Currently, the described dedicated partial REBOA catheter is the only FDA-approved catheter designed specifically to enable partial occlusion and is in limited market release at 7 Level I trauma centers in North America. The data provided are qualitative surgeon impressions from experienced REBOA users, but no quantitative measurements are obtained as part of this effort. Caution is warranted when interpreting these initial results; similar outcomes may not be observed when using alternative REBOA devices to deliver partial occlusion.
The third-generation, dedicated, partial REBOA catheter is designed specifically to enable partial occlusion while maintaining many of the key features of the second-generation, complete-occlusion catheters, including integrated blood pressure monitoring and image-free and wire-free use. Additionally, it provides significantly improved precision control of occlusion to deliver easily titratable partial aortic occlusion and improve the transition to reperfusion (Video 2). One major clinical benefit of the dedicated partial REBOA catheter is the ability to precisely control the extent of aortic occlusion to allow perfusion past the balloon, as seen on the CT angiogram performed after 2 h of partial aortic occlusion (Video 1). On the CT, partial occlusion is being performed during contrast-enhanced imaging. Distal perfusion should be monitored in real time by ensuring that distal pulses are present via the arterial line or other appropriate method.
Although zone 1 provides maximal hemodynamic support22, complete occlusion in zone 1 has been associated with short occlusion times to mitigate physiologic hazards. The data show that partial occlusion has increased the use of zone 1 occlusion (80% compared to 67% reported in the AORTA database from 2017 to the present), and that partial REBOA is associated with specific features compared to complete occlusion. As shown in Table 1, compared to complete occlusion, partial occlusion significantly increases the following observed benefits: improved transition to reperfusion (56.9% vs 0%), extension of safe occlusion time (47.1% vs 5.6%), reduction of distal ischemia (39.2% vs 5.6%), with a trend toward reduction of proximal hypertension (21.6% vs 0%). As expected, the observations surrounding reduced interoperative bleeding and reduced blood use are not different between the two occlusion strategies. It should be noted that there may be differences in baseline patient physiology (e.g., SBP, injury severity) between the two occlusion strategies, as the surgeons report patient intolerance of partial REBOA as the main reason for using complete REBOA exclusively (85.7%, n = 12 of 14 respondents).
Additionally, in cases requiring extended (≥30 min) occlusion time, surgeons have observed reduction of distal ischemia (47.5% vs 8.7%) and extension of safe occlusion time (50.0% vs 21.7%) at significantly higher rates than when occlusion times are <30 min (Figure 3). There were six cases where occlusion time was not reported and were eliminated from this analysis. One limitation of these initial observed benefits is the use of subjective observations based on clinical experience and expertise of the surgeons, as these items are not quantitatively measured. Quantification of physiological responses to partial occlusion in the clinical setting would benefit the field.
In summary, partial REBOA significantly increases the observation of improved transition to reperfusion, extension of safe occlusion time, and reduction of distal ischemia compared to complete occlusion (Table 1). Additionally, surgeons report reduction of distal ischemia and extension of safe occlusion time significantly more often in cases requiring ≥30 min of occlusion compared to cases of shorter occlusion length (Figure 3). These benefits are associated with partial REBOA, which is characterized by blood flow distal to aortic occlusion (Video 1).
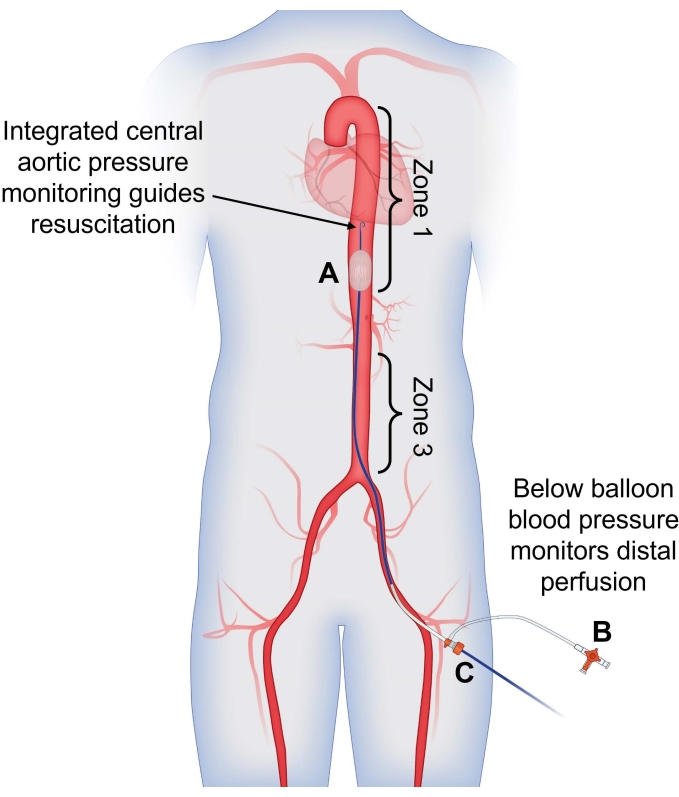
Figure 1: Use of dual arterial blood pressure monitoring to guide partial REBOA. (A) Partial REBOA is performed using the flow channels incorporated into the semicompliant balloon. Integrated central aortic pressure monitoring from the tip of the catheter is used to guide resuscitation and assess the patient's response to partial occlusion, providing a blood pressure reading above the site of occlusion. (B) Arterial pressure measured from the CFA sheath is used to assess distal perfusion; presence of pulsatile arterial flow indicates that partial occlusion is being performed. (C) The catheter is placed through the CFA sheath for a singular access site with dual-channel pressure-monitoring capabilities. Abbreviations: REBOA = Resuscitative endovascular balloon occlusion of the aorta; CFA = common femoral artery. Please click here to view a larger version of this figure.
