The uniqueness of this method rests in its adaptation of the gavaging technique to the size and frailty of a neonatal mouse. The previous section described the important steps in carrying out a successful gavage procedure on a DOL 2 mouse. To establish a good quantification scale, a standard curve was generated using pure LP DNA with three technical replicates (Figure 2). The standard curve provided a dynamic range of detection of the LP DNA using the primers. The dynamic range was between 7 and 28 cycles where a range of 101 to 107 copies of LP DNA was detected. The steady slope of the standard curve represented the efficiency and scalability of the reaction.
The procedure of IE gavage has been used in adult mice with relative ease. However, the upper gastrointestinal tract of a neonatal mouse is fragile and required calibrated movements of the gavage needle during the procedure. Repeated gavages could increase the chances of intra-esophageal irritation, injury and failure or rejection by the dam due to the handling. Thus, two different gavaging schedules were tested and the intestinal colonization was quantified using DNA from whole intestine homogenates. Mice were gavaged from DOL 2 through DOL 8 with probiotic administered every day or every two days (Figure 3). Each sample contained one technical replicate and every condition had at least two biological replicates. The pups gavaged every day with 7 doses had around 103 copies of LP whereas the pups gavaged every two days with 4 doses had around 105 copies. The consistency of results between the replicates add credit to the precision of technique. There was more LP detected in intestines of pups gavaged every two days in comparison with pups that were gavaged every day. Given this, subsequent experiments were set up with a gavage schedule of every other day as it also reduces the stress for the pups.
It is important to avoid intra-litter probiotic cross contamination when working with probiotics. The microbiome of littermates was expected to be similar as they share the same mother and nesting environment. This proves a problem for probiotic studies if the treatment and control conditions were present within the same litter as the probiotic organism has the potential to become a part of the microbiota ("colonization spread'). To determine if a probiotic will contaminate and colonize untreated littermates, half of a litter was gavaged as above and the intestines were collected for qPCR. Intestinal qPCR analysis of DOL 10 mice showed expected amplification of LP DNA in the gavaged mice but also, to a lesser degree in the non-gavaged littermates (Figure 4). The intestines of the same DOL mice from an untreated cage showed no amplification or minimal amplification at cycles greater than 32. This provided evidence for the communal sharing of the microbiome within a litter in a cage. Thus, for experiments with probiotics the treatment groups should be separated by cages to control for variability through cross contamination. The use of foster dams can be considered if an experiment is to be set up within a litter setting, but confounding effects like diminished care from the foster dam and rejection should be evaluated and optimized for. When mice gavaged until DOL 8 were left untreated for six days and the intestinal DNA was analysed at DOL 14, approximately 10 copies of LP were found (Figure 5). Thus, the colonization of LP was found to be transient and the detectable population diminished over time.
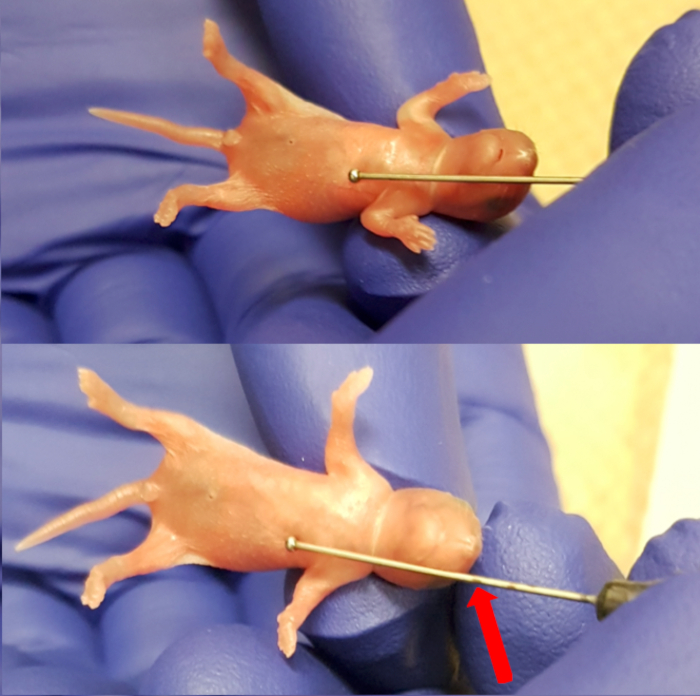
Figure 1. Measuring the length between the xiphoid process (lower end of the sternum) and the snout to make maximum insertion marking for the needle. Please click here to view a larger version of this figure.
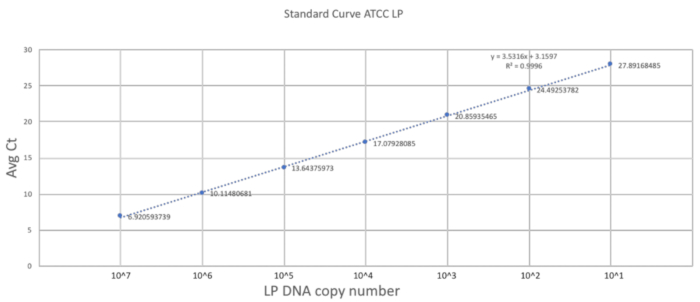
Figure 2. Standard curve established using LP primers and ATCC LP DNA. A serial dilution of the ATCC LP DNA was made to establish the dynamic detectable range for the primers used in the study. Please click here to view a larger version of this figure.
