A Murine Model of Cervical Spinal Cord Injury to Study Post-lesional Respiratory Neuroplasticity
Summary
Respiratory failure is the leading cause of death following a cervical spinal cord injury. Having a reproducible, quantifiable, and reliable pre-clinical animal model of respiratory failure induced by a partial cervical injury will help to understand the subsequent respiratory and non-respiratory neuroplasticity and allow testing putative repair strategies.
Abstract
A cervical spinal cord injury induces permanent paralysis, and often leads to respiratory distress. To date, no efficient therapeutics have been developed to improve/ameliorate the respiratory failure following high cervical spinal cord injury (SCI). Here we propose a murine pre-clinical model of high SCI at the cervical 2 (C2) metameric level to study diverse post-lesional respiratory neuroplasticity. The technique consists of a surgical partial injury at the C2 level, which will induce a hemiparalysis of the diaphragm due to a deafferentation of the phrenic motoneurons from the respiratory centers located in the brainstem. The contralateral side of the injury remains intact and allows the animal recovery. Unlike other SCIs which affect the locomotor function (at the thoracic and lumbar level), the respiratory function does not require animal motivation and the quantification of the deficit/recovery can be easily performed (diaphragm and phrenic nerve recordings, whole body ventilation). This pre-clinical C2 SCI model is a powerful, useful, and reliable pre-clinical model to study various respiratory and non-respiratory neuroplasticity events at different levels (molecular to physiology) and to test diverse putative therapeutic strategies which might improve the respiration in SCI patients.
Introduction
Spinal cord trauma is a common injury observed in the human population with dramatic incidences, such as permanent paralysis. However, the severity of the injury depends on the level and the extent of the initial trauma. Respiratory failure is the leading cause of mortality following upper cervical spinal cord injury (SCI)1. Currently, the only therapeutic treatment is to place the patient under ventilatory assistance. Since few patients can be weaned off the ventilatory assistance2, due to spontaneous recovery which occurs with post-lesional delay, the need to develop new innovative non-invasive therapeutics is urgent3. Having a good standardized pre-clinical model to investigate the effect of a cervical SCI on respiratory insufficiency and therefore, to study the application of putative therapeutic strategies, is essential.
In this technical article, we describe a specific pre-clinical murine model of respiratory impairment induced by a partial cervical SCI at the C2 level. This model is currently used by several laboratories around the world (for reviews: 4-13). However, slight differences in the surgical procedure can be observed among the different investigators to generate this particular cervical injury murine model. The effect of a C2 SCI on the respiratory output was first described in 1895 by Porter14. A cervical hemisection induces a deafferentation of the phrenic motoneurons from their central drive (located in the rVRG in the brainstem, Figure 1A) on the ipsilateral side of injury, leading to a silent phrenic nerve activity and the subsequent diaphragm paralysis. The contralateral side remains intact and allows the animal to survive. Unlike different SCI located in a lower spinal segment (for example a contusive injury at C4 level15), the integrity of the phrenic motoneuron nucleus on both side is preserved. After a cervical C2 injury, some spontaneous activity can be observed on the ipsilateral side (phrenic and diaphragm) due to an activation of contralateral silent synaptic pathways which crossed the spinal midline at the segmental level C3-C6 (Crossed phrenic pathways, CPP, Figure 1B). The activation of the CPP, which is, by definition, a C2 hemisection combined with a contralateral phrenicotomy which induce an ipsilateral partial phrenic nerve recovery, can occur from hours to weeks post-injury16-18. The real beneficial effect of this CPP pathway on the respiratory recovery is limited19 and further investigation and treatment should be developed to improve the magnitude of spontaneous restoration3.
This protocol provides a powerful type of pre-clinical murine model to study respiratory post-lesional plasticity at various levels (respiratory physiology from pre and phrenic motoneurons, interneurons, molecular and cellular, locomotion of the front limb for example) as well as a model to test invasive and non-invasive therapeutic strategies aimed to improve the respiratory and locomotor recovery following C2 partial cervical spinal cord injury.
Protocol
This protocol was approved by the Ethics committee of the RBUCE-UP chair of Excellence (University of Paris Sud, grant agreement No. 246556) and the Université de Versailles Saint-Quentin-en-Yvelines.
1. Preparation of Sterilized Surgical Instruments
- Clean the surgical instruments with laboratory detergent.
