Induction of Periodontitis via a Combination of Ligature and Lipopolysaccharide Injection in a Rat Model
Summary
In this study, a rat model of induction of periodontitis is presented via a combination of retentive ligature and repetitive injections of lipopolysaccharide derived from Porphyromonas gingivalis, over 14 days around the first maxillary molars. The ligation and LPS injection techniques were effective in inducing peridontitis, resulting in alveolar bone loss and inflammation.
Abstract
Periodontitis (PD) is a highly prevalent, chronic immune-inflammatory disease of the periodontium, that results in a loss of gingival soft tissue, periodontal ligament, cementum, and alveolar bone. In this study, a simple method of PD induction in rats is described. We provide detailed instructions for placement of the ligature model around the first maxillary molars (M1) and a combination of injections of lipopolysaccharide (LPS), derived from Porphyromonas gingivalis at the mesio-palatal side of the M1. The induction of periodontitis was maintained for 14 days, promoting the accumulation of bacteria biofilm and inflammation. To validate the animal model, IL-1β, a key inflammatory mediator, was determined by an immunoassay in the gingival crevicular fluid (GCF), and alveolar bone loss was calculated using cone beam computed tomography (CBCT). This technique was effective in promoting gingiva recession, alveolar bone loss, and an increase in IL-1β levels in the GCF at the end of the experimental procedure after 14 days. This method was effective in inducing PD, thus being able to be used in studies on disease progression mechanisms and future possible treatments.
Introduction
Periodontitis (PD) is the sixth most prevalent public health condition worldwide, affecting approximately 11% of the total population, being an advanced, irreversible, and destructive form of periodontal disease1,2. PD is an inflammatory process that affects the gingival and periodontal tissues, which results in gingiva recession, apical migration of the junctional epithelium with pocket development, and the loss of alveolar bone3. Furthermore, PD is associated with several systemic diseases, including cardiovascular disease, obesity, diabetes, and rheumatoid arthritis, for which environmental and host-specific factors play a significant role4,5.
Hence, PD is a multifactorial disease primarily initiated by the accumulation of microbial plaque – resulting from dysbiosis of microbial communities – and by an exaggerated host immune response to periodontal pathogens, which leads to the breakdown of periodontal tissue4,6. Among several periodontal bacteria, the gram-negative anaerobic bacterium Porphyromonas gingivalis is one of the key pathogens in PD4. P. gingivalis contains a complex lipopolysaccharide (LPS) in its walls, a molecule known to induce polymorphonuclear leukocyte infiltration and vascular dilatation in inflamed periodontal tissues7. This results in the production of inflammatory mediators, such as interleukin 1 (IL-1), IL-6, and IL-8, tumor necrosis factor (TNF), or prostaglandins, with a subsequent osteoclast activation and bone resorption, leading to tissue destruction and ultimate tooth loss3.
Among the different advantages of animal models include the capacity to mimic cellular complexities as in humans, or to be more accurate than in vitro studies, which are carried out on plastic surfaces with limited cell types8. For modeling PD experimentally in vivo, different animal species have been used, like non-human primates, dogs, pigs, ferrets, rabbits, mice, and rats9. However, rats are the most extensively studied animal model for the pathogenesis of PD because they are inexpensive and easy to handle10. Their dental gingival tissue has similar structural features to human gingival tissue, with a shallow gingival sulcus and junctional epithelium attached to the tooth surface. Furthermore, as in humans, the junctional epithelium facilitates the passage of bacterial, foreign materials, and exudates from inflammatory cells 9.
One of the most reported experimental models of PD induction in rats is the placement of ligatures around the teeth, which is technically challenging but reliable10. The ligature placement facilitates dental plaque and bacterial accumulation, generating a dysbiosis in the gingival sulci, that causes periodontal tissue inflammation and destruction11. Loss of periodontal attachment and resorption of alveolar bone could occur in 7 days in this rat model8.
Another animal model for PD consists of the injection of LPS into the gingival tissue. As a result, osteoclastogenesis and bone loss are stimulated. The histopathological features of this model are similar to human-established PD, characterized by higher levels of proinflammatory cytokines, collagen degradation, and alveolar bone resorption6,8.
Thus, the aim of this study was to describe a simple rat model of experimental PD based on the techniques of P. gingivalis-LPS (Pg-LPS) injections, combined with ligature placement around the first maxillary molars (M1). This is a model with similar characteristics to those observed in human PD disease, which could be used in the study of disease progression mechanisms and future possible treatments.
Protocol
NOTE: The experimental protocol of the study was approved by the Ethical Committee of Animal Experimentation of the Balearic Islands Health Research Institute (CEEA-UIB; reference number 163/03/21).
1. Animal anesthesia and procedure preparation
- Sterilize all surgical instruments (aluminium mouth gags, dental explorer, diamond lance, surgical scissors, microsurgical pliers, a micro needle holder, a hollenback carver, a periosteal microsurgical elevator, and microsurgical scissors) (5 min at 135 °C) before surgery.
