Cohort demographics
Ten consecutive patients underwent the Pro-LLIF procedure from August 2020 to February 2021. The eligibility criteria for this procedure were ages 18 and older and symptomatic degenerative spondylosis with spinal instability (spondylolisthesis or degenerative scoliosis) from L2 to L5, requiring interbody fusion. Per the institution's standard of care, all patients had trialed and failed a course of conservative management. The exclusion criteria were patients excluded from operative intervention based on their medical inability to tolerate surgery. In addition, in patients with unfavorable anatomies, especially if the L4-5 disc level is caudal to the top of the iliac crest, it would be difficult to use the Pro-LLIF approach. All operations were performed by the same neurosurgeon (Y.L.).
The initial Pro-LLIF cohort comprised eight female and two male patients. The mean age at the time of surgery was 66 years, with individual ages ranging from 41 to 77 years. Eight patients were current or former smokers, and five patients met the Center for Disease Control's definition of obesity (BMI > 30).
Spondylolisthesis was the most common spinal disease amongst this cohort (five patients). The most common indication for surgery was radiculopathy with low back pain (six patients), followed by radiculopathy alone (three patients). Four patients had undergone prior fusion procedures.
Operative characteristics
The majority of the patients in this cohort (60%) underwent one level of Pro-LLIF (Table 1). The mean total operative time for the Pro-LLIF procedure was 4.5 h (median 4.1 h, range 3.2-6.9 h). The total time under anesthesia averaged 6.5 h (median 5.9 h, range 4.2-9.7 h). The average estimated blood loss during the Pro-LLIF procedure was 240 mL (range 50-650 mL).
Preoperative and postoperative magnetic resonance images (MRIs) of the lumbar spine were used to evaluate the changes in foraminal height, segmental lordosis, lumbar lordosis, and disc height after undergoing Pro-LLIF (Table 2). For some patients, the foraminal height or lumbar lordosis improvement is limited, which might be due to the significant disc space and facet joint stiffness in those patients.
Hospital course, length of stay, and dispensation
Pro-LLIF patients experienced an average length of stay of 3.5 days. One patient required early reoperation to recover a retained surgical drain in the posterior incision. No neurological injury or subsidence was reported for any patient in the immediate postoperative period. Six of the ten patients were discharged to home; the remaining four patients were discharged to rehabilitation facilities.
Follow-up and postoperative clinical evaluation
One-month follow-up data were available for all ten patients. The Odom Criteria's 4-point rating scale was adapted to assess Pro-LLIF surgical outcomes (Table 3). At one month, three patients met the criteria for an "Excellent" rating, and six patients reported symptoms consistent with a "Good" rating. One patient reported similar symptoms post-ProLLIF, earning the patient an Odom rating of "Poor." That patient was a complex lumbar deformity patient who has failed multiple surgeries in the past with the development of severe left leg pain following a previous lumbar fusion surgery at another hospital.
Comparison with a propensity score-matched cohort analysis
Retrospective data were also collected on patients who had undergone oblique lateral interbody fusion (OLIF) procedures at the same institution by the same senior neurosurgeon. Using propensity-score matching, 10 OLIF patients were identified who had undergone comparable levels of lateral interbody fusion and decompression as the Pro-LLIF patients. Student's two-sided, unpaired t-tests with Bonferroni multiple-comparison correction were used to compare the quantitative outcome measures between the Pro-LLIF and OLIF groups. No significant differences in total operative time, total anesthesia time, lengths of stay, and estimated blood loss were identified between the Pro-LLIF and OLIF patients (Figure 5).
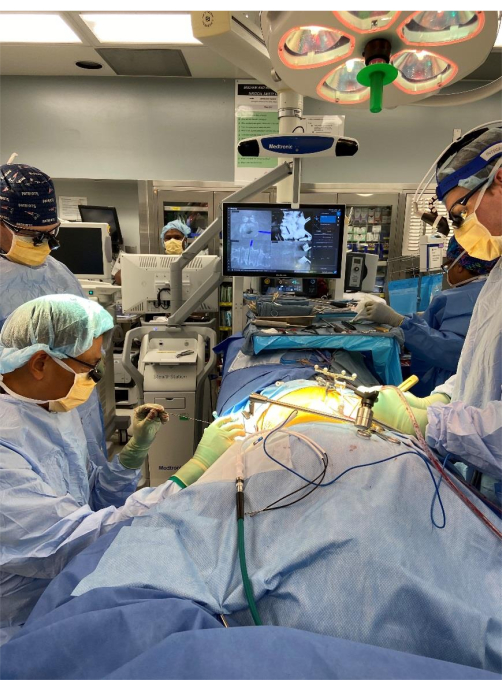
Figure 1: Intraoperative view of single-position pro-LLIF procedure, showing the setup, air-planing of the operative table, and intra-operative navigation and two surgeons performing the lateral and the posterior portions of the surgery simultaneously. Abbreviation: pro-LLIF = prone lateral lumbar interbody fusion. Please click here to view a larger version of this figure.