- Autoclave the instruments prior to surgery.
- In a surgical session, sterilize the tools by placing the tips in a hot bead sterilizer for 10 min at 180 °C between 2 surgeries.
2. Preparation of Drugs
- Prepare 2 x 1 ml syringes for pre-anesthetic drugs cocktail and post-operation drugs.
- According to the weight of the rat, prepare a syringe with pre-anesthetic drugs: Carprofen (5 mg/kg), Buprenorphine (50 μg/kg), Baytril (5 mg/kg) and Dexmedetomidine (0.5 mg/kg). Complete the volume to 1 ml with Lactated Ringers.
- Prepare in another syringe the reversal for the pre-anesthetic drugs: Atipamezole (500 μg/kg).
3. Anesthesia of the Rat
- Administer subcutaneously to the animal the solution of pre-anesthetic drugs described in step 2.2. Then, put the animal back in cage and wait until the sedative effect appears.
- Place the rat into a closed chamber filled up with 5% isoflurane in 100% O2, and wait until the respiratory rhythm slows down (around 30 sec). Then, remove the rat from the chamber and place it onto the intubation table.
4. Orotracheal Intubation
- Lie the animal on his back, then secure the head by placing a strap attached to his front teeth to the table.
- With a fiber optic light, light up the thoracic space. Then, place a laryngoscope (or a custom made one, Jou et al.20 for details) in the animal’s mouth. Visualize the vocal cords.
- Slide and place an orotracheal guide into the trachea (between the vocal cords). Slide the orotracheal tube (16 G catheter size) on the guide.
- Remove the guide and check with a laryngeal mirror placed at the end of the orotracheal tube for the presence of moisture, confirming the appropriate position of the tube in the trachea and not in the esophagus.
- Connect the tube to a rodent ventilator (683 rodent ventilator, Harvard Apparatus) and adjust the concentration of isoflurane to 2% (in 100% O2).
- Secure the orotracheal tube with surgical tape.
5. Spinal Surgery
- Place the animal in ventral decubitus position on a heated surgical plate, with the nose pointing at 90° angle to the surgeon. Maintain the body temperature around 37.5 °C throughout the surgery.
- Shave the hair with clippers between the scapulas and remove the hair with gauze.
- Clean the skin with betadine, then with 70% alcohol. Repeat this step 3x.
- A toe pinch is performed before beginning of surgery to ensure proper anesthetic depth. Then, perform a lateral skin incision rostro-caudally with scissors between the scapulas.
- Cut the acromiotrapezius muscle rostro-caudally by following the tendon to prevent any bleeding. Then dissociate the rhomboid muscle to access the spinalis muscles (surrounding the vertebra).
- Retract the spinalis muscle from C1 to C3 vertebra. The C2 vertebra is the one with a prominent apophysis.
- Clean the muscle around the dorsal part of the vertebra by using sterile cotton swabs.
- Start to remove carefully the apophysis of C2 with a rongeur. Then, continue meticulously until the dorsal spinal cord is exposed. Ensure that laminectomy is a dorsal hemi laminectomy. Pay careful attention to the dura which encloses the spinal cord, and arteries in the vicinity of this area.
- With a #55 forceps, dissect rostro-caudally the dura along C2, next continue laterally on each rostral and caudal side.
- Sponge up the cerebrospinal fluid.
- Make a lateral section under the cervical dorsal root number 2 with the microscissors. Verify with a micro scalpel that the extent of the lesion is close enough to reach the midline of the spinal cord (see Figure 2A for a dorsal view of the injury). If not, then another cut could be made to complete the injury. In case of bleeding, use sterile cotton swabs. Be careful not to go to the contralateral side, otherwise, the animal will not recover from the injury and will have a respiratory failure.
- Suture the muscles as a protective layer and suture back the skin. Clean the wound with Betadine saturated sterile gauze.
- Turn-off the isoflurane vaporizer and inject the reversal drugs (Atipamezole [500 μg/kg, i.m.]), check the body temperature.
- When the animal starts to breathe against the ventilator, disconnect the tracheal tube from the ventilator, and then remove the orotracheal tube. Place the animal in a heated cage for recovery.