- Prepare all the solutions needed for the procedure in sterile conditions, as described:
- Prepare a mix of Ketamine (60 mg/mL) and Xylazine (8 mg/mL) by mixing 1.6 mL of Ketamine with 1 mL of Xylazine diluted in Phosphate Buffer Solution (PBS)/saline. Store the stock at 4 °C.
- Dilute Atipamezole to a final concentration of 0.25 mg/mL in PBS/saline. Store the stock at 4 °C.
- Dilute Buprenorphine to a final concentration of 0.03 mg/mL in PBS/saline. Store the stock at 4 °C.
- Prepare 1 mL of Pg-LPS (1 mg/mL) in sterile saline. Store the stock at -20 °C.
- For the experiment, use female and male Wistar rats, aged 12 weeks and weighing 210-350 g at the time of surgery. Keep the animals housed in groups under the appropriate environment and constant conditions (20-24 °C, 12 h per day light-dark cycles), with food and standard water, offered ad libitum.
- To induce anesthesia, weigh the rat and administer the mix of Ketamine/Xylazine at a concentration of 80/10 mg/kg intraperitoneally (IP), by using a 25 G sterile hypodermic needle and 1 mL syringe.
- After the rat is anesthetized, place the animal on its back on a heated surgical platform; during the procedure, cover the animal's body to prevent heat loss.
NOTE: Anesthesia depth is assessed by the loss of pedal reflex during the procedure and by monitoring vital signs. If needed, use a small nose cone to maintain anesthesia with 2% Isoflurane in 100% oxygen. Apply sterile ophthalmic ointment to both eyes after anesthesia induction to protect the corneas and prevent drying. - During the procedures, administer 100% oxygen using a small nose cone, and monitor the pulse rate and oxygen saturation by pulse oximetry.
NOTE: If the oxygen saturation and pulse rate fall below 95% and 190 bpm, respectively, stop the procedure and place the animal in the lateral decubitus position until reaching normal values. - Open the rat mouth using an aluminum mouth gag around the incisors (upper and lower), retracting the tongue with it and stabilizing the maxilla and mandible in an open, comfortable working position, enabling access to mandibular molars.
NOTE: If the animal needs to be placed in lateral decubitus, remove the mouth gag before changing its position to favor recovery. Once the animal is anesthetized, collect gingival crevicular fluid (GCF) before surgery (sample in basal conditions) (day 0). - Collect GCF as described by the following steps:
- Place the animal on its back on a surgical platform and stabilize the maxilla and mandible in an open position with aluminum mouth gags.
- Collect GCF using a total of four (two for each M1) absorbent paper point nº 30 (0.03 cm diameter x 3 cm length), by inserting it into the gingival crevice (space between gingival epithelium and adjacent enamel) around the mesio-palatal of the M1 until slight resistance. Retain the paper point in the same position for a total of 30 s before immediate removal.
- After collection, transfer the paper point immediately into a plastic vial, and store at -80 °C until assay performance.
2. Retentive ligature technique and intragingival Pg -LPS injection
NOTE: The ligature model was created (day 0) by placing a sterile braided silk ligature (5/0) around the M1 bilaterally within the gingival sulcus using microsurgical instruments and securing it with the surgeon's knots on the palatal surface. The microsurgical instruments used were microsurgical pliers, a micro needle holder, a hollenback carver, a periosteal microsurgical elevator, and microsurgical scissors. Surgical loupes with an LED light source were also used (3.6x magnification).
- Position the distal tail of the suture on the palatal side of the dentition and insert the proximal segment between the contact of M1 and second maxillary molars (M2).
- Use the periosteal microsurgical elevator to insert the suture within the sulcus. Wrap the ligature around the buccal surface of the M1 very carefully, as the tissues at this level present a narrow zone of attached gingiva. On the palatal aspect, make sure the suture is tightened on both ends to ensure it is driven into the gingival sulcus.
NOTE: If resistance is observed when inserting the suture between the M1 and the M2, the contact may be opened slightly using a dental explorer and diamond lance-shaped bur. - Tie the ends of the suture with a surgeon's knot and trim the tails as short as possible. Insert the knot in the sulcus.
NOTE: Tips of surgical instruments can cause oral trauma and bleeding. Prepare small segments of gauze or a cotton swab to remove blood from the oral cavity and apply pressure to stop any hemorrhage. Careful soft tissue management with a microsurgical approach minimizes surgical complications and leads to less tissue trauma. - After ligature positioning, inject 40 µL of Pg-LPS in sterile saline with a 25 G sterile hypodermic needle and a 1 mL syringe to the subgingival tissue (between the root or neck of a tooth and the gum margin) at the mesio-palatal side of the M1 bilaterally (day 0).
3. End of the procedure
- After ligation positioning and Pg-LPS application, release the rat from the surgical state and place it in a clean individual cage under a heat lamp.
