Following a pilot series of seven animals, totally 16 animals were included in the experimental protocol. Two animals died prematurely and were therefore excluded from the final analysis (12.5% mortality). Calculated on 14 animals, immediate aneurysm patency rate during fluorescence angiography was 71.43% in both, the control and modified group. Four aneurysms had to be reopened with consecutive thrombus evacuation and after a repeated fluorescence angiography there was a documented patency in all cases (100%). Aneurysm patency rate in MR- and fluorescence-angiography was 85.72% in the control and 85.72% in the elastase modified group at follow-up after 28 days (two animals showed complete parent artery and aneurysm thrombosis and therefore were excluded from further analysis). Partial thrombosis was observed by analyzing three-dimensional reconstructions of the MR-imaging (Figure 9) in 3 out of the 12 remaining cases. Both groups demonstrated an increase in aneurysm size over time; control group: 6.48 ± 1.81 mm3 at time of creation vs. 19.85 ± 6.40 mm3 at follow-up, p = 0.037 (all statistical tests were performed using the non-parametric Wilcoxon-Mann-Whitney-U test); modified group: 8.03 ± 1.08 mm3 at the time of creation vs. 20.29 ± 6.16 mm3 at follow-up, p = 0.054), showing no significance between both growth rates (p = 0.87). There was no postoperative aneurysm-related hemorrhage. Average duration of the surgical procedure for the control group was 164 ± 10 min (range, 122‒187 min) compared to 201 ± 13 min (range, 158‒250 min) for the modified group. An average of 24 ± 1 interrupted sutures (range, 21‒26) was needed to create aneurysms in the control group, 25 ± 2 (range, 18‒28) stitches in the elastase group. Figure 8 and Figure 9 show histological characteristics as well as CE-3D-MRA morphometric measurements of bifurcation aneurysms on day 28.
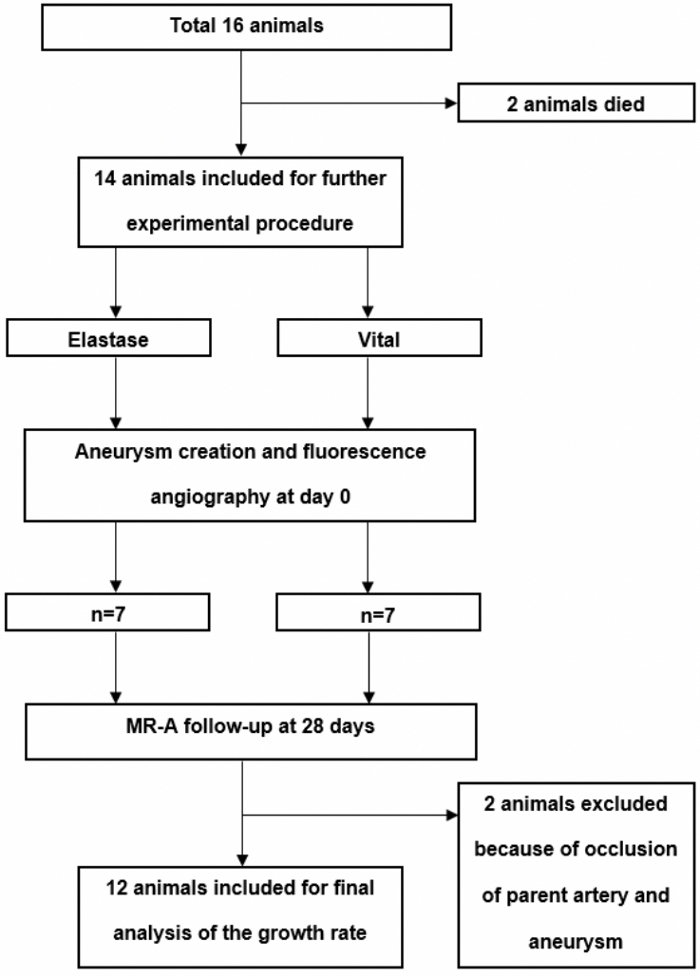
Figure 1: Flow chart of the experimental setting.
In total, after a piloting phase of seven animals, 16 animals were operated and either randomized to control group or elastase pretreatment. Two animals died in the early postoperative course. Please click here to view a larger version of this figure.
