A Teleoperated Robotic System-Assisted Percutaneous Transiliac-Transsacral Screw Fixation Technique
Summary
Teleoperated robotic system-assisted percutaneous transiliac-transsacral screw fixation is a feasible technique. Screw channels can be implemented with high accuracy owing to the excellent freedom of movement and stability of the robotic arms.
Abstract
Transiliac-transsacral screw fixation is challenging in clinical practice as the screws need to break through six layers of cortical bone. Transiliac-transsacral screws provide a longer lever arm to withstand the perpendicular vertical shear forces. However, the screw channel is so long that a minor discrepancy can lead to iatrogenic neurovascular injuries. The development of medical robots has improved the precision of surgery. The present protocol describes how to use a new teleoperated robotic system to execute transiliac-transacral screw fixation. The Robot was operated remotely to position the entry point and adjust the orientation of the sleeve. The screw positions were evaluated using postoperative computed tomography (CT). All the screws were safely implanted, as confirmed using intraoperative fluoroscopy. Postoperative CT confirmed that all the screws were in the cancellous bone. This system combines the doctor’s initiative with the Robot’s stability. The remote control of this procedure is possible. Robot-assisted surgery has a higher position-retention capacity compared with conventional methods. In contrast to active robotic systems, surgeons have full control over the operation. The robot system is fully compatible with operating room systems and does not require additional equipment.
Introduction
The first robotic application utilized in orthopedic surgery was the ROBODOC system employed in 19921. Since then, robot-assisted surgical systems have rapidly developed. Robot-assisted surgery improves arthroplasty by enhancing the surgeon's ability to restore the alignment of the limb and the physiological kinematics of the joint2. In spinal surgery, the placement of pedicle screws using a robot is safe and accurate; it also reduces the surgeon's radiation exposure3. However, studies on robot-assisted surgery have been limited owing to the heterogeneity of traumatic orthopedic diseases. The existing research on robotic surgery for orthopedic trauma mainly focuses on robot-assisted sacroiliac joint screws and pubic-screw fixation of pelvic ring fractures4, cannulated screw fixation of the femoral neck5, entry point and distal locking bolts in intramedullary nailing6,7, percutaneous fracture reduction8,9, and the treatment of critically wounded patients in the military field10.
The percutaneous screw technique can be performed using 2D and 3D navigation support. The sacroiliac, anterior column, posterior column, supraacetabular, and magic screws are the most common percutaneous techniques for pelvic and acetabular factures11. The percutaneous transiliac-transsacral screw technique remains challenging for surgeons. An understanding of pelvic anatomy and X-ray fluoroscopy, accurate positioning, and long-term hand stability are required for this procedure. The teleoperated robotic system can meet these requirements well. This study utilizes a teleoperated robotic system to complete percutaneous transiliac-transsacral screw fixation for pelvic ring fractures. The details and workflow of this protocol are presented below.
Robotic system
The Master-Slave Orthopaedic Positioning and Guidance System (MSOPGS) is mainly composed of three parts: the surgical Robot (Slave Manipulator) with seven degrees of freedom (DOF), the Master Manipulator with force feedback, and the console. The system has four operating modes: manual traction, master-slave operation, remote center of motion (ROM), and emergency. Figure 1 shows the MSOPPGS; its main components are briefly described below.
The surgical robot (see Table of Materials) is a seven DOF manipulator that is pre-certified for integration into medical products12. The Robot has force-feedback sensors that can detect changes in force. The robotic arm can be operated manually or remotely. A torque sensor is installed at the tip and mapped to the "Master Manipulator," enabling real-time force feedback. The maximum load on the robotic arm is sufficient to resist soft tissue forces and reduce the fluttering of the surgical instruments. The Robot is attached to a mobile platform to acquire an operational workplace and ensure stability. The base is connected to the "Master Manipulator" and the operative system and can process instructions from the operative system.
The "Master Manipulator" is designed for healthcare industries to precisely control the Robot. This device offers seven active DOF, including high-precision force-feedback grasping capabilities. Its end effector covers the natural range of motion of the human hand. An incremental control strategy is used to achieve intuitive control of the robotic arm.