- Inject the antagonist Atipamezole (0.5 mg/kg subcutaneously (SC)) with a 25 G sterile hypodermic needle and a 1 mL syringe.
- For pain relief, inject 0.03 mg/kg Buprenorphine, SC.
- Monitor the animal's recovery until the effects of the operation are completely reversed. Individually house each rat in the appropriate environment under constant conditions (20-24 °C, 12 h per day light-dark cycles). Offer food and deionized water ad libitum.
- During the first 2 days after the procedure, weigh the animals and inject Buprenorphine SC twice daily for pain relief.
NOTE: Buprenorphine can be administered before beginning the procedure to eliminate the windup effect. - During the time of the experiment, monitor the animals by weight and general behavior assessment one or two times a week.
4. Post-procedure follow-up
NOTE: The induction of PD was maintained for 14 days to promote the accumulation of bacteria biofilm and consequent inflammation. The ligatures have to be examined and adjusted, and Pg-LPS is injected three times per week (day 2, day 4, day 6, day 8, day 10, and day 12).
- Examine and adjust the ligature (day 2, day 4, day 6, day 8, day 10, and day 12) as follows:
- Anesthetize with 2% isoflurane in 100% oxygen using an anesthesia induction chamber.
- After the rat is anesthetized, place the animal on its back and use a small nose cone during the procedure with 1% isoflurane in 100% oxygen for maintenance of the animal anesthesia.
- Open the rat mouth using the aluminum mouth gag around the incisors (upper and lower), retracting the tongue with it and stabilizing the maxilla and mandible in an open, comfortable working position, enabling access to ligatures.
- Tighten the ligatures against the gingiva with the help of a periosteal microsurgical elevator, and make sure the suture of the ligatures is inserted, creating inflammation around the gingiva.
NOTE: It is possible that 7-10 days after surgery, ligatures are lost. If this happens, follow the protocol as explained for the injection of Pg-LPS (step 2.4).
- After the ligature adjustment, bilaterally inject 40 µL of Pg-LPS with a 25 G sterile hypodermic needle and a 1 mL syringe to the subgingival tissue at the mesio-palatal side of the M1 (day 2, day 4, day 6, day 8, day 10, and day 12).
- Remove the nose cone for anesthesia and place the rat in its cage. Monitor the animal's recovery until the effects of the anesthesia are completely reversed.
5. Animal sacrifice and analysis
NOTE: There are different options for evaluating the progression of PD. Here, the analysis described consists of an evaluation of pro-inflammatory cytokines at the gingival crevicular fluid (GCF), and an evaluation of the loss of alveolar bone.
- On day 14 of the study (day 14), sacrifice the animals with CO2 in a carbon dioxide chamber. A displacement rate of 30% to 70% of the chamber volume/min is recommended for rodents.
NOTE: Lack of animal response to pedal reflex and absence of vital signs must be verified to confirm euthanasia. - Collect GCF as described by the following steps:
NOTE: GCF is collected before PD induction (before surgery) (day 0) and after PD induction (after sacrifice) (day 14).- Place the animal on its back on a surgical platform, and stabilize the maxilla and mandible in an open position with aluminum mouth gags.
- Collect the GCF using adsorbent paper point nº 30 (0.03 cm diameter x 3 cm length) by inserting it into the gingival crevice around the mesio-palatal of the M1 until slight resistance. Retain the paper point in the same position for a total of 30 s before immediate removal.
- After collection, transfer the paper point immediately into a plastic vial and store at -80 °C until assay performance.
- To evaluate proteins within the GCF, prepare the following solutions and follow the steps of the elution method as described:
NOTE: IL-1β is evaluated on the GCF (day 14) using an immunoassay, according to the manufacturer's protocol.- Prepare the elution buffer fresh and keep it on ice throughout the entire extraction process to inhibit protease activity.
- Prepare all solutions needed for the elution buffer as described:
- Prepare 1 mL of Aprotinin (1 mg/mL) in ultrapure water.
- Prepare 10 mL of phenylmethylsulfonylfluoride (PMSF) (200 mM) in methanol.
- Add 125 µL of PMSF and 250 µL of Aprotinin to 24.5 mL of PBS solution (pH = 7.4) to prepare the elution buffer.
- Dissolve one commercial phosphatase inhibitor tablet with 10 mL of freshly prepared elution buffer for 10 min under agitation at 4 °C.
NOTE: The duration of GCF elution is limited; use immediately for centrifugations after the addition of phosphatase inhibitor tablet within the first 30 min. - After adding the phosphatase inhibitor, add 11 µL of complete elution buffer directly onto the tube with the paper points.
- Centrifuge the tube at 452 x g for 5 min at 4 °C.
- Transfer the eluted content to a new plastic vial. Repeat this process four additional times to yield a 50 µL total volume.
- After the last centrifugation, add a total volume of 60 µL directly onto the paper point, and centrifuge one last time at 452 x g for 5 min at 4 °C.
