Outcome evaluation
Surgical results were assessed using the Visual Analog Scale (VAS) scores for leg and back pain, Japanese Orthopaedic Association (JOA) Scores, Oswestry Disability Index (ODI) scores, and the modified MacNab standard12,15,17. These indicators were measured pre-operatively and at two days, six months, 12 months, and 24 months post-surgery.
Clinical outcome
All 132 patients who underwent surgery successfully completed the 24-month follow-up. There is a statistically significant difference in scores before and after the operation (P < 0.001). According to the modified MacNab criteria17, all 132 patients exhibited satisfactory results at the final follow-up. Figure 4 and Figure 5 illustrate a clinical example of LE-ULBD performed. Changes in VAS scores, JOA scores, and ODI scores over time are presented in Table 1 and Figure 6. Figure 7 shows the clinical results based on the modified MacNab criteria.
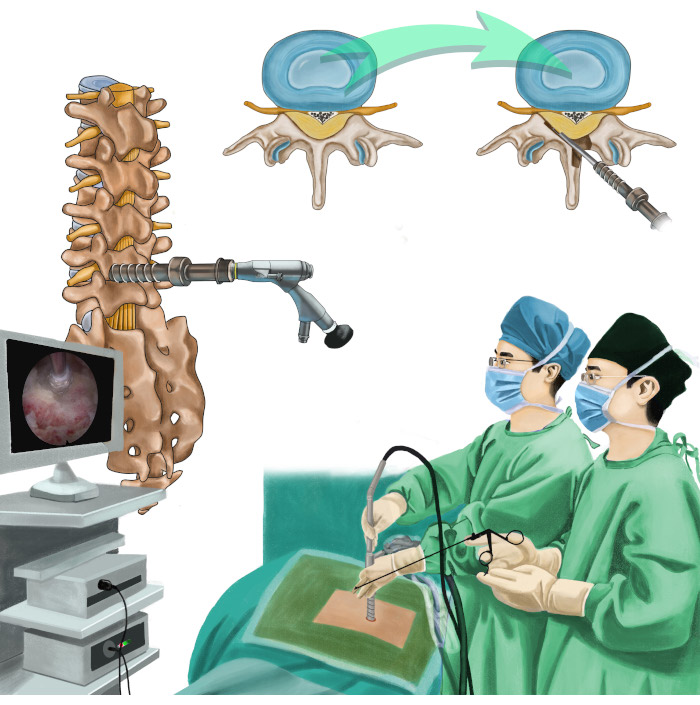
Figure 1: Overview of the protocol. Illustration depicting percutaneous endoscopic unilateral-approach bilateral decompression for lumbar spinal stenosis. Please click here to view a larger version of this figure.

Figure 2: Patient positioning. The patient is positioned in a prone posture on a radiolucent operating table and appropriately flexed. Please click here to view a larger version of this figure.
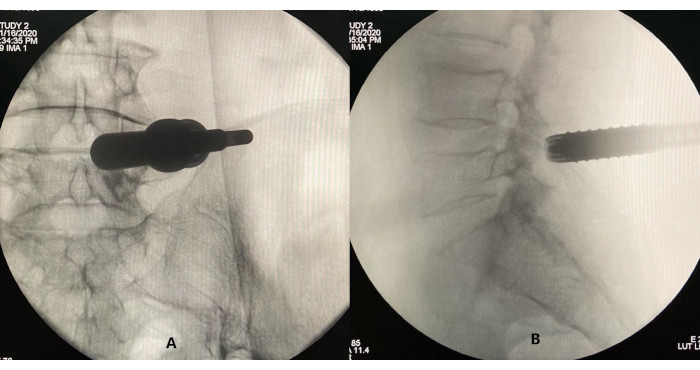
Figure 3: Confirming the correct placement of the working cannula through fluoroscopy. (A) Lateral view and (B) anteroposterior view. Please click here to view a larger version of this figure.
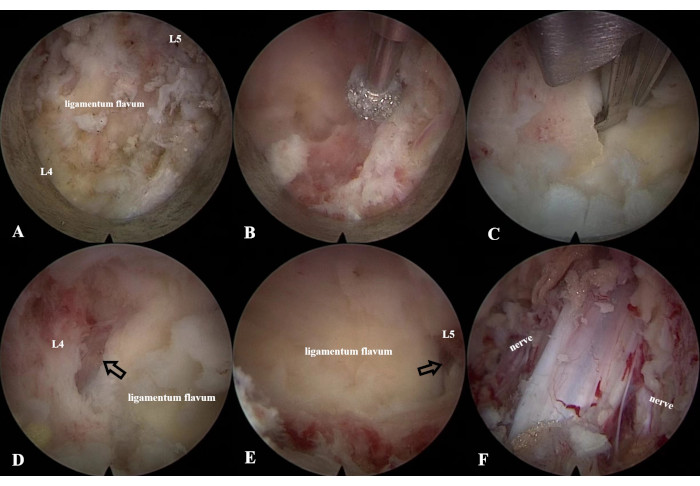
Figure 4: LE-ULBD procedure. (A) Identification of the anatomical structures of the left L4 lamina, L5 lamina, and ligamentum flavum using (B) a diamond bur and (C) an endoscopic Kerrison Rongeur to enlarge the interlaminar window. (D,E) Identification of the cranial and caudal ends of the ligamentum flavum. (F) Decompression of the dural sac and bilateral traversing nerve roots. Please click here to view a larger version of this figure.
