The present technique was performed on a flat surface, with a mouthpiece for global anesthesia (Figure 1A). The mouthpiece should not block access to the medial canthus (Figure 1B). In albino animals, a fiber optic light source was placed below the animal, to assist with the visualization of the veins (Figure 1B). The needle was placed at an angle of approximately 40°, and advanced around 2 mm into the medial canthus (Figure 1C). Injection of trypan blue dye in a P5 albino rat allowed clear visualization of the dye in the retroorbital sinus (Figure 1C).
The retroorbital injection technique described in this protocol was successfully used to administer the tracer biotin-dextran (BDA, 10,000 Da)12. The use of visible tracers in vascular research can, for example, provide an alternative to using radioactive sucrose extravasation from the blood vessels, enabling the use of the same brains for other histological measurements12.
Recently, we have established a neonatal rat model of germinal matrix hemorrhage (GMH)13. In brief, P5 Wistar rats received a single intracranial injection of 0.3 U of collagenase VII into the medial striatum. GMH results in rupture of the vessels in the germinal matrix and is one of the prevalent causes of preterm brain injury and mortality14. To further characterize the GMH model, we used a retroorbital injection of the BDA tracer (Figure 2) to investigate the effects of GMH in blood-brain barrier function and integrity14.
When compared to saline-injected controls (Figure 2A), successful retroorbital injection of the BDA tracer14 allowed assessment of the tracer presence in the brain vasculature 10 min after BDA injection (Figure 2B). This technique was then used to detect penumbra vascular leakage of BDA at the individual blood vessel level in GMH-injured animals (Figure 2C, red arrows) which can then be quantified10.
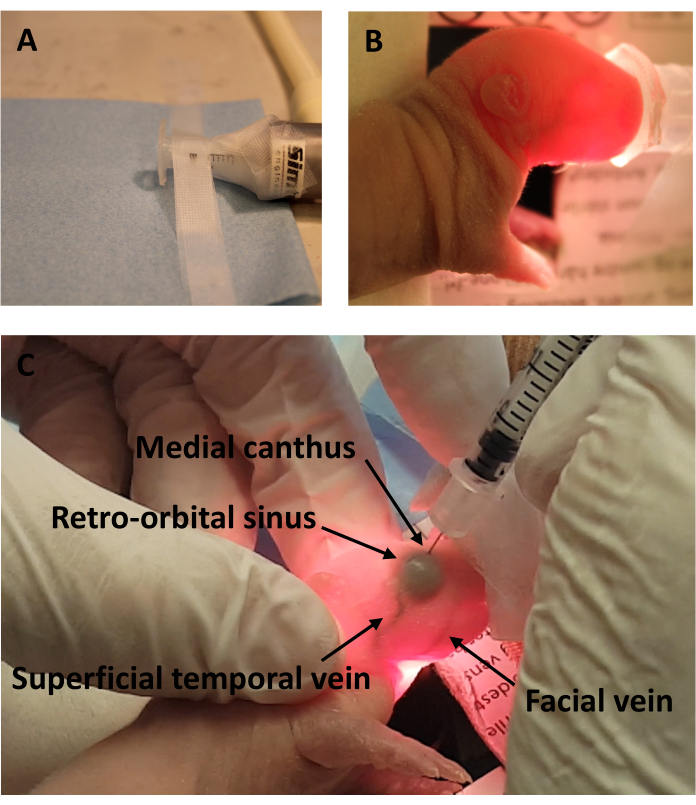
Figure 1: Experimental setup with diagram view of the blood vessels after trypan blue dye administration. (A) Anesthesia setup (B) without and (C) with fiber optic light source. (D) Retroorbital injection of trypan blue dye in the P10 C5BL/6 mouse. (E) Diagram view of the blood vessels in the P5 Wistar rat following trypan blue dye injection. Please click here to view a larger version of this figure.
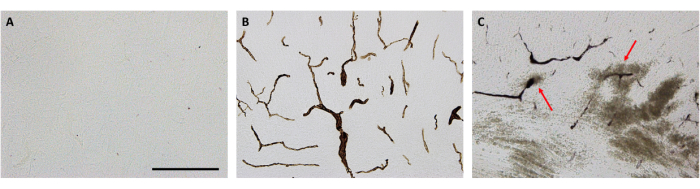
Figure 2: Representative brain micrographs showing the distribution of the BDA tracer. (A) No positive stain in saline-injected control animals. (B) BDA tracer dissolved in saline, at a dose concentration of 2.0 – 2.5 mg per animal was visible within blood vessels of the brain (cortex). (C) BDA tracer leaking into the brain parenchyma following GMH (red arrows). Scale bar = 200 μm. Adapted from Andersson et al., 202114. Please click here to view a larger version of this figure.