- Use the required volume eluted for protein evaluation.
- After euthanasia and GCF collection, with the help of surgical scissors, cut out the superior jaw of the rats. Try to peel off the mask of the rat and leave as little soft tissue as possible.
- Position the jaw in the microscope stage for visualization and take a picture at the desired magnification.
- Place the jaw directly in 4% paraformaldehyde (PFA) diluted in PBS. Refresh twice a week with new PFA for 12 days for a complete fixation.
CAUTION: Steps involving PFA should be performed in a fume hood following the Safety Data Sheet recommendations. - After complete jaw fixation, evaluate bone loss using a cone-beam computed tomography (CBCT) scanner, as follows:
- Open the PC.
- Open the CBCT analysis program.
- Select Scan Protocol > Denture Scan Mode.
- Select Field of View (FOV) > (11×8) HIRes (90 kV of voltage and 3 mA of current).
- Place the fixed upper maxilla of the rats in the gantry.
- Click Next.
- Click the X-ray firing button (press the X-ray remote control to make the emission and keep it pressed for the entire duration of the scan).
- If necessary, relocate the upper maxilla in the center of the frontal plane by pressing the control button, then click the X-ray firing button (press the X-ray remote control to make the emission and keep it pressed for the entire duration of the scan).
- Click Next.
- Click the X-ray firing button (press the X-ray remote control to make the emission and keep it pressed for the entire duration of the scan).
- If necessary, relocate the denture in the center of the sagittal plane by pressing the control button, then click the X-ray firing button (press the X-ray remote control to make the emission and keep it pressed for the entire duration of the scan).
- Click Next.
- Click the Start button (press the X-ray remote control to make the emission and keep it pressed for the entire duration of the exam). Wait until receiving a processing message, and then follow the instructions shown.
- A window view appears. Regulate the gray at 65% and click Apply.
- For saving the scan, click on File and save it in DICOM format. Then, click All Images and at the DICOM export selection window, select all the parameters shown (initial image, original axial, reformatted axial, multiplanar) and select predefined type.
- Process the maxillary molars' two-dimensional and sagittal representative images using an analysis program, as follows:
- Open the software.
- Click File and Open, and then select the folder with images in DICOM format and click Open.
- Wait until the window "Convert to 8 bit" appears, select the range from 0 to 6,000, and click OK.
- Click Raw images.
- Define the top and bottom of the selection to limit the region of interest. Search for the first and last images where alveolar bone appears and select it with the top of selection and bottom of selection commands.
NOTE: Representative two-dimensional images of the alveolar bone of the molars could be exported, as in Figure 3A,B. - For sagittal representative images, click on Toggle profile bar.
- Draw a sagittal line in the middle of the palate and click Reslice model. Determine parameters for delimiting the region of interest (slice spacing: 1; number of slices: 100) and click OK. Wait until the reslicing model ends. Finally, click save Resliced images.
NOTE: Representative sagittal imagines of the alveolar bone of the molars could be exported, as in Figure 3C,D.
Representative Results
A timeline of the experimental steps is presented in Figure 1. Figure 2A shows an image of the mandibula after surgical intervention, with ligature placement around the sulcus of the M1 at time 0 of the experiment. Figure 2B shows how, after 14 days of the procedure, the ligature around the M1 enters the gingival sulcus, causing inflammation of the gingiva and infiltrating accumulation.
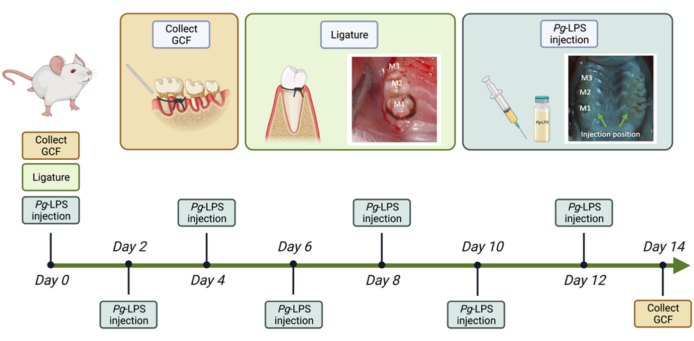
Figure 1: Schematic representation of the timeline of the experimental procedure of periodontitis (PD) induction in rats. Please click here to view a larger version of this figure.
Representative bi-dimensional images (Figure 3; red square) demonstrate alveolar bone loss differences in the mandibula between the basal control, showing more bone volume (Figure 3A), and after PD establishment, showing higher alveolar bone loss (Figure 3B). Furthermore, analysis of the sagittal images highlights the greater alveolar bone loss in the interradicular bone area of the M1 (Figure 3D; red arrow) and M2 (Figure 3D; green arrow) after PD establishment, compared to the basal control group (Figure 3C). Moreover, alveolar bone resorption was characterized by an increase in the space between the cement enamel junction (CEJ) and alveolar bone crest (ABC). The distance between the CEJ and ABC in both rat groups are shown in Figure 3C,D with blue arrows. Established PD developed large spaces between the CEJ and ABC (Figure 3D), compared to the basal control (Figure 3C).
