors ending in ###2 or ###3 are gradiometers. Red boxes indicate the channels along the anterior-posterior midline used to visualize the spectral properties of the EEG and MEG, FPz (frontal), Cz (central) and Oz (occipital) and frontal, central and occipital magnetometer channels respectively. Please click here to view a larger version of this figure.
- Obtain auditory evoked responses for filtered artifact-free MEG and EEG data for each recording involving the aCPT task. Epoch the signals from -1000 ms to +2000 ms relative to the tone trigger times and average all available artifact free epochs. Take the latency between stimulus trigger generation and delivery of sound to the ear into account, in this case 190.5 ms.
This section utilizes data obtained from one subject in order to demonstrate the typical features of the simultaneous recordings and the potential of such information to contribute a better understanding of anesthetic induced altered states of consciousness. To simplify the exposition, results are shown for i) recordings of the post-anti-emetic administration baseline (baseline 3), ii) 0.75 equi-MAC-awake peak gas concentrations (level 3) of N2O (47%) and Xe (24%), and iii) Xe peak gas concentration of 42% (level 4). Levels 3 and 4 were chosen as they are the highest steady-state levels considered for N2O and Xe, respectively. Moreover, level 4 Xe involves a clear loss of responsiveness, a state not typically achievable for N2O.
In order to clearly illustrate the extent of head movement the absolute positions of all 5 HPI coils are shown as a function of time during multiple recordings. Figure 4 clearly demonstrates that the steps followed to ensure limited movement during the scans are associated with acceptable levels of head and body movement despite pharmacological intervention. A notable example of extensive head movement can be seen in Figure 4(ii) between 20-25 minutes (during the washout period) when large head movement was recorded. Such periods are visually detected and removed from the data. The protocol ensures that stable end-tidal gas concentrations at all levels can be easily and readily achieved (see Figure 4), with subject responsiveness robustly assessed using the aCPT task. Figures 4(ii) and 4(iv) clearly show such assessed reductions in responsiveness during the 5 minute steady state phases for both xenon and nitrous oxide. Figure 4(v) indicates loss of responsiveness (0% accuracy) during the steady state period under 42% Xe administration, as expected.
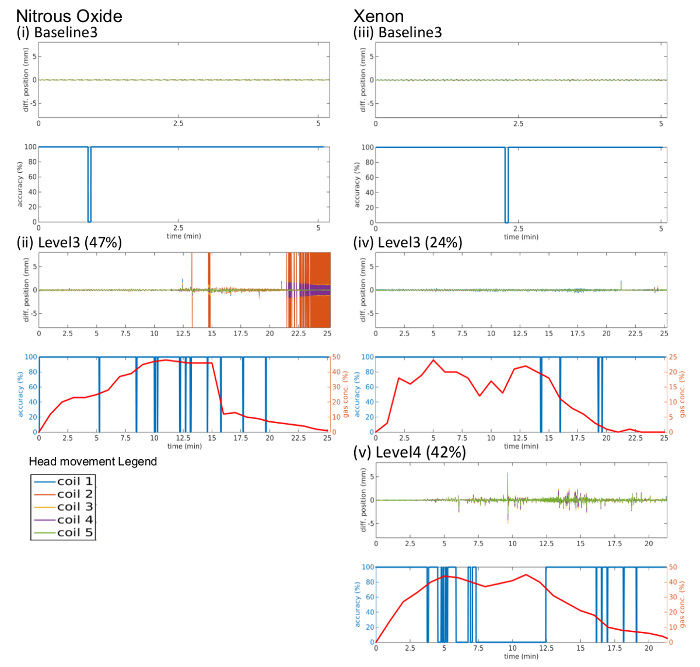
Figure 4: Examples of head movement, gas concentration and aCPT accuracy time series from one participant for (i) baseline 3 (post antiemetic) prior to N2O administration, (ii) 47% N2O (level 3), (iii) baseline 3 prior to Xe administration, (iv) 24% Xe (level 3), and (v) 42% Xe (level 4). Each sub-figure shows absolute movement (top) of the 5 head coils (legend below (ii) indicates coils) and gas concentration (bottom, red) and aCPT accuracy (bottom, blue) as a function of time in minutes. Please click here to view a larger version of this figure.
Examples of the filtered artifact-free MEG and EEG data along the anterior-posterior mid-line for the same subject as in figure 4 are shown for time aligned 10 second segments for N2O and Xe in Figure 5. Baseline 3 (post antiemetic) for both Xe and N2O shows strong alpha oscillations in the occipital channels (Oz for EEG and an occipital magnetometer channel for MEG). As the anesthetic level increases for level 3 N2O (47% peak gas) total signal power is reduced, with reductions in alpha band power particularly evident. In contrast alpha activity, in response to Xe administration is not significantly reduced until level 4 (42% peak gas). In contrast to N2O increasing Xe concentrations are more clearly associated with an increase in the amplitude of delta (0 – 4 Hz) and theta (4 – 8 Hz) band activity, being especially clear in the central site during 42% administration (level 4) in the MEG.