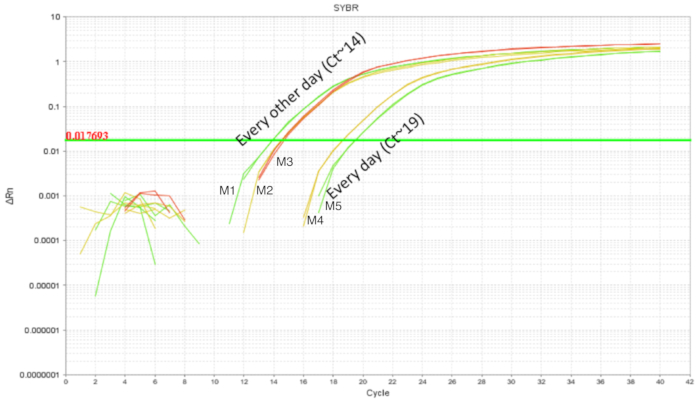
Figure 3. LP amplification of intestinal DNA from DOL 10 pups treated between DOL 2 and DOL 8 in scheduled gavages every day (7 doses) and every other day (4 doses). Gavaging every other day showed higher intestinal LP in comparison with gavaging every day. Please click here to view a larger version of this figure.
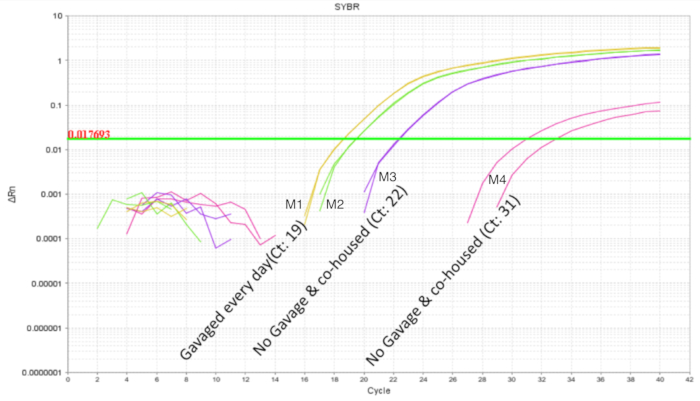
Figure 4. LP amplification of intestinal DNA from DOL 10 pups with 2 treated and 2 untreated in a litter of 4 pups. The gavage was between DOL 2 and DOL 8 in scheduled gavages every day (7 doses). The two probiotic treated pups show the expected amplification profile. The untreated pups show variable amplification of LP indicating communal sharing of the probiotic organism within a litter. Please click here to view a larger version of this figure.
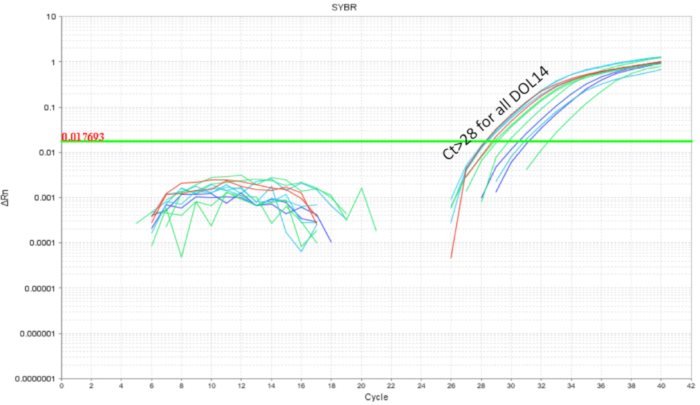
Figure 5. LP amplification of intestinal DNA from DOL 14 pups treated between DOL 2 and DOL 8 in scheduled gavages every day (7 doses) and every other day (4 doses). The LP load drops below cycle 28 indicating clearance of LP over the course of 6 days post last probiotic gavage. Please click here to view a larger version of this figure.
| Step | Temperature | Time |
| 1 | 50 °C | 2 minutes |
| 2 | 95 °C | 3 minutes |
| 3 | 95 °C | 30 seconds |
| 4 | 58 °C | 30 seconds |
| 5 | 72 °C | 30 seconds |
Table 1. qPCR amplification conditions. The temperature and number of cycle conditions for the PCR reaction.
| Target | 16S-23S intergenic spacer region |
| Expected fragment size | 144 bp |
| Primer Tm | 58˚C |
| Forward primer (FP) | Lpn-1: TGG ATC ACC TCC TTT CTA AGG AAT |
| Reverse primer (RP) | Lpn-2: TGT TCT CGG TTT CAT TAT GAA AAA ATA |
Table 2. Details of components of the qPCR reaction. The details on the primers, their annealing temperature and expected fragment size in the PCR reaction.
| Concentration | 10 µL reaction | 20 µL reaction | |
| Template DNA | 200 pg/µL | 1 µL | 1 µL |
| SYBR Master Mix | – | 5 µL | 10 µL |
| FP | 10 µM | 0.3 µL | 0.6 µL |
| RP | 10 µM | 0.3 µL | 0.6 µL |
| dH2O | – | 3.4 µL | 8.8 µL |
Table 3. Per reaction volumes and concentrations. The concentration of reagents and volumes for reactions.
