Ten subjects (five males and five females) from the Department of Rehabilitation Medicine at Guangzhou Medical University were recruited in this pilot study. The participants had similar baseline characteristics, such as age (mean age: male 21.00 ± 1.58 years; female 21.20 ± 0.45 years) and physical fitness [sports activity and body mass index (BMI)]. There were no significant differences in age, height, or BMI between the male and female groups. Moreover, for the spirometry, the female group showed lower FVC, lowered forced expiratory volume in 1 s (FEV1), lower MVV, and lowered peak expiratory flow (PEF) compared with the male group (Table 1).
The results of CPET under different conditions (mask-on and mask-off) are depicted in Table 2. For exercise tolerance and cardiac function, compared to the mask-off condition, both male and female groups during the mask-on condition showed a significant decrease in anaerobic threshold per kilogram, i.e., VO2/kg (LT), and oxygen pulse, i.e., O2/HR (peak), whereas no significant differences in oxygen uptake related to work rate, i.e., ΔVO2/ΔWR and HR (rest). Moreover, the male group also showed a significant decrease in HR (rest), and the female group showed a significant decrease in peak oxygen uptake per kilogram, i.e., VO2/kg (peak) during the mask-on condition. For ventilatory function, compared to mask-off condition, both male and female groups during mask-on condition showed a significant decrease in tidal volume, i.e., VT (peak), but no differences were found in the breathing reserve in percentage, i.e., BR%. For gas exchange, compared with the mask-off condition, both male and female groups during the mask-on condition showed a significant decrease in the ventilation, i.e., VE (peak), but no differences were found in VE/VCO2. For the total CPET performance, both male and female groups showed no difference in Loadmax, RPE scale, and Borg's scale.
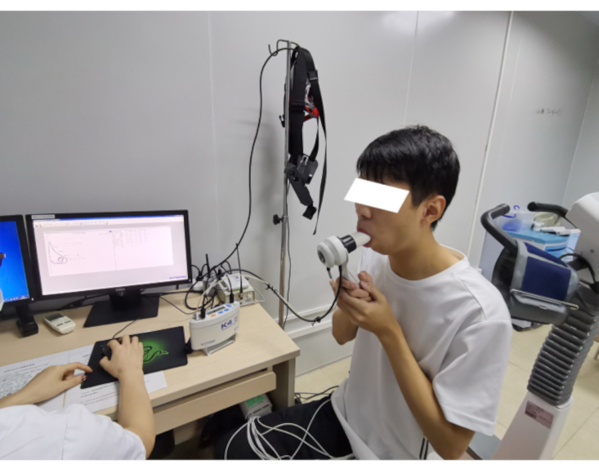
Figure 1: Diagram for spirometry. Please click here to view a larger version of this figure.
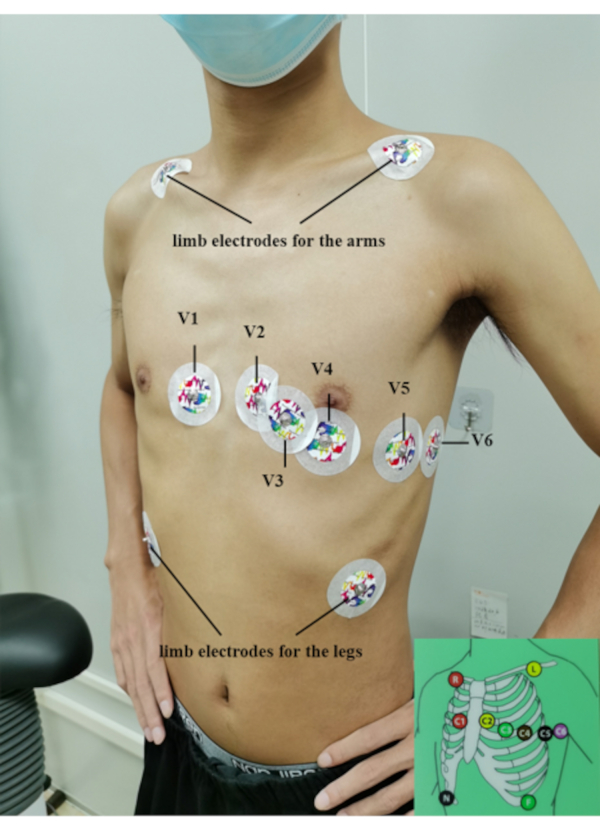
Figure 2: The ECG electrode settings. Please click here to view a larger version of this figure.