The operative system provides four methods for controlling the robotic arm: manual traction, master-slave operation mode, remote centre of motion (RCM), and emergency. The operative system links the surgeon and Robot and provides safety alarms. The manual traction mode allows the manipulator to be dragged freely within a specific working range. The Robot is automatically locked after being stopped for 5 s. In the master-slave mode, the surgeon can use the "Master Manipulator" to control the movement of the robotic arm. The RCM mode permits the surgical instrument to pivot around the end of the instrument. The RCM mode is best suited to reorientation on the axial fluoroscopy view of the channel, such as the radiographic teardrop sign of the supraacetabular channel and the true sacral view of the transiliac-transsacral osseous pathway. The manipulator can be used for emergency braking at any position. Figure 2 shows the workflow of the system.
Protocol
The application of this robotic technique was approved by the ethics committee of the Tongji Hospital of Tongji Medical College, Huazhong University of Science and Technology, and it complies with the Helsinki Declaration of 1975, as revised in 2013.
1. Preoperative planning
- Fix the cadaveric pelves in the supine position using a fluoroscopic plate base (see Table of Materials) by inserting two Schanz pins through the femur. In the supine position, place both the posterior superior iliac spines simultaneously on the plank and the lumbar vertebrae parallel to the floor.
NOTE: The donated cadavers were embalmed by the Department of Anatomy and Research, Tongji Medical College, Huazhong University of Science and Technology. The pelvic specimens were obtained by transection at the level of the lumbar 5 vertebrae and below the lesser trochanter of the femur. The organs in the pelvic cavity were removed. The muscles, joint capsules, and ligamentous structures were left intact. - Acquire images of the pelves from the upper edge of the L5 vertebrae to the distal femoral trochanter using a spiral CT (see Table of Materials). Process the computed tomography (CT) images of all the cadavers using the workstation, and store them in the DICOM format.
NOTE: CT parameters: 0.5 mm slice thickness, 63 mA current, 140 kV voltage. - Import the CT scan data into the preoperative planning software (see Table of Materials) of this system in the DICOM format to obtain axial, coronal, and sagittal images of the pelvis.
NOTE: The DICOM files contain the information from the CT scan, and the reconstructed image can be obtained by automatic import. - Create a cylinder using the MedCAD module of the software, and define the size of the cylinder by typing in the diameter and length. Place it into the S1 or S2 vertebral body, and adjust the orientation of the cylinder midline on the axial and coronal images. Check the relationship between the edge of the cylinder and the cortical bone in each image.
NOTE: The cylinder entirely within the cancellous bone (excluding contact with the cortical bone) is considered to have a corresponding screw channel in S1 or S2. The length of the middle line of the cylinder is the length of the screw.
2. Surgical setting
- Fix the pelvis on the fluoroscopic operating table in the supine position (Figure 1).
- Place the Robot (see Table of Materials) on the ipsilateral side at 45° to the operating table with the C-arm perpendicular to the operating table on the contralateral side. The monitor of the C-arm should face the operating room to enable the surgeon to observe it (Figure 1).
- Place the workstation of the MSOPGS and Slave Manipulator outside the operating room. The surgeon should be able to observe the surgical field and the C-arm monitor while teleoperating with the Slave-Manipulator (Figure 1).
3. Surgical procedure
NOTE: After the system is started and inspected, the manipulator is automatically deployed to the working state.
- Fix the grid position maker with adhesive tape on the ipsilateral side. Select the target area by a grid position marker on the true lateral view of the sacrum. Ensure that the manual traction mode on the console is selected and started. Drag the robotic arm to the general area of the S1 or S2 transiliac-transsacral screw entry point (Figure 3A, B).
NOTE: The target area is enclosed by the anterior border of the sacrum, the sacral nerve canal, and the spinal canal. - Visualize the true lateral view of the sacrum, operate the Master Manipulator, and adjust the tip of the distal sleeve to be located in the guidewire entry area in the Master-Slave operation mode (Figure 3C).
- After selecting the RCM mode, continue the C-arm fluoroscopy for the lateral sacral view. Adjust the center of the guidewire sleeve into concentric circles to be consistent with the screw channel (Figure 3D).
- Lock the robotic arm, and insert a guidewire (2.5 mm K-wire, see Table of Materials) through the contralateral ilium using an electric drill. Then, remove the Robot in Manual traction mode (Figure 3E).
NOTE: No fluoroscopy should be performed during this step. - Turn the C-arm to the inlet and outlet angles (different pelves have different angles) to determine whether the guidewire has broken through or contacted the anterior and posterior sacral cortex and the sacral nerve canal (Figure 3F, G).
- Insert a 7.3 mm semi-threaded screw (see Table of Materials) along the guidewire to the contralateral iliac cortex.
- Assess the screw position in the pelvic inlet and outlet view and the lateral view (Figure 4).