At the moment of sacrifice, images of the palate presented differences in gingival recession in the M1 in the different groups (Figures 4A,B). The PD group (Figure 4B) shows a greater apical gingival migration due to the loss of bone support and root exposure, compared to the basal control group (Figure 4A). Also, the PD group (Figure 4B) presented a greater inflammation of the gingiva around the maxillary molars, compared to the basal control group (Figure 4A). Figure 4C shows the results of the analysis of pro-inflammatory cytokine IL-1β from GCF, showing a significantly higher release of IL-1β displayed in the PD group compared to the control group. According to the literature, IL-1β participates in inflammation, immune regulation, and bone resorption in periodontitis, and is a strong stimulator of periodontal tissue destruction12.
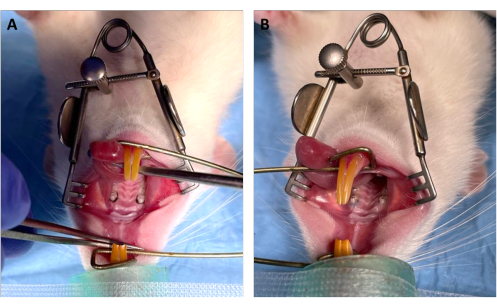
Figure 2: Images of the ligature inserted in the sulcus of the M1 at different times. (A) Rat palate with ligature placement around the M1, 0 days following insertion of the ligature. (B) Rat palate with ligature placement around the M1, 14 days following insertion of the ligature. Please click here to view a larger version of this figure.
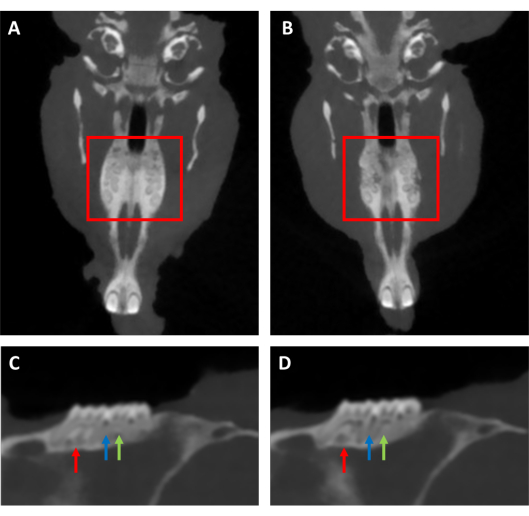
Figure 3: Representative bi-dimensional images of alveolar bone and maxillary molars. Representative bi-dimensional photos obtained by CBCT of alveolar bone of maxillary molars (red square) of (A) the basal control, and (B) established periodontitis (PD) for 14 days with ligature insertion and Pg-LPS injection. Representative sagittal bi-dimensional views of the maxillary molars of (C) the basal control and (D) the PD. The red arrows indicate the interradicular alveolar bone area of the M1, the blue arrows indicate the distance between the CEJ and ABC, and the green arrows indicate the interradicular alveolar bone area of the M2. Please click here to view a larger version of this figure.
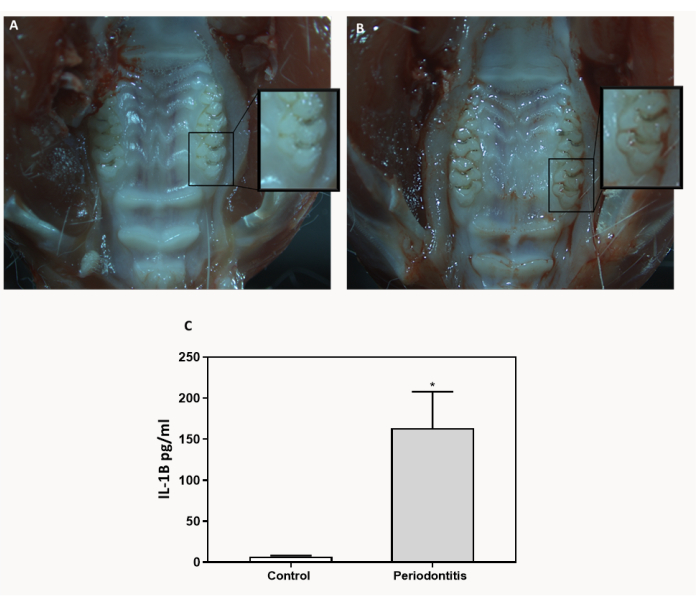
Figure 4: Representative images of the palate. Representative images of the palate after sacrifice of the (A) basal control group and (B) periodontitis (PD) group, treated for 14 days with ligature insertion and Pg-LPS injection. (C) Determination of IL-1β concentrations in the GCF of the basal control group and PD group (n = 9). Data represent the mean ± SEM. Results were statistically compared by Kruskal-Wallis: * p < 0.05 PD group versus basal control group. Please click here to view a larger version of this figure.
