The study was approved by the medical ethics committee of West China Hospital, Sichuan University (2018[457]), and written informed consent was obtained from all subjects.
1. Preoperative preparation
- Patient eligibility
- Select patients who have stringent cosmetic requirements and meet the following criteria: (1) a benign nodule <4 cm in diameter; (2) a differentiated thyroid carcinoma (DTC) <2 cm in diameter without clinical lateral lymph node metastasis or distance metastasis; and (3) no imaging indication of central lymph node metastasis or a metastatic lymph node <2 cm in diameter without fusion and fixation.
- Exclude patients who meet the following criteria: (1) medullary carcinoma or undifferentiated thyroid carcinoma; (2) oral or neck infections; (3) severe thyroiditis that has an acute impact on thyroid function; (4) suspicious invasion of the primary tumor or metastatic lymph node to adjacent organs, such as the esophagus, trachea, or recurrent laryngeal nerve (RLN); (5) location of the primary tumor in the upper pole; (6) previous history of neck surgery, ablation, or neck radiation; (7) biochemical evidence of uncontrolled hyperthyroidism; (8) substernal goiter; and (9) intolerance to surgery.
- Patient preparation
- Evaluate the patients preoperatively with fine-needle aspiration cytologic testing, parathyroid gland tests, thyroid function tests, laryngoscopy, and thyroid ultrasonography16.
- Ask the patient to prepare the oral cavity by using mouthwash (such as tinidazole) before and after meals at least 2 days before the TOETVA and keeping the mouthwash in the mouth for at least 15 s every time.
- Equipment
- Ensure the availability of the absorbable sutures (5-0) for oral wounds.
- Ensure the availability of all the instruments and materials required for the protocol (see Table of Materials).
2. Surgical preparation
- Pre-operative preparation
- Assess the anesthesia risk of surgery according to the American Society of Anesthesiologists' classification17.
- Induce general anesthesia with orotracheal intubation using intraoperative neuromonitoring (IONM).
- Tape the eyes and nose, and pad the head to avoid inadvertent trauma.
- Perform catheterization.
- Operation field
NOTE: Figure 1 shows the schematic of the operating room layout.- Let the operator stand in front of the patient's head. Let the first assistant stand on the left side of the patient's head.
NOTE: The first assistant will be responsible for holding the endoscope. - Let the second assistant stand beside the patient's body according to the location of the lesion to hold the hook. Let the scrub nurse stand beside the patient's leg.
- Place the endoscopic equipment and monitor beyond the patient's feet.
- Place the patient in the supine position with the neck extended. Fix the patient's head with the top cuff during the operation to avoid neck rotation.
- Let the operator stand in front of the patient's head. Let the first assistant stand on the left side of the patient's head.
- Disinfection
- Skin disinfection: Prepare the upper chest, neck, and lower face with iodine solution three times according to the principle of top-down and in-out.
- Oral disinfection: Put the diluted iodine gauze into the mouth, disinfect the oral cavity with it three times, and rinse it with normal saline.
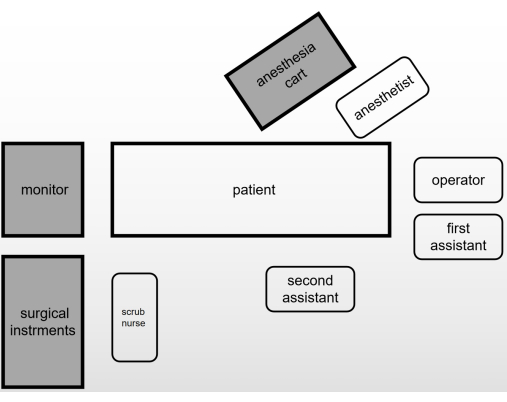
Figure 1: A schematic of the operating room layout. Please click here to view a larger version of this figure.
3. Designing the incisions and establishing the working space (Figure 2)
- Make the camera port incision with an electrotome; this should be a 20 mm transverse incision 5 mm above the frenulum through the alveolar mucosa of the central lower lip vestibule.
- Advance the camera port incision to the chin with an electrotome. Take care to avoid the penetration of the mentum skin. Use hemostatic forceps and a subcutaneous stripping rod to make a tunnel in the midline of the neck, and further extend to the lower neck.
- Place a 10 mm camera through the central port. Insufflate the working space with carbon dioxide gas to establish a pressure of 4 mmHg.
NOTE: The pressure of the carbon dioxide gas should be <8 mmHg to avoid complications caused by high pressure. - Make two 5 mm vertical incisions laterally from the first premolars for instrument placement.
- Use an ultrasonic scalpel to make the working space, and widen it to both sternocleidomastoid muscles laterally and along the subplatysmal plane to the sternal notch inferiorly. Use the traction of the skin suspension device, which is made of unabsorbable sutures (3-0) and rubber bands, to help expand the working space (Figure 3).