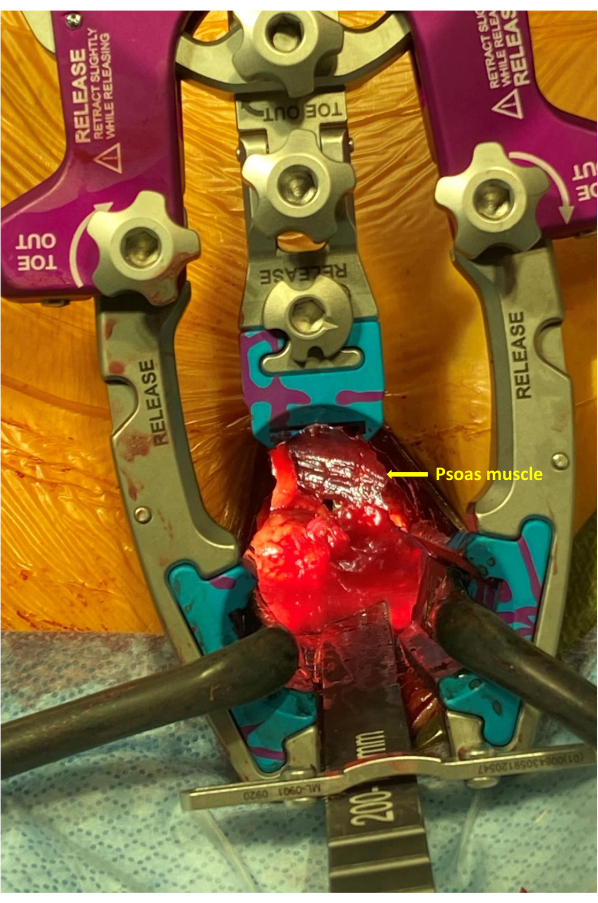
Figure 2: Intra-operative close-up view showing the placement of the expandable retractor system superficial to the psoas muscle in the retroperitoneal space, providing a clear view for direct psoas dissection. Please click here to view a larger version of this figure.
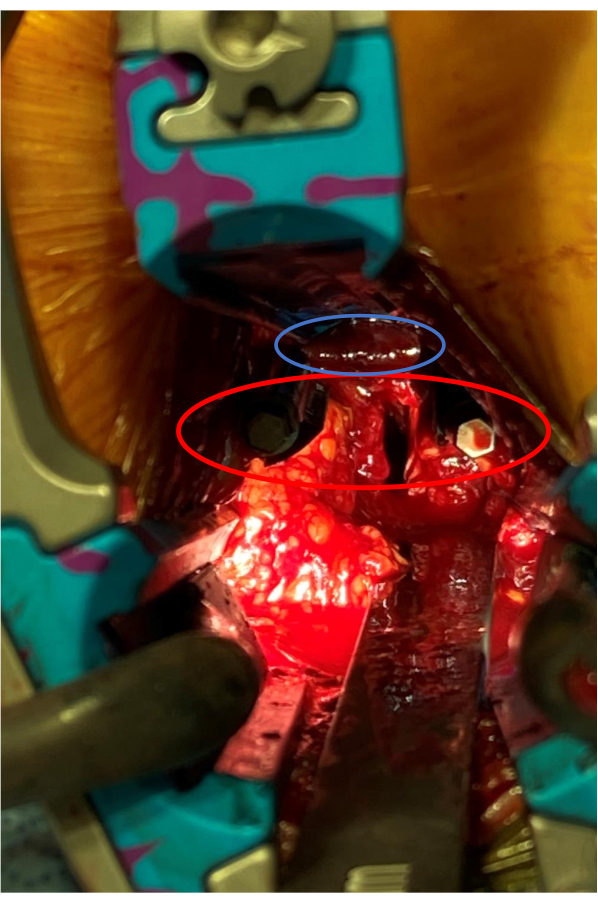
Figure 3: Following direct psoas muscle dissection, separate retractor pins (in red oval) placed in the cranial and caudal vertebral bodies kept the psoas muscle (in blue oval) out of the surgical corridor, allowing easy disc preparation and interbody cage placement. Please click here to view a larger version of this figure.