4. Postoperative assessment
- Perform steps 1.2-1.3.
NOTE: CT parameters: 0.5 mm slice thickness, 63 mA current, and 140 kV voltage. - Check the screw position in each axial, coronal, and sagittal image.
NOTE: The screw positions were assessed using Gras's method. Specifically, screws in the cancellous bone are Grade I, screws in contact with the cortical bone are Grade II, and screws that penetrate the cortical bone are Grade III. Grade III represents screw misplacement and indicates a risk of vascular and nerve injury13.
Representative Results
A senior orthopedic surgeon completed the surgery using the procedure described. All the screws (three in S1 and two in S2) were secured. The time taken (from the first X-ray fluoroscopy to the insertion of the screw) for inserting each of the five screws was 32 min, 28 min, 26 min, 20 min, and 23 min, respectively. The fluoroscopy time for each screw was approximately 5 min. Although all the screws were in the correct place on the intraoperative fluoroscopic images, several articles have highlighted the need for postoperative CT scans to evaluate the screw placement. No screws penetrated the cortical bone on the postoperative CT scans. All the screws were completely in the cancellous bone (Figure 4).
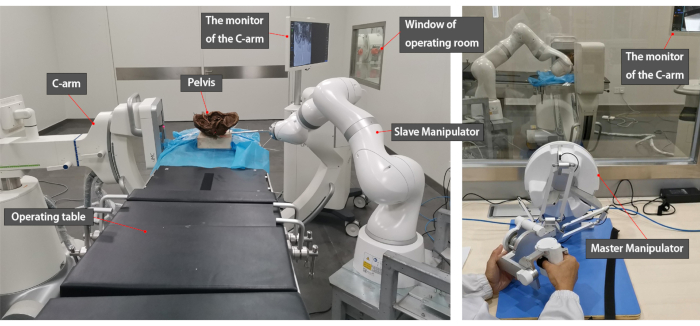
Figure 1: Surgical environment setup. The robotic arm is positioned on the affected side at an angle to the operating table and locked by the base. The C-arm is positioned on the healthy side of the pelvis, with the image display facing the surgeon. The controller for teleoperation is located outside the operating room. Please click here to view a larger version of this figure.
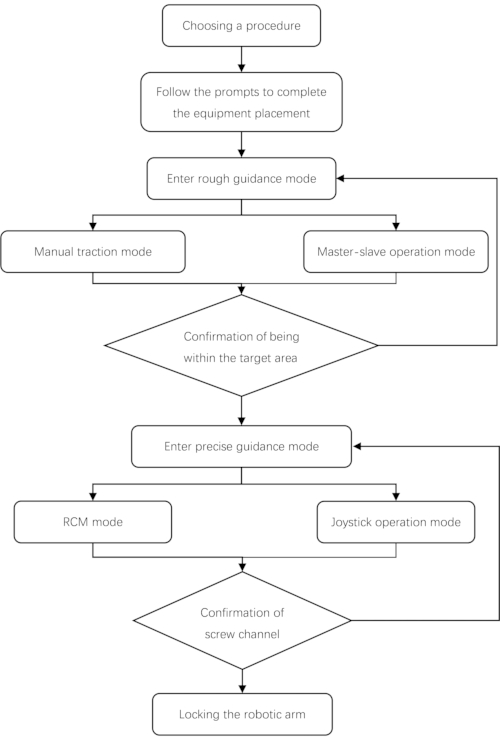
Figure 2: Clinical workflow for MSOPGS. After choosing the surgical procedure, the robot placement instructions should be followed. The rough guidance mode means the surgeon uses Manual traction mode or Master-Slave mode to move the surgical instruments to the position of interest. Then, adjust the sleeve's direction in the RCM mode or Joystick operation mode. In other words, the rough mode is used to select the entry point, and the precise mode is used to adjust the direction of the guidewire. The Joystick operation mode, used for the oblique sacroiliac style screws, is not mentioned in the text. Please click here to view a larger version of this figure.