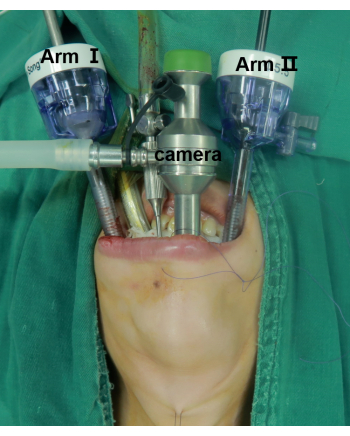
Figure 2: Positioning of the patient and the laparoscopic ports. The center one is the camera port. Arm I and Arm II are for instrument placement. Please click here to view a larger version of this figure.
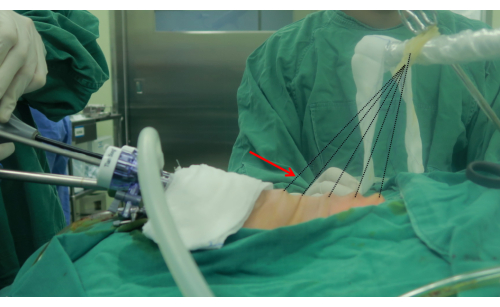
Figure 3: The traction suspension device. The arrow points at the traction suspension device. The suspension device is made of unabsorbable string (3-0) and rubber bands. Please click here to view a larger version of this figure.
4. Thyroid lobectomy
- Divide the linea alba coli with an ultrasonic scalpel. Separate part of strap muscle from the thyroid gland.
- Use a 20 mL needle to pierce the skin at the level of the inferior corner of the thyroid cartilage, and place a pull hook through the hole. Use the pull hook to grab the separated part of the strap muscle.
- Use the ultrasonic scalpel to separate the remaining part of the strap muscle and expose the common carotid artery. Find the vagus nerve, and use the IONM to record the signal.
NOTE: The IONM technology helps to quickly locate, identify, and protect the recurrent laryngeal nerve (RLN) and the external branch of the superior laryngeal nerve (EBSLN). The use of IONM is encouraged; it is an excellent auxiliary tool, but not a mandatory tool. - Use nontraumatic forceps to hold the inferior margin of the isthmus. Use the ultrasonic scalpel to cut the isthmus from the inferior portion of the cricoid cartilage and expose the trachea. For the lobectomy of the TOETVA, first locate the trachea, and take it as a sign.
- Use the nontraumatic forceps to hold the upper pole of the thyroid, and divide the cricothyroid space with the ultrasonic scalpel. Transect part of the sternothyroid muscle. Expose the upper pole of the thyroid.
- Sever the superior thyroid artery and vein. Free the lateral glands from the top down. Lift up the upper pole of the gland, find the RLN under direct visualization, and use the IONM to record the signal.
- Use the ultrasonic scalpel to separate the thyroid capsule from the trachea. Divide the inferior thyroid vessels, and cut the Berry's ligament with the ultrasonic scalpel.
- Remove the unilateral lobe of the thyroid gland from the trachea. Use the IONM to record the signal of the vagus nerve and RLN again.
5. Central lymph node dissection
- Locate the inferior parathyroid gland first, and try to retain it in situ.
NOTE: The thymus should be carefully identified and protected to ensure the functionality of the inferior parathyroid gland from the source of the thymus blood supply and to prevent accidental resection of the parathyroid gland. Carbon nanoparticles can be chosen to help facilitate the identification of the parathyroid glands and the dissection of the lymph nodes. Autotransplantation is feasible for parathyroid glands that cannot be retained in situ. - Stretch the strap muscles to the outside as much as possible to fully expose the operative field.
- Identify the central lymph node compartment by the hyoid bone (superior), suprasternal fossa (inferior), carotid artery (lateral), superficial layer of the deep cervical fascia (anterior), and esophagus (posterior).
- Use the ultrasonic scalpel to dissect the pretracheal and prelaryngeal lymph nodes. Cut the connective tissue in front of the carotid artery to determine the lateral boundary of the central lymph nodes and the connective tissue in front of the trachea to determine the medial boundary of the central lymph nodes. Sweep the anterior side of the left RLN or the anterior and posterior side of the right RLN to complete the central lymph node dissection.
NOTE: The lateral margin should not be swept too deep in order to prevent damage to the vagus nerve and sympathetic trunk. When cleaning the inferior margin, injury to the innominate vessels and pleura should be avoided.
6. Removal of the specimen and closure
- Use endoscopic pouches to remove the specimens.
NOTE: To avoid ectopic implantation, the specimens should be completely removed by the endoscopic pouches. - Wash the surgical wound repeatedly with a large amount of warm sterile distilled water.
- Place a surgical drain (4#) through a small skin puncture in the anterior neck.
- Re-approximate the strap muscles. Close the oral wounds with 5-0 absorbable sutures.
7. Parathyroid gland autotransplantation
- Preserve the parathyroid glands with normal saline, and examine them by frozen section biopsy.
- Cut the isolated parathyroid gland into tiny fragments of 1 mm x 1 mm x 1 mm with ophthalmic scissors. Mix the fragments with normal saline. Inject the mixture into the brachioradialis muscle of the forearm.