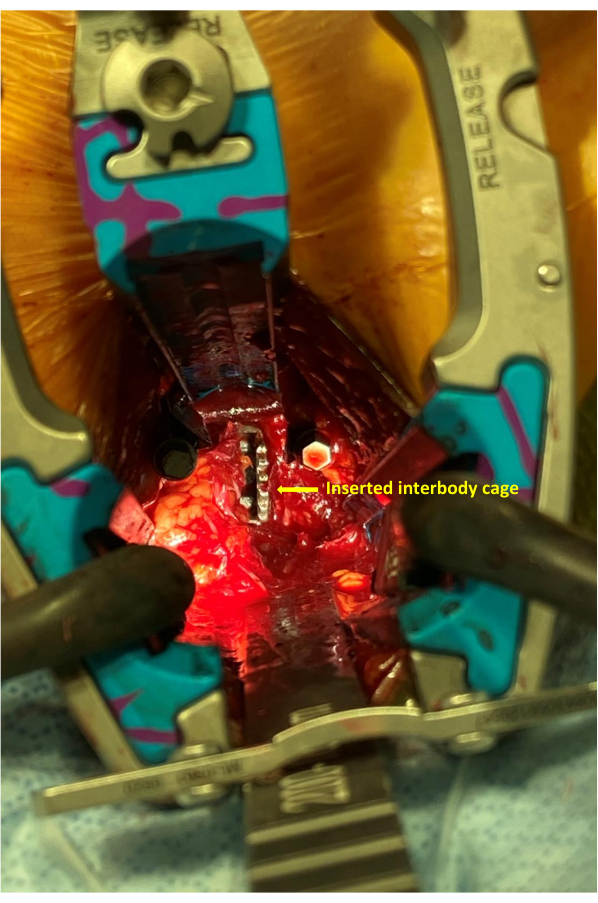
Figure 4: After the disc preparation, the lateral Conduit titanium interbody cage is inserted into the disc space. Please click here to view a larger version of this figure.
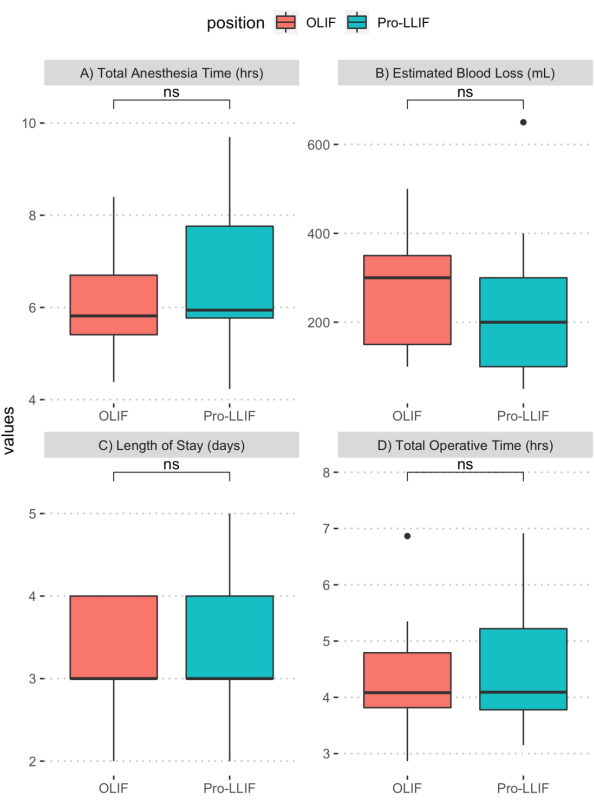
Figure 5: Comparison of operative outcomes between Pro-LLIF and OLIF patients. Student's two-sided, unpaired t-tests were used to compare (A) total anesthesia time (h), (B) estimated blood loss (mL), (C) lengths of stay (days), and (D) total operative time (h). Bonferroni correction was used to adjust for multiple comparisons. No significant difference between the Pro-LLIF and OLIF cohorts was identified for any of the evaluated outcome measures. Abbreviations: pro-LLIF = prone lateral lumbar interbody fusion; OLIF = oblique lateral interbody fusion. Please click here to view a larger version of this figure.