6. Post-surgical care
Following surgery, the animals are monitored continuously to ensure the best environment possible for recovery. Antibiotics (Baytril, 5 mg/kg), anti-inflammatory (Carprofen, 5 mg/kg) and Buprenorphine (50 μg/kg) drugs are given every 12 hr for the first 2 days post-surgery to prevent infections and reduce the occurrence of post-operative pain. Rats have access ad libitum to soft food and water (or jellified water for the 1st post-operative day). Subcutaneous fluids can be used to prevent dehydration on the first few post-operative days. The body weight and the food intake are monitored daily. Their environment is enriched throughout the experiment and time post-injury (dual housing, tubing in their cages).
Representative Results
Extent of Injury
The success and the reproducibility of this particular experimental model are dependent on the experience of each manipulator/surgeon. The subsequent amount of respiratory recovery (phrenic nerve activity and diaphragm activity) following a C2 injury is correlated with the remaining ventrolateral spared white matter21. Since the injury is “handmade” and requires some practice from the surgeon, the extent of each injury has to be checked by histological techniques (fixation of the tissue with paraformaldehyde 4%, frozen tissue slicing, cresyl violet staining) to determine the exact size of damaged tissue (Figure 2B).
Electrophysiological Recordings
Following a C2 SCI, the ipsilateral phrenic nerve activity is abolished (Figure 3A, see Vinit et al.17 for methodology). The contralateral phrenic nerve activity is not affected by the injury and allows the animal survival (Figure 3B). 7 days post-injury, a slight activity can be recorded on the ipsilateral side of some animals, mainly due to the CPP which crossed the midline from the contralateral side (Figure 3A and 3B). Similar results can be observed on the diaphragm activity (Figure 3C and 3D), with a slight activity at 7 days post-injury on the ipsilateral side (Figure 3C). This activity is strengthened over time post-injury and can be observed in all the animals after few months (not shown).
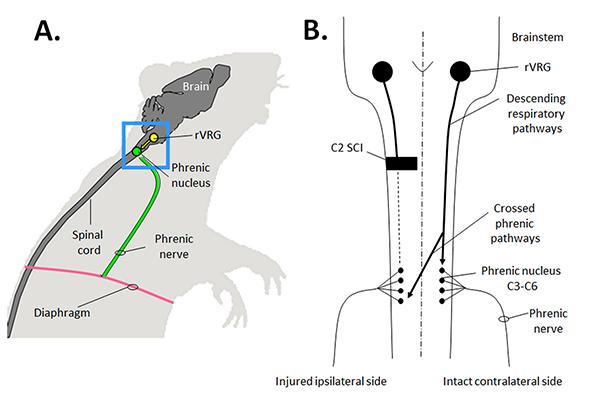
Figure 1. Schematic view of the respiratory anatomy of the rat. A) Lateral view of the main inspiratory organization, with the phrenic pre-motoneurons located in the rVRG (Brainstem) and the phrenic motoneurons located in the phrenic nucleus (C3 to C6), which project their axons to the diaphragm. B) Schematic dorsal view of the effect of a C2 partial injury on the respiratory descending pathways. Note the presence of the crossed phrenic pathways from the contralateral side which cross the midline at the phrenic nucleus segmental level. Click here to view larger image.
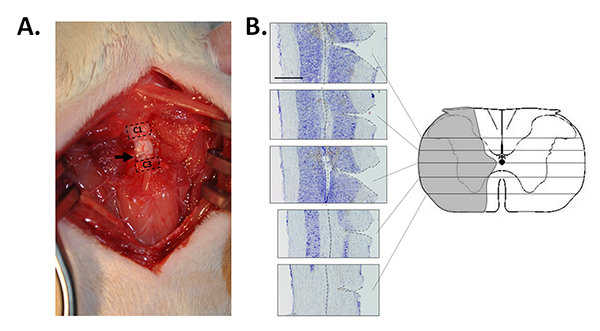
Figure 2. Pictures of the C2 partial injury in the rat. A) Dorsal picture of the surgery site. The arrow shows the site of the injury. Note the absence of the C2 vertebra (dorsal part). B) Reconstruction of the extent of the C2 injury (right picture, extent in gray) from transversal section of the spinal cord (left pictures). Scale bar: 1,000 µm. Click here to view larger image.