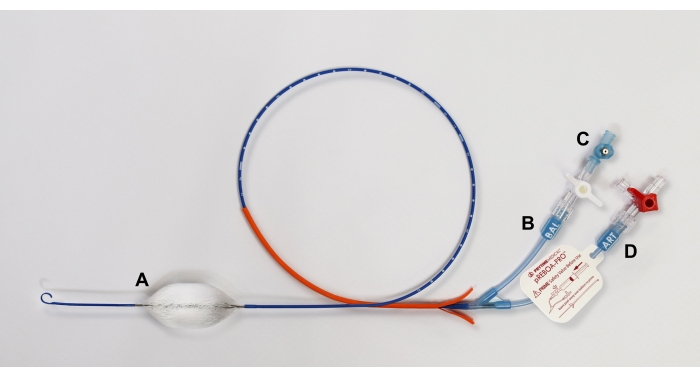
Figure 2: Diagram of pREBOA-PRO catheter and its features. The catheter is characterized by (A) a semicompliant prune balloon that forms flow channels when apposed to the aortic wall, enabling partial REBOA. The catheter includes two extension lines: (B) BAL for balloon inflation with (C) an integrated safety valve to prevent overinflation of the balloon and (D) ART with an integrated arterial line to measure central aortic pressure. Abbreviation: REBOA = Resuscitative endovascular balloon occlusion of the aorta. Please click here to view a larger version of this figure.
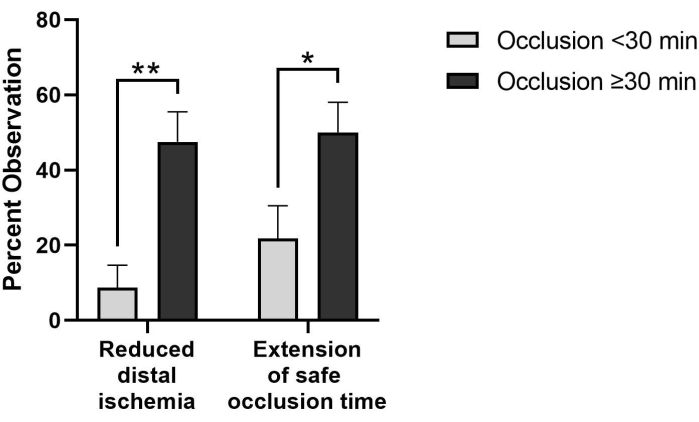
Figure 3: Perfusion-related benefits are observed more frequently in pREBOA-PRO cases requiring extended occlusion times (≥30 min, n = 40) compared to shorter occlusion (<30 min, n = 23). In cases with occlusion times greater than 30 min, reduced distal ischemia and extension of safe occlusion time are observed significantly more frequently than in cases with shorter occlusion times. * indicates p < 0.05, ** indicates p < 0.01 via Fisher's exact test. Data represent mean ± SEM. Please click here to view a larger version of this figure.
Video 1: Partial REBOA observed on CT angiogram with perfusion distal to aortic occlusion after 2 h of partial REBOA in zone 1. The patient was in a motor vehicle collision and was persistently hypotensive upon presentation to the trauma bay with a positive FAST exam, suggestive of abdominal hemorrhage. Partial REBOA was deployed in zone 1, and the patient was taken to the operating room for exploratory laparotomy. As no significant sources of bleeding were identified, a full-body contrast-enhanced CT scan was performed after 2 h of partial aortic occlusion. Partial occlusion was performed during the scan, which allowed contrast to pass, while maintaining hemodynamic stability. Abbreviations: REBOA = Resuscitative endovascular balloon occlusion of the aorta; CT = computed tomography; FAST = focused assessment with sonography in trauma. Please click here to download this Video.
Video 2: Side-by-side comparison of REBOA balloon deflation demonstrating improved transition to reperfusion. Both REBOA balloons are inflated to complete occlusion in a silicone tube with 19 mm inner diameter, simulating zone 1 aortic occlusion. Complete aortic occlusion, evidenced by a non-pulsatile waveform from the distal blood pressure, can be observed on the monitors. The balloons are deflated simultaneously at 0.2 cc/s using a syringe puller. The ER-REBOA catheter (left) has a transition volume of 2.3 cc, while pREBOA-PRO (right) has a transition volume of 9.4 cc. The increased transition volume of the dedicated partial occlusion device provides increased control of aortic occlusion and reperfusion. Abbreviation: REBOA = Resuscitative endovascular balloon occlusion of the aorta. Please click here to download this Video.
| Observed benefit: | Partial REBOA N=51 % (n) | Complete REBOA N=18 % (n) | p value | |
| Improved transition to reperfusion | 56.9 (29) | 0 (0) | *p=0.00001 | |
| Extension of safe occlusion time | 47.1 (24) | 5.6 (1) | *p=0.001 | |
| Reduced distal ischemia | 39.2 (20) | 5.6 (1) | *p=0.007 | |
| Reduced proximal hypertension | 21.6 (11) | 0 (0) | +p=0.05 | |
| Reduced interoperative bleeding | 45.1 (23) | 22.2 (4) | p=0.10 | |
| Reduced blood use | 33.3 (17) | 11.1 (2) | p=0.12 | |
Table 1: Observed benefits in cases utilizing partial REBOA at any point during the case compared to cases utilizing complete aortic occlusion only. Fisher's exact test was used to determine whether response rates for observed benefits differed by aortic occlusion strategy (partial or complete). Exact p values are reported, with * indicating p < 0.05 and + indicating p = 0.05.
