We dissected a total of five whole head specimens and 12 temporal bone specimens (n=22 sides) using the described instructions. The different regions of the TC were documented photographically and further analyzed. All regions were explored using 0° and 45° endoscopes. We conducted a complete exploration of all anatomical regions and identified all mentioned anatomical landmarks.
The anatomical structures are illustrated according to the progress of the dissection. Figure 1 illustrates the Prussak space and the malleolar ligaments, whereas Figure 2 demonstrates the anatomy after complete TMF elevation. The wide-angle view allows the visualization of the meso- and hypotympanum as well as parts of the epi-, retro-, and protympanum. In Figure 3, the superior retrotympanum is shown as it appears in a 45° endoscope, while the surgeon is standing on the opposite side of the table. Figure 4 illustrates in detail the protympanum with a dehiscent ICA. After removal of the OC and transcanal atticotomy the epitympanum is inspected until the lateral semicircular canal and the antrum as shown in Figure 5.
No specimen required canaloplasty to perform complete exploration of the tympanic cavity. The identification of the anatomical structures was possible in all specimens using the 0° and 45° scope. However, the complete exploration of the retrotympanum, especially the facial recess and the sinus tympani, was not possible in 27% of the cases (n=6), since these bony bays were too deep to be completely explored.
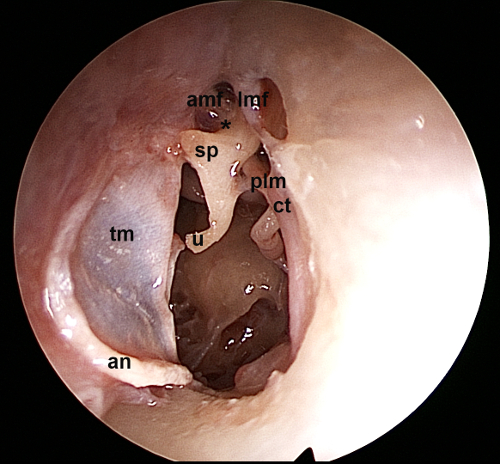
Figure 1. Left ear, 0° endoscope: View of the Prussak space and the surrounding ligamental folds of the malleus. tm: tympanic membrane, an: annulus, u: umbo, sp: short process of malleus, amf: anterior malleolar fold, lmf: lateral malleolar fold, plm: posterior ligament of malleus, ct: chorda tympani, *: Prussak space Please click here to view a larger version of this figure.
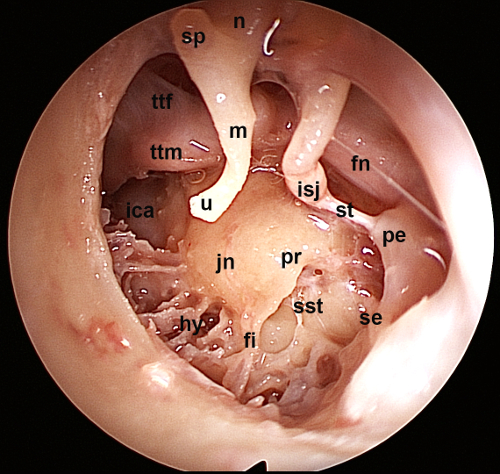
Figure 2. Left ear, 0° endoscope: View of the tympanic cavity after elevation of the tympano-meatal flap. The meso- and hypotympanum as well as parts of the epi-, retro- and protympanum are visualized. pr: promontory, jn: Jacobson nerve, hy: hypotympanum, fi: finiculus, sst: sinus subtympanicus, se: styloid eminence, pe: pyramidal eminence, st: stapedial tendon, isj: incudostapedial joint, fn: facial nerve, u: umbo, m: manubrium, sp: short process, n: neck of the malleus, ttm: tensor tympani muscle, ttf: tensor tympani fold, ica. Internal carotid artery Please click here to view a larger version of this figure.
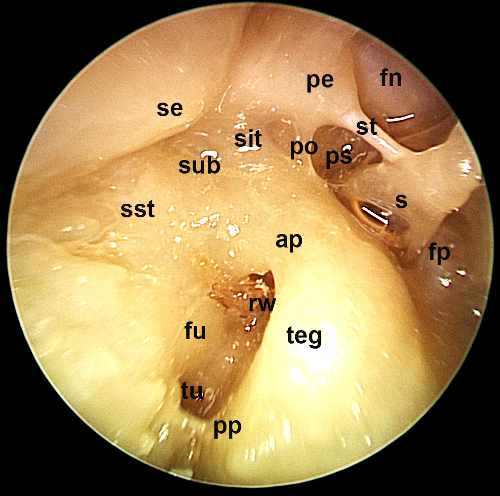
Figure 3. Right ear, 45° endoscope, contralateral position of the surgeon: The superior retrotympanum is illustrated using an angled endoscope. fn: facial nerve, s: stapes, st: stapedial tendon, ps: posterior sinus, fp: footplate, po: ponticulus, pe: pyramidal eminence, sit: sinus tympani, sub, subiculum, se: styloid eminence, sst: sinus subtympanicus, ap: anterior pillar, teg: tegmen, pp: posterior pillar, rw: round window, fu: fustis, tu: subcochlear tunnel Please click here to view a larger version of this figure.
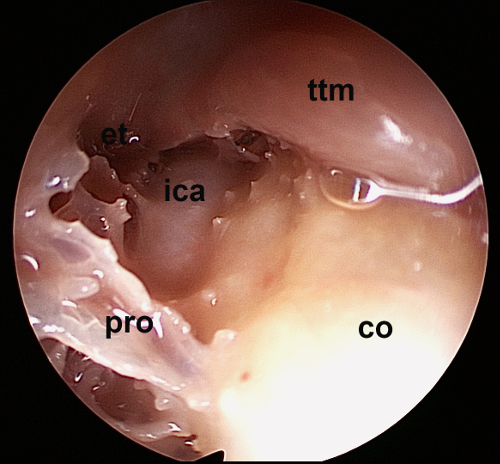
Figure 4. Left ear, 45° endoscope: Detailed view of the protympanum. Note the dehiscent carotid artery. et: Eustachian tube, ica: internal carotid artery, pro: protiniculus, co: cochlea, ttm: tensor tympani muscle Please click here to view a larger version of this figure.
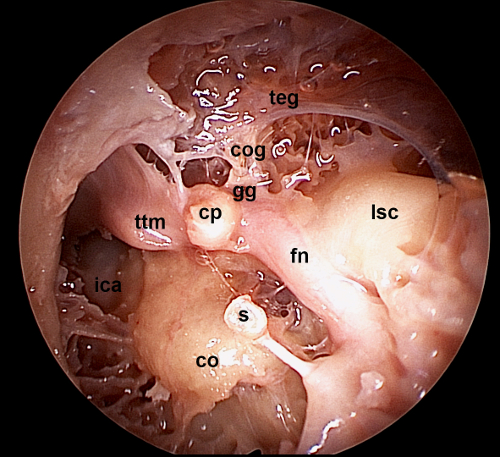
Figure 5. Left ear, 0° endoscope: After removal of the incus and malleolus and curettage of the scutum, a wide overview of the tegmen tympani and the antrum is illustrated here. Note the lateral semicircular canal and the tensor tympani muscle being in one line with the facial nerve crossing. teg: tegmen, cog: COG or transverse crest, gg: geniculate ganglion, cp: cochleariform process, ttm: tensor tympani muscle, lsc: lateral semicircular canal, fn: tympanic segment of facial nerve, s: stapes, co: cochlea, ica: internal carotid artery Please click here to view a larger version of this figure.
