Heart rate and blood pressure were monitored during surgery. Mean heart rate was 193/min in rabbits and 196/min in rats. The rabbits' body weight ranged 3.05-4.18 kg, and the rats weighed 335-690 g.
We were able to perform FVA in eight out of ten rabbits (Figure 1). Four aneurysm examinations in two rabbits were not recorded with the camera due to technical difficulties. No technical difficulties involving FVA in rats were reported. However, FVA could not be performed in one rat due to difficulties puncturing the femoral vein.
Of 16 aneurysms in eight rabbits, two aneurysms showed persistent perfusion of the parent artery (confirmed macroscopically) (see Table 1) while FVA identified five cases with residual perfusion. 14 rabbit aneurysms showed no residual perfusion macroscopically, however 11 (79%) were subsequently detected using FVA. Residual perfusion was observed macroscopically in 25 of 48 rats (Table 1), and the other 23 rats showed no macroscopic signs of residual perfusion (Figure 2). 22 of those 23 aneurysms were then confirmed using FVA (96%). Altogether, 25 of 27 cases could be confirmed, resulting in a positive predictive value of 92.6%, a sensitivity rate of 100% and specificity of 94.1%. (Table 2).
In summary, 25 aneurysms showed residual perfusion, 53 parent arteries were patent and 11 were occluded as confirmed macroscopically and on video angiography. There were only minor complications associated with FVA in rabbits; such as perforation of marginal ear vein during catheterization. No further adverse events were experienced. No mortality and no morbidity due to FVA was reported.
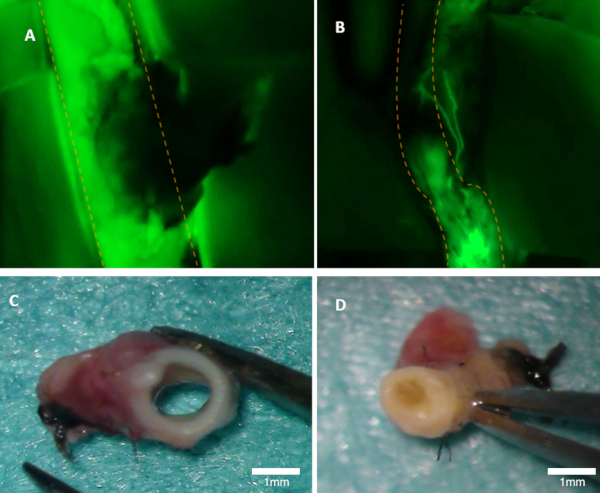
Figure 1: Visualizing patency in a rabbit. (A) Patency of the parent artery is clearly visible on the fluorescence image (green emission from fluorescein are seen). (B) This artery is occluded (fluorescence image). Both arteries were inspected macroscopically (C–D). Panel (C) shows in the artery from panel A; the lumen is open. Panel (D) shows artery from panel B where occlusion can be seen macroscopically. Orange dotted lines mark the borders of the parent artery. Please click here to view a larger version of this figure.
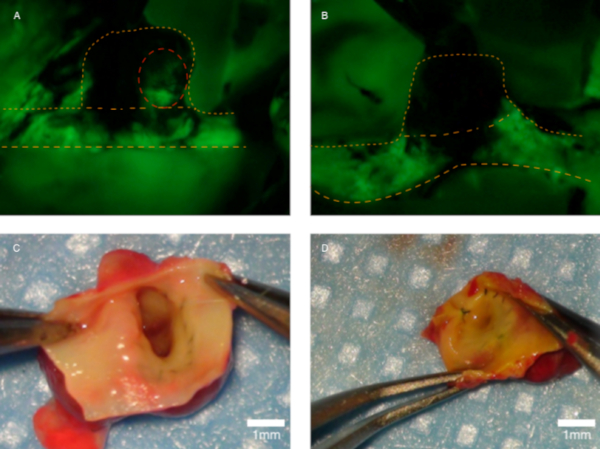
Figure 2: Visualizing perfusion in a rat. (A) This panel shows a residually perfused aneurysm (red dotted line marks the residual perfusion). (B) No perfusion can be detected. Panel (C) shows the artery from panel A during macroscopic scrutiny; the aneurysm orifice is open. (D) Macroscopic view of the neointima on an occluded aneurysm. Orange dotted lines mark the parent artery and the aneurysm’ dome. Panels (A) and (B) are fluorescence-only images and the green color shows fluorescein emission. Please click here to view a larger version of this figure.
| Patency/Residual Perfusion | ||||
| Macroscopical + | Macroscopical – | Fluorescein + | Fluorescein – | |
| Rabbits | 2 | 14 | 5 | 11 |
| Rats | 23 | 25 | 22 | 21 |
| Total | 25 | 39 | 27 | 32 |
Table 1: Patency testing. Patency of parent artery was only tested in rabbits and is illustrated here. Fluorescein detected more patencies of parent arteries than macroscopical evaluation. (All rats in this setting had an open parent artery, as aneurysms were sutured on the abdominal aorta.) The patency of aneurysms was tested in rats only. Twenty-two of 23 macroscopically detected patencies were confirmed using FVA. Twenty-one of 25 showed no patency on FVA.
| Macroscopic positive | Macroscopic negative | total | |
| Fluorescein positive | 25 | 2 | 27 |
| Fluorescein negative | 0 | 32 | 32 |
| total | 25 | 34 |
Table 2: Two-by-two table used to calculate specificity and sensitivity of FVA.