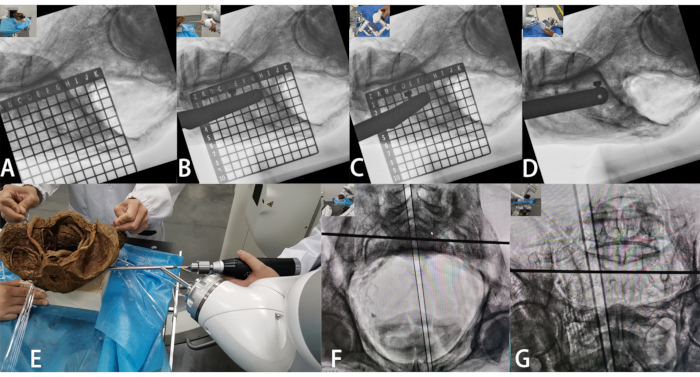
Figure 3: Surgical procedure. (A) Locating the target area using the grid prior to surgery. (B) Dragging the robotic arm into the target area. (C) In Master-Slave operation mode, the robotic arm is more precisely positioned so that the guidewire sleeve is at the desired entry point. (D) Movement is made around the distal end of the guidewire sleeve until the sleeve appears as a concentric circle. (E–G) After drilling into the guidewire, the ideal position of the guidewire is confirmed on the inlet and outlet images of the pelvis. Please click here to view a larger version of this figure.
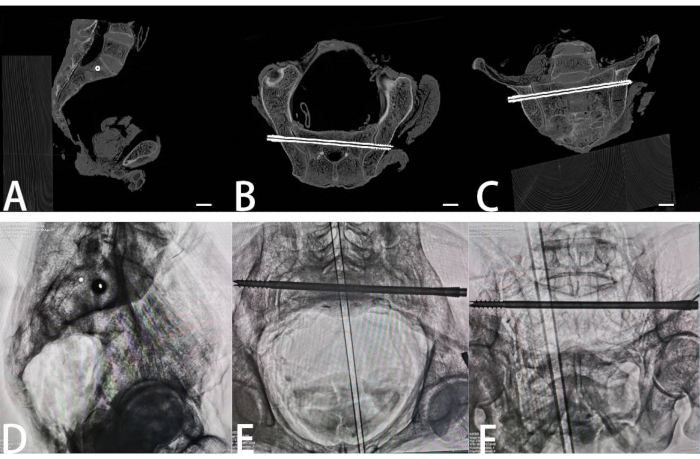
Figure 4: Computed tomography reconstruction and X-rays confirming that the screw was entirely within the cancellous bone. (A) Sagittal CT reconstruction images of the midline site suggesting that the screw is located in the S1. (B) The screw did not enter the sacral canal on the reslice axial CT reconstruction image. (C) The screw is safe on the reslice coronal CT reconstruction image. (D) The screw is located entirely within the bone on the true lateral view of the sacrum. (E,F) The screw is at a safe distance from the anterior and posterior sacral cortex and the sacral nerve canal on the inlet and outlet images. Scale bars (A–C): 2 cm. Please click here to view a larger version of this figure.
Discussion
Regardless of the type of Robot, the core application of robots in orthopedics provides an advanced tool for surgeons to improve the accuracy of surgery. However, the emergence of surgical robots is not a replacement for doctors. Surgeons performing robotic surgery may or may not be in the operating room. Surgical robots generally include a computer control system, a robotic arm responsible for the operation, and a navigation system responsible for tracking. There are three categories of robot systems depending on how the robot and the surgeon interact, including semi-active, passive, and active systems14. Robotic assistance is mainly restricted to joint arthroplasty and spinal instrumentation procedures to improve surgical accuracy2,15,16. The use of robots in trauma orthopedics is relatively rare. Trauma Pod10 saves the lives of critically injured patients on the battlefield, and Robot-assisted fracture surgery (RAFS)17 and RepoRobo18 can assist in femoral fracture reduction. The TiRobot is a semi-automatic robot system that uses an intelligent algorithm to plan the screw trajectory based on preoperative images; it uses 3D imaging and optical tracking to navigate19,20. The system can only perform preoperative planning and navigation and cannot perform other surgical tasks. Similarly, the TiRobot system plays a role in determining the screw position during femoral neck fracture surgery21. As a tool, the MSOPGS combines with doctors’ skills and knowledge to make surgery more accurate and minimally invasive.
Transiliac-transsacral screws break through six layers of cortical bone22. The screw channel is so long that minor discrepancies can result in iatrogenic neurovascular injuries. The most significant challenge associated with the freehand technique is adjusting the guidewire direction in the outlet and inlet views. The guidewire deflects when it breaks through the cortical or subchondral bone. Robot-assisted surgery is more precise than traditional surgical procedures for the following reasons. First, the amplitude of the surgeon’s hand movements is not transferred to the surgical instruments on a one-to-one basis. The scaling effect reduces the amplitude of the movements of the surgical instrument to facilitate finer movements. Second, the Robot can maintain its position without any deviation. However, whether soft tissues are traumatized during the movement of the surgical instruments is unknown. A feedback threshold is required to avoid excessive tension on the soft tissue. Moreover, the surgeon can avoid the danger of radiation exposure during the entire procedure.