Discussion
This method describes the induction of PD in rats following a combined technique of Pg-LPS injections and ligature placement around the M1, revealing that significant changes in the periodontal tissues and alveolar bone could be induced in 14 days following this method.
During this procedure, attention to different critical steps must be provided. During animal anesthesia and procedure preparation, assessing the proper anesthesia during the surgical process is critical for its success, as is ensuring the correct positioning of the animal, stabilizing the open rat mouth with the aluminum mouth gag around the incisors, and avoiding the animals being hurt with the gag and surgical instruments. If oxygen saturation and pulse rate fall, the procedure should be stopped and the animal placed in the lateral decubitus position until reaching normal values. During the ligature position, it is essential that the suture and knot are inserted correctly in the sulcus, considering soft tissue injury should be minimized to prevent pain and inflammation in other areas. Taking into account ethical issues regarding the well-being of the animals, it is essential to monitor the animal's recovery until the effects of the anaesthesia are completely reversed. Pain medication during the first 2 days following the procedure is indispensable. Monitoring the weight and behaviour of the animals is important too, to assess how well the rat tolerates the procedure and ensure it does not exhibit any extreme distress. During the post-procedure protocol of injection of Pg-LPS and adjustment of the ligature to the subgingival tissue around the M1, first of all, it is important to tighten and relocate the ligature in an apical position to create the inflammation. Secondly, it is important to bilaterally inject the Pg-LPS with care, to not cause oral trauma. Also, care must be taken while anesthetizing the animal, and it should be monitored until recovery. During the collection of GCF, the calibrated paper should be maintained at the same position for the same total time, and it is important to insert it at the same gingival crevice around the mesio-palatal M1. During the GCF elution steps, it is important to use the elution buffer immediately after adding the commercial phosphatase inhibitor tablet. One last critical step of the protocol is during CBCT scans; a proper alignment of the samples and protocol of analysis is critical to obtain interpretable results.
The variation of the specific exposure of each animal to Pg-LPS injection and the retentive ligature around the M1 could be included as reasons for not achieving the correct inflammation and the consequent bone resorption. While good results are achieved in the induction of PD by using this procedure, it is important to closely reduce variation between animals by following the protocol closely. One of the most significant modifications of the method is the placing of the retentive ligature around the M1, and not around the M2, the most traditional ligature model in literature13,14,15. The operating procedure for the ligature placement in mice or rats presents technical difficulty, and represents a potential challenge for many researchers due to the small size of the murine oral cavity and teeth11,16. The use of rats and placing the ligature around the M1 facilitated the manipulation and access to the area, which also reduced the stress of the animal during the procedure. No animal suffering was observed during the protocol, but if any rat shows signs of distress, consider removing them from the experiment to prevent suffering. Finally, the most limiting step of the procedure is to avoid the loss of the ligature, which could happen 7-10 days after surgery. To increase and maintain the disease intensity with time, it is important to adjust the ligatures to maintain intimate contact with gingiva tissues, mitigating the variability of intensities on periodontitis induction between animals15. In general, if the procedure is performed correctly, no modifications should be needed, and consistent results will be obtained.
It is important to note that this model presents several limitations. First of all, a technique was developed for the study of PD caused by a traumatic injury (ligature position), which is thought to facilitate the local accumulation of bacteria and thereby enhance bacteria-mediated inflammation and bone loss13,10, with the combination of Pg-LPS injection. But, as a matter of fact, the method does not mimic the natural etiological factors that are responsible for microbiota dysbiosis in human periodontitis and does not mimic several other possible mechanisms by which periodontitis may arise. In addition, murine dental structures are not identical to human15. Further, while the method presented is effective for studying acute PD, it may not reflect the long-term bone loss and inflammatory infiltration characteristics in chronic PD16. In detail with the methodology proposed for the evaluation of alveolar bone loss, the most commonly used method of multidimensional evaluation of bone is micro-CT, which allows the evaluation of external factors and provides three-dimensional images of the bone. Additionally, trabecular bone parameters, bone volume, and bone mineral density can be analyzed without breaking the bones14,17. However, the use of CBCT for the assessment of alveolar bone loss was proposed here (Figure 3) as an alternative to micro-CT; although lower resolution images are obtained, it also provides a useful qualitative and quantitative analysis of periodontitis progression18,19,20. So, CBCT exams provide an accurate method for imaging, more available and accessible than micro-CT, which would facilitate studies of periodontitis induction in rats.