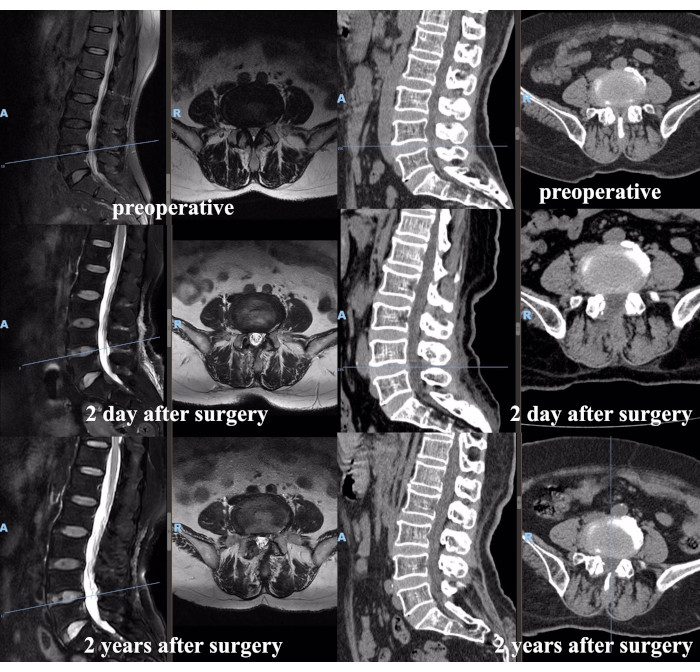
Figure 5: Pre- and post-operative MRI and CT scans of a representative patient. Please click here to view a larger version of this figure.
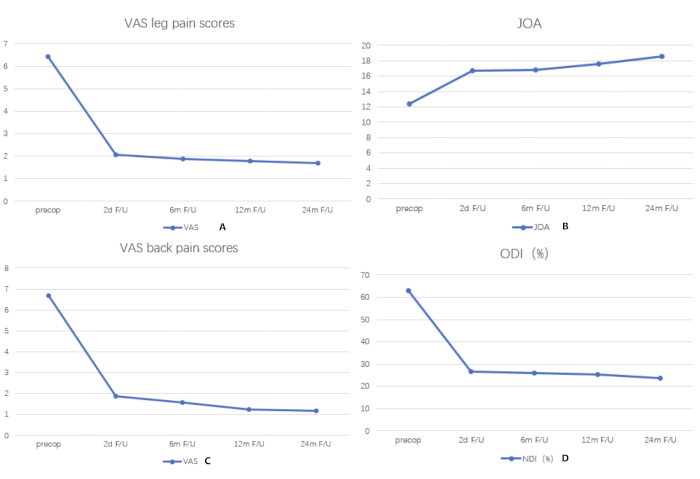
Figure 6: Changes in VAS, JOA, and ODI scores over time. Significant improvements in leg and back VAS scores (A,C), JOA scores (B), and ODI (D) during the follow-up period. The x-axes depict time, and the y-axes depict the scores. Please click here to view a larger version of this figure.
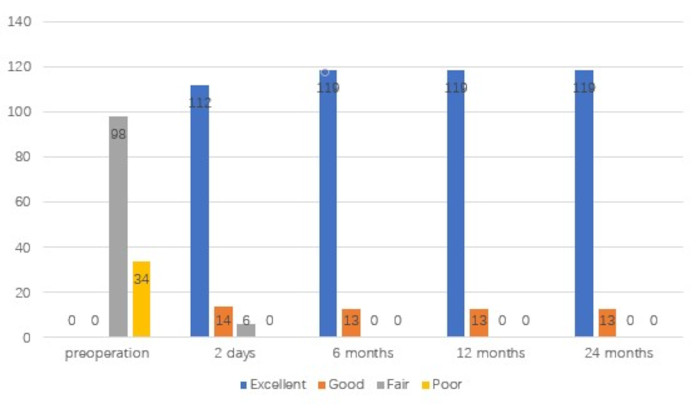
Figure 7: Clinical results assessed according to the modified MacNab criteria. The x-axes depict time, and the y-axes depict the scores. Please click here to view a larger version of this figure.
| Time | VAS leg pain scores | VAS back pain scores | JOA | ODI |
| scores | (%) | |||
| Pre-operative | 6.41 ± 1.33 | 6.68 ± 1.43 | 12.44 ± 1.87 | 62.94 ± 9.52 |
| post-operative | ||||
| 2 d | 2.06 ± 1.12 | 1.89 ± 0.83 | 16.69 ± 1.60 | 26.56 ± 6.93 |
| 6 m | 1.88 ± 1.16 | 1.58 ± 0.88 | 16.81 ± 1.85 | 25.89 ± 6.74 |
| 12 m | 1.78 ± 0.90 | 1.26 ± 0.90 | 17.62 ± 2.91 | 25.44 ± 7.29 |
| 24 m | 1.70 ± 1.10 | 1.17 ± 1.02 | 18.53 ± 2.80 | 23.55 ± 7.46 |
| F value | 789.446 | 1130.254 | 287.64 | 2243.436 |
| P value | P < 0.001 | P < 0.001 | P < 0.001 | P < 0.001 |
| data as (x̄̄ ± s) |
Table 1: Pre- and post-operative scores for 132 patients.