New technology is always associated with a learning curve. In this study, compared with the time taken to fix the first three screws, the operation time of the last two screws was significantly reduced. The teleoperation logic will help surgeons create connections in the brain between the surgical instrument and the Master Manipulator. Doctors should be skilled in placing the sacroiliac screws using the freehand technique under fluoroscopy. In our technique, an intuitive control strategy was used to reduce the difficulty of operating the system. Although the Master Manipulator and the end of the surgical instrument are not in the same working space, the end of the surgical instrument can move appropriately with the Master Manipulator. The RCM, the most crucial step, greatly simplifies the adjustment of the direction of the guidewire. The RCM mode ensures that the entry point is not displaced during rotation, provided that the entry point is determined. The surgeon operates the Master Manipulator, and the surgical instruments move in a cone-like space, where the apex is the point of screw insertion.
As lateral sacral images are used for most of the procedure, the patients must maintain the same position throughout the surgery. In cadaveric studies, the pelvis is fixed on the surgical table. The patient’s trunk can be secured to the surgical table using a harness in real surgical settings. However, patients are heavier than cadavers and do not move as easily. The Robot and the patient are two unrelated parts of the system. With the development of the project, the Robot and patient will form a real-time synchronized system using a tracking system, meaning that the relative positions of the Robot and patient can remain constant.
This robotic system is expected to become an essential part of telemedicine in the future owing to its low latency and compatibility with current surgical systems. Patients with orthopedic trauma have a specific time window between injury and surgery, especially in the case of pelvic and acetabular fractures. In such cases, ensuring circulatory stability and preventing other systemic injuries are pivotal. Doctors at central hospitals can use the telemedicine system to guide preoperative preparations and perform complete remote surgery through the MSOPGS. Furthermore, this system combines 2D or 3D navigation, virtual reality (VR), augmented reality (AR), and mixed reality (MR) technologies. Reality technology possesses significant potential for orthopedic surgery. The ability to verify patient data at any time, advance the plan of the operation, and improve the precision of interventions enhances the quality of healthcare and patient outcomes23. The preoperative imaging data can be combined with further visual data presented in a spatially correct alignment to the patient’s surface. Multimodal image integration in AR/MR provides surgeons with intraoperative fluoroscopy by overlaying image reconstructions with actual anatomical structures, thereby eliminating the necessity to reuse radiation.
This study has some limitations. The sample size for the pelvis used was small. Although we attempted to simulate the actual surgical circumstance completely, there are significant differences between cadaveric studies and real operating circumstances. This system needs to be further refined for clinical applications.
Divulgaciones
The authors have nothing to disclose.
Acknowledgements
None.
Materials
| 160-slice CT | United Imaging Healthcare Surgical Technology Co. Ltd | uCT780 | Acquire the prescise image and DICOM data |
| Electric bone drill | YUTONG Medical | None | Power system |
| Fluoroscopic plate base | None | None | Fix the cadaveric pelves to operating table |
| K-wire | None | 2.5mm | Guidewire |
| Master-Slave Orthopaedic Positioning and Guidance System | United Imaging Healthcare Surgical Technology Co. Ltd | None | A teleoperated robotic system that positions screws for orthopaedic surgery |
| Mimics Innovation Suite | Materialise | Mimics Medical 21 | Preoperative planning software |
| Mobile C-arm | United Imaging Healthcare Surgical Technology Co. Ltd | uMC560i | Low Dose CMOS Mobile C-arm |
| Operating table | KELING | DL·C-I | Fluoroscopic surgical table |
| Schanz pins | Tianjin ZhengTian Medical Instrument Co.,Ltd. | 5.0mm | Fix the cadaveric pelves |
| Semi-threaded screw | Tianjin ZhengTian Medical Instrument Co.,Ltd. | 7.3mm | Transiliac-Transsacral Screw |
| Seven DOF manipulator | KUKA, Germany | LBR Med 7 R800 | Device for performing surgical operations |
Referencias
- Bargar, W. L., Bauer, A., Börner, M. Primary and revision total hip replacement using the Robodoc system. Clinical Orthopaedics and Related Research. (354), 82-91 (1998).