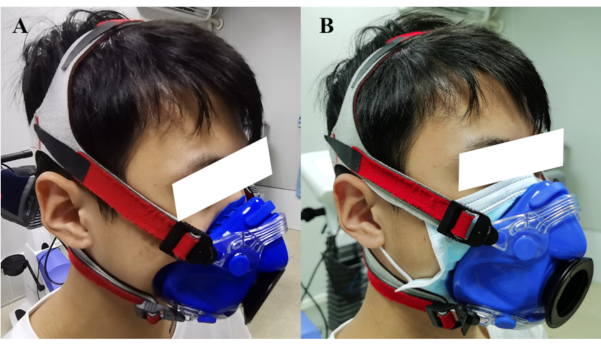
Figure 3: Fitting of mask. (A) shows the mask-off condition. (B) shows the mask-on condition. Please click here to view a larger version of this figure.
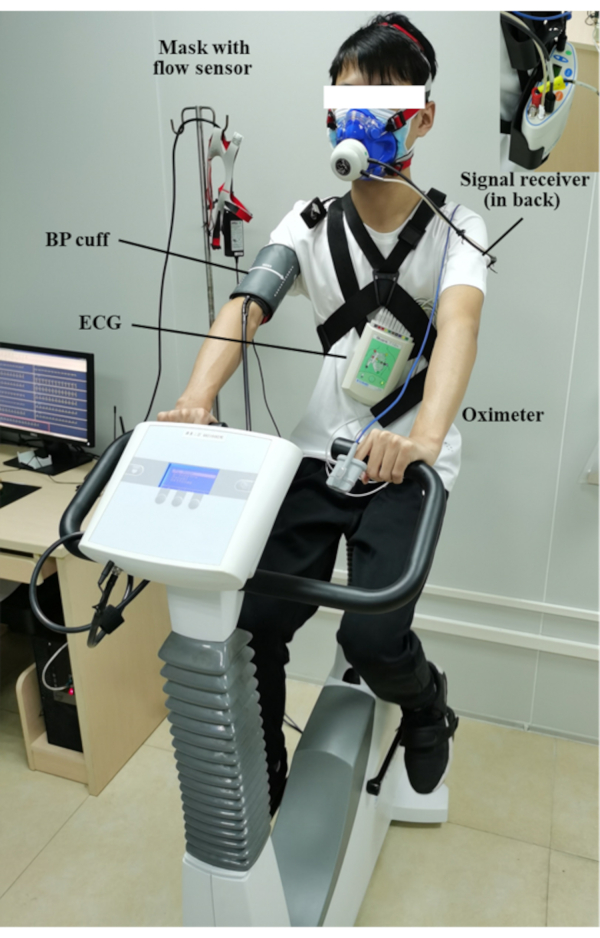
Figure 4: Diagram for CPET settings. Please click here to view a larger version of this figure.
| Parameters | Unit | Male group | Female group | P value | ||
| (n=5) | (n=5) | |||||
| Age | years | 21.00±1.58 | 21.20±0.45 | 0.792 | ||
| Alto | cm | 172.60±4.45 | 157.00±3.80 | <0.001 | ||
| Weight | kg | 59.40±3.50 | 49.10±2.49 | 0.001 | ||
| BMI | kg/m2 | 19.94±0.80 | 19.91±0.41 | 0.955 | ||
| Spirometry | ||||||
| FVC | L | 4.43±0.26 | 3.13±0.31 | <0.001 | ||
| FEV1 | L | 3.70±0.24 | 2.78±0.23 | <0.001 | ||
| MVV | L/min | 131.78±12.42 | 76.38±13.57 | <0.001 | ||
| PEF | L/s | 8.96±1.11 | 5.95±1.41 | 0.060 | ||
| Notes: Significant results are indicated in bold. FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; MVV, maximum voluntary ventilation. PEF, peak expiratory flow; L, liter; s, second. | ||||||
Table 1: Baseline characteristics and spirometry results.