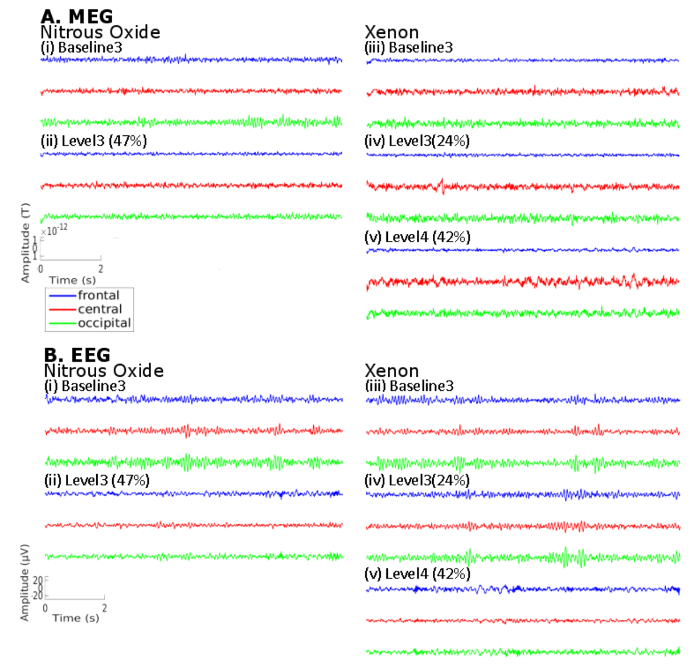
Figure 5: Example of a time aligned 10 second window of filtered artifact-free (A) MEG and (B) EEG data for the same subject in Figure 4 for the cases of (i) baseline 3 (post antiemetic) prior to N2O administration, (ii) 47% N2O (level 3), (iii) baseline 3 (post antiemetic) prior to Xe administration, (iv) 24% Xe (level 3), (v) 42% Xe (level 4). For 24% Xe and 47% N2O, the time period selected was a fragment of the 5 minute steady state while for 42% Xe, the epoch of data selected was during the period of loss of responsiveness, as indicated by the subject's aCPT response. Frontal (blue), central (red) and occipital (green) correspond to the respective MEG magnetometer and EEG channels. Please click here to view a larger version of this figure.
The changes in signal power observed in Figure 5 are further detailed in single-sided amplitude spectra of the same signals in Figure 6. While there emerge a range of observed changes in power when transitioning from baseline to gas, the most significant changes appear to be the gradual attenuation of the strong baseline alpha band (8-13 Hz) power, observed in the occipital electrodes, with increasing gas concentrations. This is complemented with increasing low frequency delta and theta band activity.
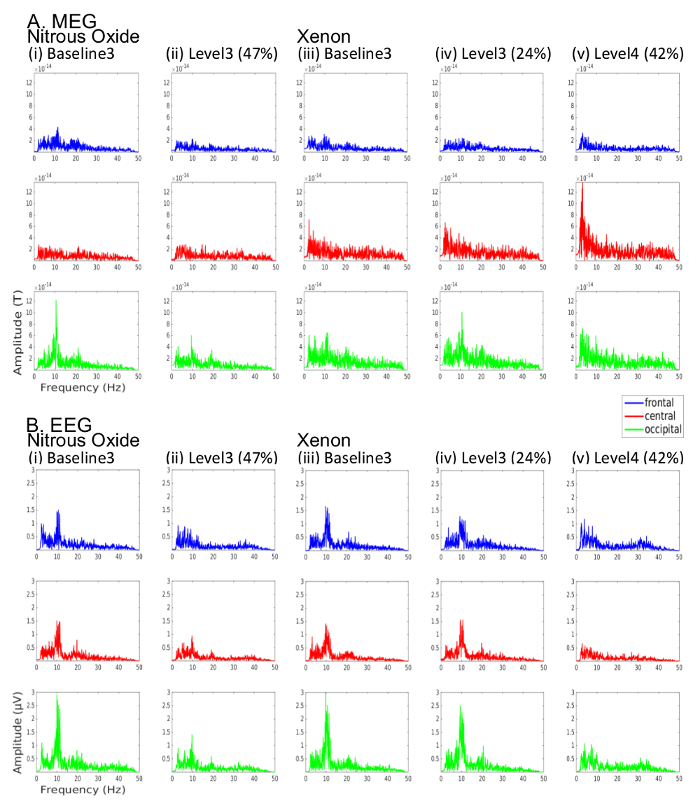
Figure 6: Amplitude spectra for the same (A) MEG and (B) EEG data shown in Figure 5 for the cases of (i) baseline 3 (post antiemetic) prior to N2O administration, (ii) 47% N2O (level 3), (iii) baseline 3 (post antiemetic) prior to Xe administration, (iv) 24% Xe (level 3), (v) 42% Xe (level 4). Frontal (blue), central (red) and occipital (green) channels correspond to respective MEG magnetometer and EEG channels. Please click here to view a larger version of this figure.
Figure 7 illustrates an example of the topographic changes in alpha band power linked to increases in Xe and N2O gas concentration. Note the clear attenuation of posterior alpha power with increases in Xe and N2O, consistent with changes observed previously for N2O and GABAergic anesthetics25,31,67.