| case | age | sex | BMI | diabetes | smoking | chronic steroids | obesity | asa | Prior fusion | disease | indication | Operated levels | ||||||||||
| 1 | 64 | 0 | 19.92 | 0 | 0 | 0 | 0 | 2 | 1 | spondylolisthesis | radiculopathy/LBP | L2-L3 | ||||||||||
| 2 | 65 | 0 | 40.24 | 0 | 0 | 0 | 1 | 3 | 0 | spondylolisthesis | radiculopathy | L4-L5 | ||||||||||
| 3 | 77 | 0 | 34.72 | 1 | 1 | 1 | 1 | 3 | 1 | Sagittal deformity | radiculopathy.LBP | L2-L4 | ||||||||||
| 4 | 62 | 1 | 35.25 | 0 | 1 | 0 | 1 | 2 | 0 | spondylolisthesis | radiculopathy.LBP | L3-L4 | ||||||||||
| 5 | 68 | 1 | 33.75 | 0 | 1 | 0 | 1 | 2 | 0 | spondylolisthesis | radiculopathy | L3-L5 | ||||||||||
| 6 | 77 | 0 | 23.44 | 1 | 1 | 1 | 0 | 3 | 1 | scoliosis | radiculopathy.LBP | L3-L4 | ||||||||||
| 7 | 41 | 0 | 19.5 | 0 | 1 | 1 | 0 | 2 | 0 | degenerative | radiculopathy | L2-L3 | ||||||||||
| 8 | 72 | 0 | 35.15 | 0 | 1 | 0 | 1 | 3 | 0 | scoliosis | radiculopathy.LBP | L2-L5 | ||||||||||
| 9 | 65 | 0 | 21 | 0 | 0 | 0 | 0 | 2 | 0 | Spondylolisthesis, scoliosis | radiculopathy.LBP | L3-L4 | ||||||||||
| 10 | 74 | 0 | 22 | 0 | 1 | 0 | 0 | 2 | 1 | pseudoarthrosis | LBP | L2-L4 | ||||||||||
Table 1: Pro-LLIF cohort demographics. Basic patient demographics, surgical indications, and operative data for all 10 Pro-LLIF cases of this series. Key: 0 = no, 1 = yes. "ASA" refers to the American Society of Anesthesiologists Physical Status Classification System, which scores patients' health status and the likelihood of surgical and anesthetic comorbidities. ASA score was determined preoperatively by anesthesiology teams at this institution. Abbreviations: pro-LLIF = prone lateral lumbar interbody fusion; ASA = American Society of Anesthesiologists; BMI = body mass index.
| case | Pre-operative foraminal height | Post-operative foraminal height | Pre-operative segmental lordosis | Post-operative segmental lordosis | Pre-operative lumbar lordosis | Post-operative lumbar lordosis | Pre-operative disc height | Post-operative disc height |
| 1 | 18 | 18 | 5 | 16 | 50 | 61 | 8 | 11 |
| 2 | 14 | 20 | 15 | 18 | 30 | 39 | 7 | 15 |
| 3 | 11 | 13 | 5 | 34 | 30 | 45 | 3 | 11 |
| 4 | 21 | 21 | 6 | 20 | 80 | 109 | 12 | 16 |
| 5 | 18 | 23 | 17 | 23 | 28 | 33 | 9 | 10 |
| 6 | 14 | 15 | 4 | 13 | 35 | 50 | 2 | 8 |
| 7 | 13 | 15 | 5 | 10 | 59 | 55 | 2 | 7 |
| 8 | 16 | 15 | 16 | 25 | 40 | 70 | 3 | 10 |
| 9 | 19 | 19 | 4 | 7 | 37 | 39 | 5 | 9 |
| 10 | 19 | 19 | 33 | 23 | 60 | 60 | 12 | 15 |
Table 2: Radiographic evaluation of Pro-LLIF outcomes. Comparison of pre- and postoperative MRIs was used to assess Pro-LLIF's impact on foraminal height, segmental lordosis, lumbar lordosis, and disc height for each patient. Abbreviations: pro-LLIF = prone lateral lumbar interbody fusion; MRIs = magnetic resonance images.
| Outcome | Definition |
| Excellent | All preoperative symptoms relieved; no postoperative symptoms |
| Good | Minimal persistence of preoperative symptoms with minor postoperative symptoms |
| Fair | Relief of some preoperative symptoms with persistence or worsening of others; minor to major postoperative symptoms |
| Poor | Persistence or worsening of all preoperative symptoms; minor to major postoperative symptoms |
Table 3: Odom's criteria (adapted). A 4-point rating scale for assessing clinical outcomes post-PLLIF, adapted from Odom's criteria for cervical spine surgery outcomes. Abbreviation: pro-LLIF = prone lateral lumbar interbody fusion.