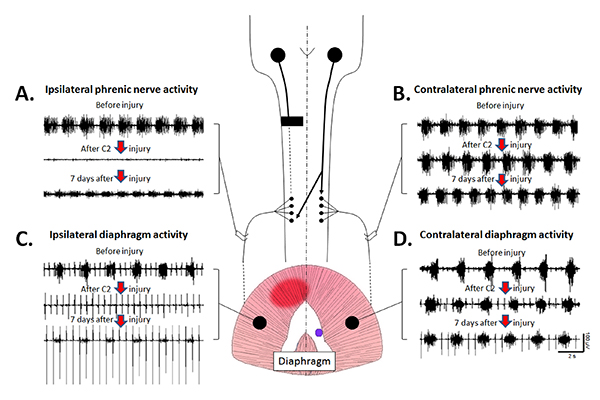
Figure 3. Physiological effects of a C2 injury on the respiratory output. A) A C2 partial injury abolishes the phrenic nerve activity on the ipsilateral side. Note a partial restoration of the ipsilateral phrenic nerve activity at 7 days post-injury due to the crossed phrenic pathway (CPP). B) A C2 injury does not affect the contralateral phrenic nerve activity immediately and at 7 days post-injury. C) The C2 partial injury abolishes the ipsilateral diaphragm activity. A slight activity appears at 7 days post-injury, mainly due to the CPP activity. The rhythmic deflection of the signal observed on the ipsilateral side is due to the artifactual recording of the electrocardiogram. D) Following a C2 injury, the contralateral diaphragm activity remains the same as before the injury, and allows the animal to survive. Click here to view larger image.
Discussion
Technical Difficulties of Making the C2 Injury Model
The C2 injury murine model is an interesting tool to study respiratory post-lesional neuroplasticity. However, the steps needed to produce a reproducible and reliable model are numerous and each one could impact on the outcome of the study. For example, during the intubation process, extreme care is to be taken since the orotracheal tube can produce an inflammation of the trachea, which can lead to diverse complications such as obstructive respiratory failure, in addition to the initial respiratory insufficiency due to the injury itself. Moreover, access to the spinal cord during the surgery procedure could be critical for the recovery of the animal. All the steps (muscle dissection/retraction, dorsal laminectomy, durotomy, the injury itself) have to be performed with extreme caution due to the presence of diverse arteries around the surgery site and into the spinal cord. Extensive bleeding has to be avoided since the post-surgical recovery could be hindered by blood loss, and spinal ischemia can occur in addition to the injury.
Another important part to be aware of is the cleanliness of the instruments and the room where the surgery is performed. Despite the fact that antibiotic drugs are injected into the animal and extreme care about the “pseudo-sterile” conditions were used during surgery, bacterial infection could occur and impact the entire study planned to be performed on this model. For example, systemic inflammation induced by Lipopolysaccharide injection will abolish respiratory neuroplasticity22, and could impact and/or hide the subsequent spontaneous neuroplasticity or the effect of putative restorative strategies. The monitoring of the body temperature throughout this procedure could also participate to the success of making this experimental model. Indeed, hypothermia can act as a neuroprotectant for acute spinal cord injury and can induce some beneficial effects (see Ahmad et al.23 for review).
The cervical 2 section on a murine model is a drastic model in term of handicap (locomotion). It is common to observe a weight loss one week following the injury due to the fact that the animal is hemiplegic and experiences some difficulties to reach food and water. Appropriate help is performed by the post-surgery operator to ensure that the weight loss is approximately 20% of the initial weight (manual feeding). Thus, the end-point of the model is a weight drop of 30% of the initial body weight in a week. Approximately one week post-surgery, the animals slowly recover a partial locomotion allowing them the ability to feed themselves and regain weight (see Lovett-Bar et al.24 for the locomotor recovery study).
At the end of the study, since the C2 injury is “handmade” by the surgeon, for the sake of reproducibility and reliability of the model, the extent of each injury has to be reconstructed by histological techniques. Especially, when respiratory neuroplasticity is studied, Fuller et al.21 showed that the amount of respiratory recovery following a C2 injury was correlated with the remaining spared ventral white matter.