Among the various animal models that have been used to mimic PD in vivo16 to assess tooth-supporting tissues (gingiva and bone) under well-controlled conditions, the ligature-induced PD model has been extensively used in rats, dogs, and non-human primates13. The literature also indicates that, despite being used in some protocols, the use of mice—that represents a convenient, inexpensive, and versatile model—results in a more technical challenge due to the relatively small size of the mouse oral cavity compared to rats13. Compared to other models, the ligature-induced PD rat model offers several advantages, including rapid disease induction, which can begin at a predictable time and culminate in alveolar bone loss within a few days (mice and rats)13. There are other advantages to this method, such as the potential to study periodontal tissue and alveolar bone regeneration, as well as the ability to locate and dissect inflamed gingival tissue in order to assess the level of inflammation15. The method of combining the ligature-induced PD model with the LPS injection adds a local destructive inflammatory response in the periodontium that enhances the loss of connective tissue attachment and alveolar bone resorption generated by the ligature. This additive effect is advisable to increase with the concentration and frequency of LPS injections10. The method reported here presents an optimized protocol of a combination of ligature with Pg-LPS injection, with the advantages and significance of both methods.
The optimization and development of secure and economical in vivo models of PD are critical to facilitate the understanding of the pathogenesis of periodontal disease and testing new therapeutic approaches. The PD model of the combined technique of Pg-LPS injections and ligature placement around the M1 presented here is assessed to be an attractive study model, to investigate host-microbe interactions, inflammation in periodontitis, and alveolar bone resorption. This model identifies the most critical sets of the protocol, describes them in image-based technical detail, and standardizes and optimizes the use of these combined techniques. The use of additional techniques for the evaluation of periodontitis progression could be possible, including histological analyses of both the alveolar bone and surrounding attached gingiva, determination of other cytokines involved in inflammation, and the characterization of oral microbiota. Although the model cannot reflect all aspects of the mechanisms or causes of PD in humans, this study reveals that significant degenerative and inflammatory changes in the periodontal tissues and alveolar bone could be induced at 14 days following the intervention, providing the basis for future preclinical preventive or treatment studies for periodontal disease.
Divulgaciones
The authors have nothing to disclose.
Acknowledgements
This work was supported by Fundació Universitat-Empresa de les Illes Balears (Proof of concept call 2020), by the Instituto de Salud Carlos III, Ministerio de Economía y Competividad, co-funded by the ESF European Social Fund and the ERDF European Regional Development Fund (contract to M.M.B; FI18/00104) and by the Direcció General d'Investigació, Conselleria d'Investigació, Govern Balear (contract to M.M.F.C; FPI/040/2020). The authors thank Dr. Anna Tomás and Maria Tortosa for their help at the experimental surgery and platform of IdISBa. Finally, thanks to ADEMA School of Dentistry for the access to the CBCT scanner.
Materials
| Adsorbent paper point nº30 | Proclinc | 8187 | |
| Aprotinin | Sigma-Aldrich | A1153 | |
| Atipamezole | Dechra | 573751.5 | Revanzol 5 mg/mL |
| Braided silk ligature (5/0) | Laboratorio Arago Sl | 613112 | |
| Buprenorphine | Richter pharma | 578816.6 | Bupaq 0.3 mg/mL |
| Cone-beam computed tomography (CBCT) Scanner | MyRay | hyperion X9 | Model Hyperion X9 |
| CTAn software | SkyScan | Version 1.13.4.0 | |
| Dental explorer | Proclinc | 99743 | |
| Diamond lance-shaped bur | Dentaltix | IT21517 | |
| Food maintenance diet | Sodispain research | ROD14 | |
| Heated surgical platform | PetSavers | ||
| Hollenback carver | Hu-FRIEDY | HF45234 | |
| Hypodermic needle | BD | 300600 | 25G X 5/8” – 0,5 X 16 MM |
| Isoflurane | Karizoo | Isoflutek 1000mg/g | |
| Ketamine | Dechra | 581140.6 | Anesketin 100 mg/mL |
| Lipopolysaccharide derived from P.Gingivalis | InvivoGen | TLRL-PGLPS | |
| Methanol | Fisher Scientific | M/4000/PB08 | |
| Micro needle holter | Fehling Surgical Instruments | KOT-6 | |
| Microsurgical pliers | KLS Martin | 12-384-06-07 | |
| microsurgical scissors | S&T microsurgical instruments | SDC-15 RV | |
| Monitor iMEC 8 Vet | Mindray | ||
| Multiplex bead immunoassay | Procartaplex, Thermo fisher Scientific | PPX-05 | |
| Paraformaldehyde (PFA) | Sigma-Aldrich | 8187151000 | |
| Periosteal microsurgical elevator | Dentaltix | CU19112468 | |
| Phenylmethylsulfonylfluoride (PMSF) | Roche | 10837091001 | |
| Phosphate Buffer Solution (PBS) | Capricorn Scientific | PBS-1A | |
| PhosSTOP | Roche | 4906845001 | Commercial phosphatase inhibitor tablet |
| Plastic vial | SPL Lifesciencies | 60015 | 1.5mL |
| Saline | Cinfa | 204024.3 | |
| Stereo Microscope | Zeiss | Model SteREO Discovery.V12 | |
| Surgical loupes led light | Zeiss | ||
| Surgical scissors | Zepf Surgical | 08-1701-17 | |
| Syringe | BD plastipak | 303172 | 1mL |
| Veterinary dental micromotor | Eickemeyer | 174028 | |
| Xylazine | Calier | 20102-003 | Xilagesic 20 mg/mL |
Referencias
- Carvalho, J. D. S., et al. Impact of citrus flavonoid supplementation on inflammation in lipopolysaccharide-induced periodontal disease in mice. Food and Function. 12 (11), 5007-5017 (2021).