| Parameters | Unit | Male group | Female group | |||||
| Mask-off | Mask-on | P value | Mask-off | Mask-on | P value | |||
| Exercise tolerance and cardiac function | ||||||||
| VO2/kg (peak) | (mL/min)/kg | 36.21±3.8 | 28.46±4.96 | 0.063 | 26.86±4.86 | 22.96±5.45 | 0.002 | |
| VO2/kg (LT) | (mL/min)/kg | 22.66±2.26 | 19.74±2.23 | <0.001 | 18.48±2.89 | 14.28±2.6 | 0.026 | |
| O2/HR (peak) | ratio | 12.14±0.63 | 10.02±1.7 | 0.028 | 7.96±0.87 | 6.9±1.15 | 0.004 | |
| ΔVO2/ΔWR | mL/(min*W) | 8.96±0.3 | 7.52±1.4 | 0.083 | 8.66±0.51 | 7.86±1.17 | 0.217 | |
| HR (rest) | bpm | 85.2±16.08 | 77.6±7.09 | 0.244 | 84±10.56 | 83.4±5.94 | 1.000 | |
| HR (peak) | bpm | 177.6±10.5 | 170.6±11.33 | 0.007 | 162.6±17.67 | 162.6±21.72 | 1.000 | |
| Ventilatory function | ||||||||
| VT (peak) | L/min | 2.23±0.31 | 1.9±0.4 | 0.004 | 1.33±0.28 | 1.21±0.28 | 0.018 | |
| BR% | % | 50.2±8.14 | 56.6±10.53 | 0.086 | 53.6±8.91 | 57.8±10.94 | 0.086 | |
| Gas exchange | ||||||||
| VE/VCO2 | ratio | 28.64±3.42 | 30.44±5.26 | 0.379 | 32.34±3.63 | 31.54±4.3 | 0.616 | |
| VE (peak) | L | 74±13.36 | 62.6±15.35 | 0.022 | 51.8±13.35 | 43.22±11.72 | 0.042 | |
| CPET performance | ||||||||
| Loadmax | ||||||||
| Loadmax (LT) | watts | 98.2±18.38 | 102±11.81 | 0.438 | 56.8±11.48 | 50.8±9.96 | 0.104 | |
| Loadmax (RC) | watts | 155.6±22.47 | 159±24.37 | 0.223 | 87.8±18.47 | 86.2±19.6 | 0.816 | |
| Loadmax (Peak) | watts | 187±28.15 | 184.8±26.81 | 0.604 | 107.6±29.25 | 105.6±30 | 0.116 | |
| RPE scale | scores | 17.8±0.84 | 17±1.73 | 0.371 | 17.4±0.89 | 17.2±1.3 | 1.000 | |
| Borg’s scale | scores | 4.2±0.84 | 4.8±1.64 | 0.468 | 4.8±0.45 | 4.8±0.84 | 1.000 | |
| Notes: Significant results are indicated in bold. VO2/kg (peak), peak oxygen uptake per kilogram; VO2/kg (LT), anaerobic threshold per kilogram; O2/HR, oxygen pulse; ΔVO2/ΔWR, oxygen uptake related to work rate; BR%, breathing reserve in percentage; VE, ventilation; VT, tidal volume; bpm, beat per minute. RPE scalse, Rating of Perceived Exertion scale; L, liter; min, minute. | ||||||||
Table 2: Results of the CPET in healthy young subjects wearing a surgical mask (mask-on) and not wearing a surgical mask (mask-off) depicted as mean ± standard deviation.