Benefits of using a Rat Model of C2 Injury to Study Respiratory Post-lesional Neuroplasticity
The C2 murine model to study post-lesional respiratory physiology and/or putative strategies to improve/restore the respiratory insufficiency presents many advantages since: 1) rats are readily available from commercial breeders around the world; 2) because of their small size and short lifespan, environmental conditions can be carefully monitored and strictly controlled from birth to adulthood; 3) rats have become the premier model of respiratory neurobiology, replacing the more traditional model, cats. Accordingly, extensive data are available in the literature concerning rat neuroanatomy, neurochemistry, neurophysiology and reflex ventilatory responses, providing context in which to perform and interpret the experimental results; 4) the (relatively) low genetic heterogeneity among commercially available rat strains allows the reduction in the number of animals required to achieve statistical power, and facilitates the comparison of results between different laboratories; 5) rats have a very low mortality rate following cervical spinal cord injury which reduces the number of animals required for statistical power; 6) rats have a very rapid motor recovery rate following cervical spinal cord injury (for example, vs. cats, dogs or primates). Accordingly, the use of rats reduces the length of time the animal requires post-surgical intensive care (e.g., bladder expression, fluid administration, etc.), and minimizes animal subject distress; 7) unlike the locomotor function, the respiratory function does not require animal motivation and is easily quantifiable (diaphragm EMG, phrenic nerve ENG, tidal volume and frequency); 8) one key aspect is the “crossed phrenic phenomenon” (CPP). This particular topic has an extensive published literature using rats as a model (see Goshgarian et al.5,16 for reviews); 9) Rats and humans share many common features in their respiratory control system, which make the rat a good preclinical model to study respiratory insufficiency following cervical SCI12. Moreover, one laboratory has started to successfully develop a C2 hemisection on a mouse model25. This approach provides great enthusiasm about the future use of transgenic animals.
A more clinically relevant animal model is a contusive injury at the cervical level26-28. However, the reproducibility of the injury is inconsistent, mainly due to the location of the descending respiratory pathways and the impossibility to do an extensive contusion (which will drastically reduce the survival rate of the animals). More work has to be done on the elaboration of contusive models to determine the appropriate way to induce a contusive injury with permanent deficits.
Uses for the C2 Injury Murine Model
This C2 SCI model is particularly pertinent for the study of various types of plasticity. For example, molecular and cellular changes from the injured identified pre-motoneurons located in the brainstem (rVRG nucleus)29 as well as the deafferented phrenic motoneurons level30-32 have been studied. The subsequent inflammatory processes33 and the cytoarchitectural changes (perineuronal net changes10) have been investigated following a C2 SCI. The spinal structural changes (implication of substitutive pathways34 and the involvement of spinal interneurons8) or the ultrastructural changes at the diaphragm motor end plate4 also actively participate in the spontaneous restoration of the respiratory activity following a C2 SCI. The most studied topic on the C2 SCI model is the physiological consequences of the initial injury on the entire respiratory system (Tidal volume, frequency in non-anesthetized animals24) and its subsequent spontaneous recovery (on anesthetized preparations i.e. phrenic nerve activity17, diaphragm activity16,17 and more recently, the intercostal activity35). This C2 SCI murine model has also been used to study hindlimb impairment and the subsequent spontaneous recovery and induced recovery following a non-invasive strategy (Intermittent hypoxias24).
Conclusion
The C2 SCI murine model is a powerful and useful pre-clinical model to study respiratory and non-respiratory neuroplasticity and to test diverse putative therapeutic strategies which may improve the respiration in SCI patients.
Divulgaciones
The authors have nothing to disclose.