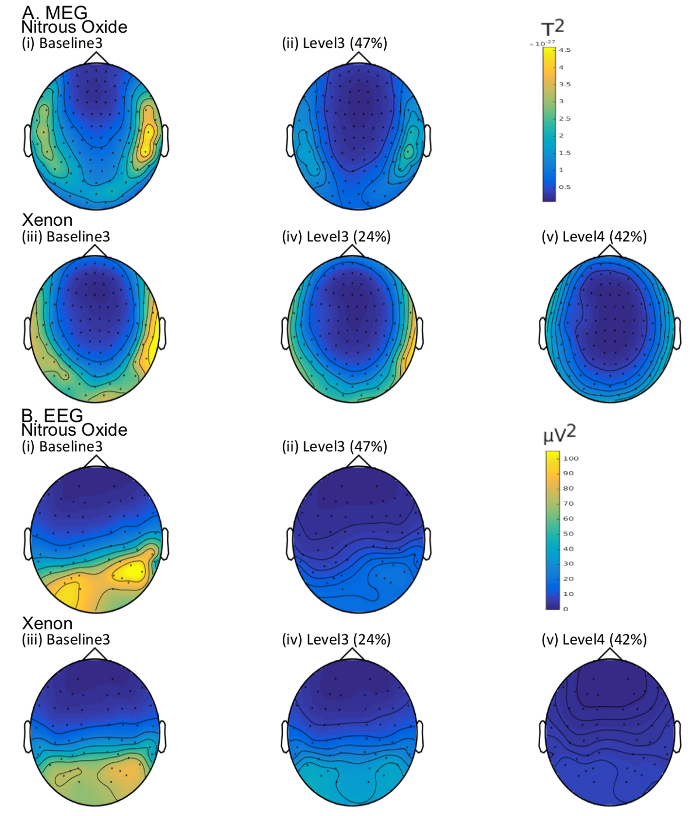
Figure 7: Topographic alpha (8-13 Hz) band power in the (A) MEG (magnetometers only) and (B) EEG for the same subject as in Figures 5 and 6 for the cases of (i) baseline 3 (post antiemetic) prior to N2O administration, (ii) 47% N2O (level 3), (iii) baseline 3 (post antiemetic) prior to Xe administration, (iv) 24% Xe (level 3), (v) 42% Xe (level 4). Please click here to view a larger version of this figure.
Finally, Figure 8 illustrates example sensor-level MEG and EEG auditory evoked responses obtained with the protocol and aCPT task for the same subject as in Figures 5-7. It can be noted that increases in in Xe and N2O gas concentration lead to a weakening of the first response peak and also to the delay, attenuation or disappearance of later response peaks, especially during loss of responsiveness for Xe level 4 (42%).
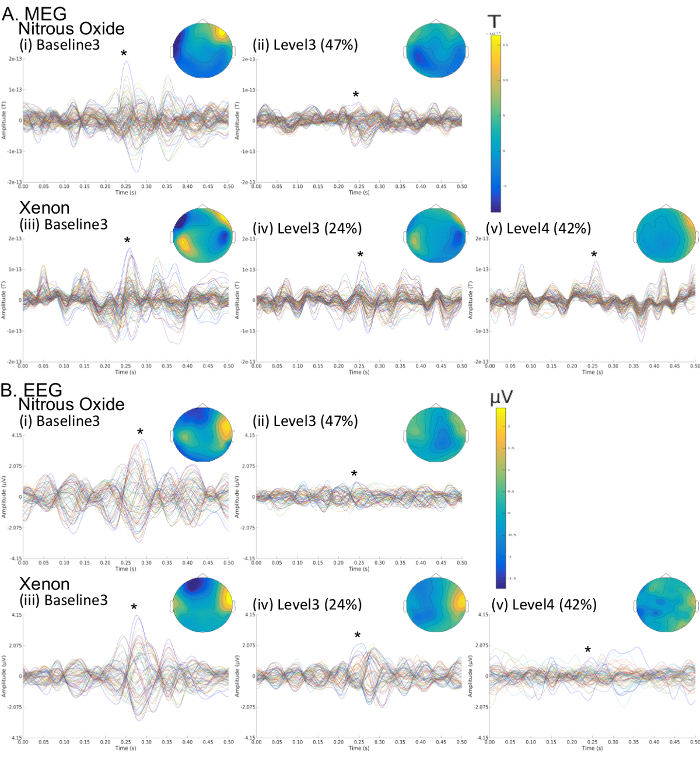
Figure 8: Sensor-level auditory evoked responses for the (A) MEG and (B) EEG for the same subject as in Figures 5-7 for the cases of (i) baseline 3 (post antiemetic) prior to N2O administration, (ii) 47% N2O (level 3), (iii) baseline 3 (post antiemetic) prior to Xe administration, (iv) 24% Xe (level 3), (v) 42% Xe (level 4). Colored butterfly plots correspond to channel-wise time ensemble responses. For each butterfly plot the topographic map corresponds to the time of peak response. Please click here to view a larger version of this figure.
