The design of the glass molds are an innovative and original idea, the use of which allowed us to set up the model in a consistent fashion with minimal/no issues with contamination. The molds were prepared by a glass blower at the University of Sheffield based on a design (Figure 1A). The experimental setup maintains the convex shape of the cornea and holds bacteria on the top of the epithelium where infection takes place (Figure 1B).
Porcine corneas usually swell after few days in medium. This is normal and we found that there was no significant difference between corneas with and without addition of dextran, which is usually added to prevent swelling of the cornea (Figure 1H). The corneas are typically wounded to help the bacteria penetrate the epithelium. Although there was no significant difference in the progress of infection between wounded (cut) and unwounded (uncut) corneas, we noticed more variations between replicates in uncut corneas (Figure 1C). Washing the corneas twice with PBS removes excess bacteria that did not attach to the epithelium. There was a significant difference in CFU between washed and unwashed porcine corneas infected with P. aeruginosa PAO1 for 24 hours (Figure 1D). There was no significant difference in CFU counts between porcine and rabbit corneas infected with PA14 and PAO1 (Figure 1E,1F). The results for both models were reproducible. After 24 hours, the cornea infected with either Pseudomonas strain always develop opacity and the cut area becomes more visible and open in comparison to the uninfected cornea (Figure 1G).
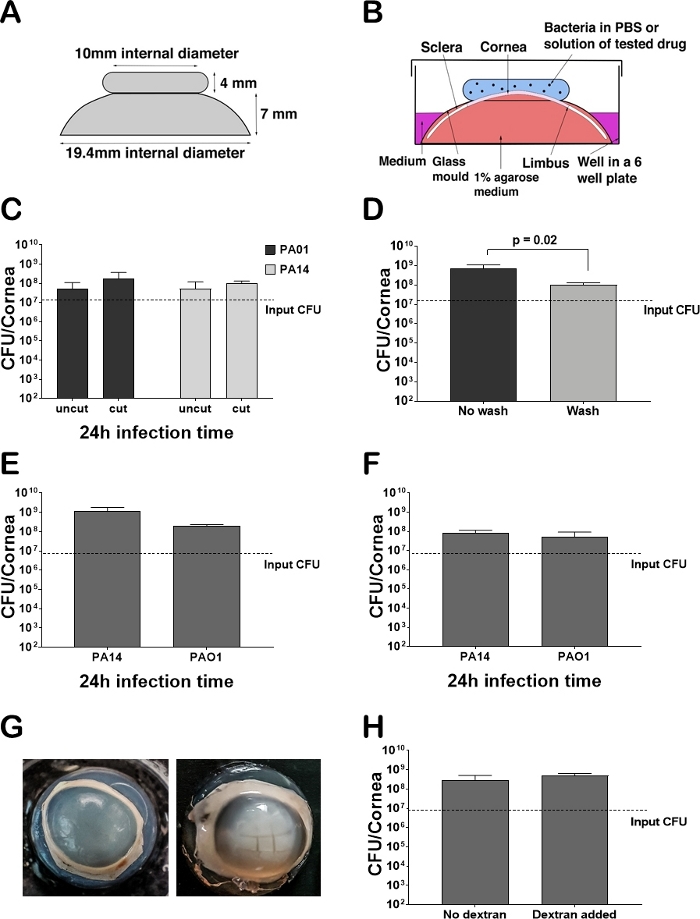
Figure 1: Ex vivo cornea infected with Pseudomonas aeruginosa. (A) Schematic picture of a glass mold used for maintaining the shape of the cornea and facilitating the introduction of bacteria and treatments. The thickness of the glass molds is 1.5 mm and is the same as the thickness of test tubes made from borosilicate glass. (B) Schematic picture of the experimental set up. (C) Testing the effect of wounding on the final CFU count after homogenization. Uncut (n = 16) and cut (n = 28) corneas were infected with P. aeruginosa PAO1 and P. aeruginosa PA14 for 24 hours. The corneas were washed with 1 mL of PBS before homogenization. Error bars indicate standard deviation. (D) Testing the effect of washing corneas with 2 x 1 mL of PBS (n = 6) and not washing (n = 6) on the final CFU count after infection with P. aeruginosa PAO1 for 24 hours. Error bars indicate standard deviation. (E) Final CFU count in porcine corneas infected with P. aeruginosa PAO1 and P. aeruginosa PA14 for 24 hours (n = 10). Corneas were washed and cut. Error bars indicate standard deviation. (F) Final CFU count in rabbit corneas infected with P. aeruginosa PAO1 and P. aeruginosa PA14 for 24 hours (n = 6). Corneas were washed and cut. Error bars indicate standard deviation. (G) Pictures of ex vivo porcine corneas infected with P. aeruginosa PAO1 for 24 hours. The control was wounded but no bacteria were added. The infected corneas were wounded and 107 CFU were added to the cut side. No CFU were recovered from the control cornea. (H) Final CFU recovered after 24 hours of infection with P. aeruginosa PAO1 from corneas treated with dextran (n = 2) and those without dextran (n = 9). Corneas were washed and cut. Error bars indicate standard deviation. Please click here to view a larger version of this figure.