Acknowledgements
This work is supported by funding from the European Union Seventh framework Programme (FP7/2007-2013) under grant agreement No. 246556 (European project RBUCE-UP), HandiMedEx allocated by the French Public Investment Board. Marcel Bonay was supported by the Chancellerie des Universités de Paris (Legs Poix), the Fonds de Dotation Recherche en Santé Respiratoire, and the Centre d’Assistance Respiratoire à Domicile d’Île de France (CARDIF)
Materials
| Animal | |||
| Male Sprague Dawley Rat | Janvier | 225-250g | |
| Surgical Instruments | |||
| Student Dumont #5 forceps | Fine Science Tool | 91150-20 | |
| Student Standard Pattern Forceps | Fine Science Tool | 91100-12 | |
| Mayo-Stille Scissors | Fine Science Tool | 14013-15 | Curved |
| Student Vannas Spring Scissors | Fine Science Tool | 91500-09 | Straight |
| Spring Scissors – 8 mm Blades | Fine Science Tool | 15025-10 | Straight Blunt/Blunt |
| Friedman Pearson Rongeur | Fine Science Tool | 16121-14 | Curved |
| Dissecting Knife – Fine Tip | Fine Science Tool | 10055-12 | Straight |
| Olsen-Hegar Needle Holder | Fine Science Tool | 12002-14 | Serrated |
| Weitlaner-Locktite Retractor | Fine Science Tool | 17012-11 | 2×3 Blunt |
| Absorbable surgical sutures | Centravet | BYO001 | |
| Equipment | |||
| Hot Bead Steriliser | Fine Science Tool | 18000-45 | |
| Catheter | Centravet | CAT188 | 16 gauge |
| Laryngoscope | |||
| Guide wire | |||
| Laryngeal mirror | Centravet | MIR011 | |
| Lactated Ringers | Centravet | RIN020 | |
| Syringe | Centravet | ||
| Needle | Centravet | ||
| O2 | Air Liquid | I1001M20R2A001 | |
| 683 RodentT Ventilator 115/230V | Havard Apparatus | 55-0000 | |
| Stand-Alone Vaporizer | WPI | EZ-155 | |
| Thin line heated bed | WPI | EZ-211 | |
| Air canister | WPI | EZ-258 | |
| Drugs | |||
| Carprofen | Centravet | ||
| Rimadyl | Centravet | RIM011 | |
| Buprenorphine | Centravet | BUP001 | |
| Baytril | Centravet | BAY001 | |
| Dexmedetomidine | Centravet | DEX010 | |
| Atipamezole | Centravet | ANT201 | |
| Betadine Solution | Centravet | VET002 | |
| Isoflurane | Centravet | VET066 | |
Referencias
- Frankel, H. L., et al. Long-term survival in spinal cord injury: a fifty year investigation. Spinal Cord. 36, 266-274 (1998).
- Ramer, M. S., Harper, G. P., Bradbury, E. J. Progress in spinal cord research – a refined strategy for the International Spinal Research Trust. Spinal Cord. 38, 449-472 (2000).
- Zimmer, M. B., Nantwi, K., Goshgarian, H. G. Effect of spinal cord injury on the respiratory system: basic research and current clinical treatment options. J Spinal Cord Med. 30, 319-330 (2007).
- Mantilla, C. B., Sieck, G. C. Neuromuscular adaptations to respiratory muscle inactivity. Respir Physiol Neurobiol. 169, 133-140 (2009).
- Goshgarian, H. G. The crossed phrenic phenomenon and recovery of function following spinal cord injury. Respir Physiol Neurobiol. 169, 85-93 (2009).
- Nantwi, K. D. Recovery of respiratory activity after C2 hemisection (C2HS): involvement of adenosinergic mechanisms. Respir Physiol Neurobiol. 169, 102-114 (2009).
- Sandhu, M. S., et al. Respiratory recovery following high cervical hemisection. Respir Physiol Neurobiol. 169, 94-101 (2009).
- Lane, M. A., Lee, K. Z., Fuller, D. D., Reier, P. J. Spinal circuitry and respiratory recovery following spinal cord injury. Respir Physiol Neurobiol. 169, 123-132 (2009).
- Seeds, N. W., Akison, L., Minor, K. Role of plasminogen activator in spinal cord remodeling after spinal cord injury. Respir Physiol Neurobiol. 169, 141-149 (2009).
- Alilain, W. J., Horn, K. P., Hu, H., Dick, T. E., Silver, J. Functional regeneration of respiratory pathways after spinal cord injury. Nature. 475, 196-200 (2011).
- Vinit, S. Cervical spinal cord injuries and respiratory insufficiency: a revolutionary treatment. Med Sci (Paris. 28, 33-36 (2012).
- Kastner, A., Gauthier, P. Are rodents an appropriate pre-clinical model for treating spinal cord injury? Examples from the respiratory system). Exp Neurol. 213, 249-256 (2008).
- Vinit, S., Lovett-Barr, M. R., Mitchell, G. S. Intermittent hypoxia induces functional recovery following cervical spinal injury. Physiol Neurobiol. 169, 210-217 (2009).
- Porter, W. T. The Path of the Respiratory Impulse from the Bulb to the Phrenic Nuclei. J Physiol. 17, 455-485 .
- Nicaise, C., et al. Phrenic motor neuron degeneration compromises phrenic axonal circuitry and diaphragm activity in a unilateral cervical contusion model of spinal cord injury. Exp Neurol. 235, 539-552 (2012).