- Jacofsky, D. J., Allen, M. Robotics in arthroplasty: A comprehensive review. Journal of Arthroplasty. 31 (10), 2353-2363 (2016).
- Perfetti, D. C., Kisinde, S., Rogers-LaVanne, M. P., Satin, A. M., Lieberman, I. H. Robotic spine surgery: Past, present and future. Spine. 47 (13), 909-921 (2022).
- Long, T., et al. Comparative study of percutaneous sacroiliac screw with or without TiRobot assistance for treating pelvic posterior ring fractures. Orthopaedic Surgery. 11 (3), 386-396 (2019).
- Duan, S. J., et al. Robot-assisted percutaneous cannulated screw fixation of femoral neck fractures: Preliminary clinical results. Orthopaedic Surgery. 11 (1), 34-41 (2019).
- Lei, H., Sheng, L., Manyi, W., Junqiang, W., Wenyong, L. A biplanar robot navigation system for the distal locking of intramedullary nails. International Journal of Medical Robotics and Computer Assisted Surgery. 6 (1), 61-65 (2010).
- Oszwald, M., et al. Robotized access to the medullary cavity for intramedullary nailing of the femur. Technology and Health Care. 18 (3), 173-180 (2010).
- Hung, S. S., Lee, M. Y. Functional assessment of a surgical robot for reduction of lower limb fractures. International Journal of Medical Robotics and Computer Assisted Surgery. 6 (4), 413-421 (2010).
- Dagnino, G., et al. Image-guided surgical robotic system for percutaneous reduction of joint fractures. Annual Review of Biomedical Engineering. 45 (11), 2648-2662 (2017).
- Garcia, P., et al. Trauma Pod: A semi-automated telerobotic surgical system. International Journal of Medical Robotics and Computer Assisted Surgery. 5 (2), 136-146 (2009).
- Gaensslen, A., Müller, M., Nerlich, M. . Acetabular Fractures: Diagnosis, Indications, Treatment Strategies. , (2017).
- LBR Med: A collaborative robot for medical applications. KUKA Available from: https://www.kuka.com/en-cn/industries/health-care/kuka-medical-robotics/lbr-med (2023)
- Gras, F., et al. 2D-fluoroscopic navigated percutaneous screw fixation of pelvic ring injuries–A case series. BMC Musculoskeletal Disorders. 11, 153 (2010).
- Innocenti, B., Bori, E. Robotics in orthopaedic surgery: Why, what and how. Archives of Orthopaedic and Trauma Surgery. 141 (12), 2035-2042 (2021).
- Chen, A. F., Kazarian, G. S., Jessop, G. W., Makhdom, A. Robotic technology in orthopaedic surgery. Journal of Bone and Joint Surgery. 100 (22), 1984-1992 (2018).
- D’Souza, M., et al. Robotic-assisted spine surgery: History, efficacy, cost, and future trends. Robotic surgery. 6, 9-23 (2019).
- Dagnino, G., et al. Navigation system for robot-assisted intra-articular lower-limb fracture surgery. International Journal for Computer Assisted Radiology and Surgery. 11 (10), 1831-1843 (2016).
- Füchtmeier, B., et al. Reduction of femoral shaft fractures in vitro by a new developed reduction robot system ‘RepoRobo. Injury. 35, 113-119 (2004).
- Schuijt, H. J., Hundersmarck, D., Smeeing, D. P. J., vander Velde, D., Weaver, M. J. Robot-assisted fracture fixation in orthopaedic trauma surgery: A systematic review. OTA International. 4 (4), 153 (2021).
- Wang, J. Q., et al. Percutaneous sacroiliac screw placement: A prospective randomized comparison of robot-assisted navigation procedures with a conventional technique. Chinese Medical Journal. 130 (21), 2527-2534 (2017).
- Zhu, Z. D., et al. TiRobot-assisted percutaneous cannulated screw fixation in the treatment of femoral neck fractures: A minimum 2-year follow-up of 50 patients. Orthopaedic Surgery. 13 (1), 244-252 (2021).
- Gardner, M. J., Routt, M. L. Transiliac-transsacral screws for posterior pelvic stabilization. Journal of Orthopaedic Trauma. 25 (6), 378-384 (2011).
- Verhey, J. T., Haglin, J. M., Verhey, E. M., Hartigan, D. E. Virtual, augmented, and mixed reality applications in orthopedic surgery. International Journal of Medical Robotics and Computer Assisted Surgery. 16 (2), 2067 (2020).