- Nazir, M. A. Prevalence of periodontal disease, its association with systemic diseases and prevention. International Journal of Health Sciences. 1 (2), 72-80 (2017).
- Dumitrescu, A. L., El-Aleem, S. A., Morales-Aza, B., Donaldson, L. F. A model of periodontitis in the rat: Effect of lipopolysaccharide on bone resorption, osteoclast activity, and local peptidergic innervation. Journal of Clinical Periodontology. 31 (8), 596-603 (2004).
- Wang, H. Y., et al. Preventive effects of the novel antimicrobial peptide Nal-P-113 in a rat Periodontitis model by limiting the growth of Porphyromonas gingivalis and modulating IL-1β and TNF-α production. BMC Complementary and Alternative Medicine. 17 (1), 1-10 (2017).
- Guan, J., Zhang, D., Wang, C. Identifying periodontitis risk factors through a retrospective analysis of 80 cases. Pakistan Journal of Medical Sciences. 38 (1), 293-296 (2021).
- Khajuria, D. K., Patil, O. N., Karasik, D., Razdan, R. Development and evaluation of novel biodegradable chitosan based metformin intrapocket dental film for the management of periodontitis and alveolar bone loss in a rat model. Archives of Oral Biology. 85, 120-129 (2018).
- Nishida, E., et al. Bone resorption and local interleukin-1alpha and interleukin-1beta synthesis induced by Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis lipopolysaccharide. Journal of Periodontal Research. 36 (1), 1-8 (2001).
- Graves, D. T., Kang, J., Andriankaja, O., Wada, K., Rossa, C. Animal models to study host-bacteria interactions involved in periodontitis. Bone. 23 (1), 1-7 (2008).
- Struillou, X., Boutigny, H., Soueidan, A., Layrolle, P. Experimental animal models in periodontology: a review. The Open Dentistry Journal. 4 (1), 37-47 (2010).
- Mustafa, H., et al. Induction of periodontal disease via retentive ligature, lipopolysaccharide injection, and their combination in a rat model. Polish Journal of Veterinary Sciences. 24 (3), 365-373 (2021).
- Chadwick, J. W., Glogauer, M. Robust ligature-induced model of murine periodontitis for the evaluation of oral neutrophils. Journal of Visualized Experiments. 2020 (155), 6-13 (2019).
- Cheng, R., Wu, Z., Li, M., Shao, M., Hu, T. Interleukin-1β is a potential therapeutic target for periodontitis: a narrative review. International Journal of Oral Science. 12 (1), 1-9 (2020).
- Abe, T., Hajishengallis, G. Optimization of the ligature-induced periodontitis model in mice. Journal of Immunological Methods. 394 (1-2), 49-54 (2013).
- Jeong-Hyon, K., Bon-Hyuk, G., Sang-Soo, N., Yeon-Cheol, P. A review of rat models of periodontitis treated with natural extracts. Journal of Traditional Chinese Medical Sciences. 7 (2), 95-103 (2020).
- Marchesan, J., et al. An experimental murine model to study periodontitis. Nature Protocols. 13 (10), 2247-2267 (2018).
- Lin, P., et al. Application of ligature-induced periodontitis in mice to explore the molecular mechanism of periodontal disease. International Journal of Molecular Sciences. 22 (16), 8900 (2021).
- Irie, M. S., et al. Use of micro-computed tomography for bone evaluation in dentistry. Brazilian Dental Journal. 29 (3), 227-238 (2018).
- Haas, L. F., Zimmermann, G. S., De Luca Canto, G., Flores-Mir, C., Corrêa, M. Precision of cone beam CT to assess periodontal bone defects: a systematic review and meta-analysis. Dentomaxillofacial Radiology. 47 (2), 20170084 (2018).
- Kamburoğlu, K., Ereş, G., Akgün, C. Qualitative and quantitative assessment of alveolar bone destruction in adult rats using CBCT. Journal of Veterinary Dentistry. 36 (4), 245-250 (2019).
- Sousa Melo, S. L., Rovaris, K., Javaheri, A. M., de Rezen de Barbosa, G. L. Cone-beam computed tomography (CBCT) imaging for the assessment of periodontal disease. Current Oral Health Reports. 7 (4), 376-380 (2020).