- Goshgarian, H. G. The crossed phrenic phenomenon: a model for plasticity in the respiratory pathways following spinal cord injury. J Appl Physiol. 94, 795-810 (2003).
- Vinit, S., Gauthier, P., Stamegna, J. C., Kastner, A. High cervical lateral spinal cord injury results in long-term ipsilateral hemidiaphragm paralysis. J Neurotrauma. 23, 1137-1146 (2006).
- Fuller, D. D., Johnson, S. M., Johnson, R. A., Mitchell, G. S. Chronic cervical spinal sensory denervation reveals ineffective spinal pathways to phrenic motoneurons in the rat. Neurosci Lett. 323, 25-28 (2002).
- Dougherty, B. J., Lee, K. Z., Lane, M. A., Reier, P. J., Fuller, D. D. Contribution of the spontaneous crossed-phrenic phenomenon to inspiratory tidal volume in spontaneously breathing rats. J Appl Physiol. 112, 96-105 (2012).
- Jou, I. M., et al. Simplified rat intubation using a new oropharyngeal intubation wedge. J Appl Physiol. 89, 1766-1770 (2000).
- Fuller, D. D., et al. Graded unilateral cervical spinal cord injury and respiratory motor recovery. Respir Physiol Neurobiol. 165, 245-253 (2009).
- Vinit, S., Windelborn, J. A., Mitchell, G. S. Lipopolysaccharide attenuates phrenic long-term facilitation following acute intermittent hypoxia. Respir Physiol Neurobiol. 176, 130-135 (2011).
- Ahmad, F., Wang, M. Y., Levi, A. D. Hypothermia for Acute Spinal Cord Injury-A Review. World Neurosurg. , (2013).
- Lovett-Barr, M. R., et al. Repetitive intermittent hypoxia induces respiratory and somatic motor recovery after chronic cervical spinal injury. J Neurosci. 32, 3591-3600 (2012).
- Minor, K. H., Akison, L. K., Goshgarian, H. G., Seeds, N. W. Spinal cord injury-induced plasticity in the mouse–the crossed phrenic phenomenon. Exp Neurol. 200, 486-495 (2006).
- Baussart, B., Stamegna, J. C., Polentes, J., Tadie, M., Gauthier, P. A new model of upper cervical spinal contusion inducing a persistent unilateral diaphragmatic deficit in the adult rat. Neurobiol Dis. 22, 562-574 (2006).
- Golder, F. J., et al. Breathing patterns after mid-cervical spinal contusion in rats. Exp Neurol. 231, 97-103 (2011).
- Lane, M. A., et al. Respiratory function following bilateral mid-cervical contusion injury in the adult rat. Exp Neurol. 235, 197-210 (2012).
- Vinit, S., et al. Axotomized bulbospinal neurons express c-Jun after cervical spinal cord injury. Neuroreport. 16, 1535-1539 (2005).
- Guenther, C. H., Windelborn, J. A., Tubon, T. C., Yin, J. C., Mitchell, G. S. Increased atypical PKC expression and activity in the phrenic motor nucleus following cervical spinal injury. Exp Neurol. 234, 513-520 (2012).
- Mantilla, C. B., Gransee, H. M., Zhan, W. Z., Sieck, G. C. Motoneuron BDNF/TrkB signaling enhances functional recovery after cervical spinal cord injury. Exp Neurol. 247, 101-109 (2013).
- Vinit, S., Darlot, F., Aoulaiche, H., Boulenguez, P., Kastner, A. Distinct expression of c-Jun and HSP27 in axotomized and spared bulbospinal neurons after cervical spinal cord injury. J Mol Neurosci. 45, 119-133 (2011).
- Windelborn, J. A., Mitchell, G. S. Glial activation in the spinal ventral horn caudal to cervical injury. Respir Physiol Neurobiol. 180, 61-68 (2012).
- Vinit, S., Stamegna, J. C., Boulenguez, P., Gauthier, P., Kastner, A. Restorative respiratory pathways after partial cervical spinal cord injury: role of ipsilateral phrenic afferents. Eur J Neurosci. 25, 3551-3560 (2007).
- Dougherty, B. J., et al. Recovery of inspiratory intercostal muscle activity following high cervical hemisection. Respir Physiol Neurobiol. 183, 186-192 (2012).