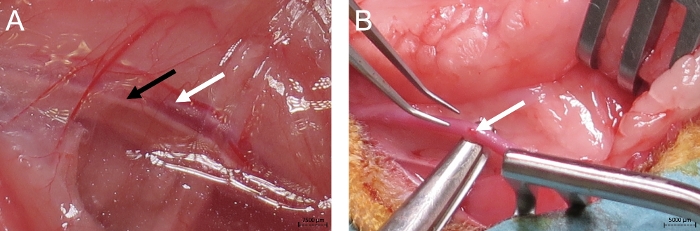
Figure 2: Initial operative step.
Initial operative step, depicting the left carotid artery (white arrow), vagal nerve (black arrow) (A) and the careful separation of the left carotid artery from the vagal nerve distally to avoid laryngeal paresis (B). Please click here to view a larger version of this figure.
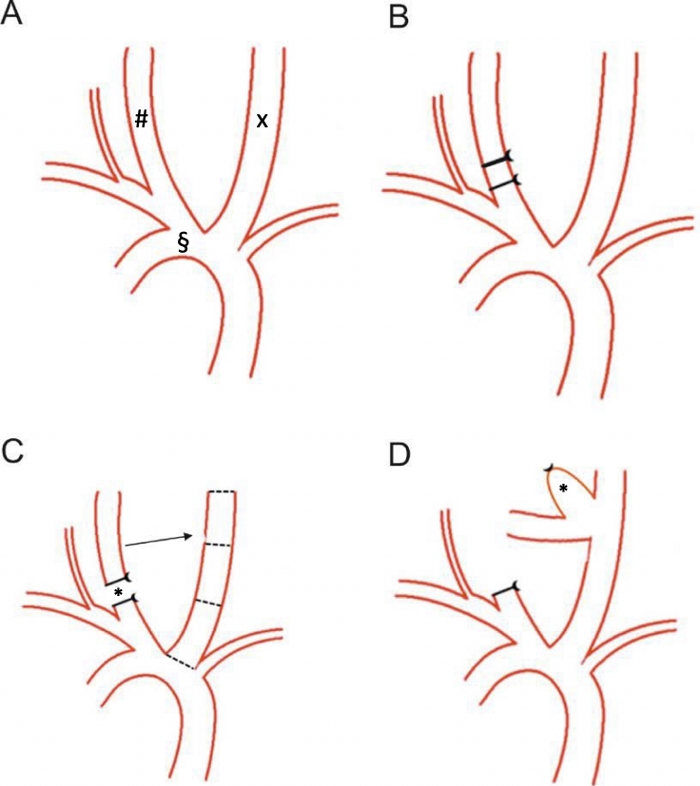
Figure 3: Schematic of the surgical steps.
The aortic arch (§) with both carotid arteries (left carotid artery, x; right carotid artery, #) of a New Zealand White rabbit is shown (A). On the proximal right carotid artery, a 4-0 ligature is performed, and a 6-0 ligature added distally (B). The autologous arterial pouch (*) has already been harvested and the blunt of the right carotid artery is sutured to the distal third of the left carotid artery (C) creating the artificial complex arterial bifurcation (D). Please click here to view a larger version of this figure.
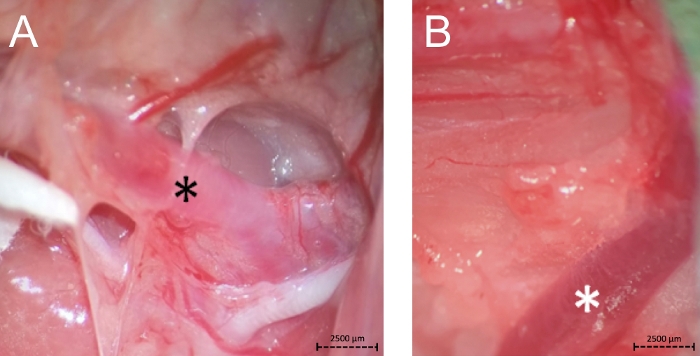
Figure 4: Bifurcation of the left carotid artery as a distal landmark for the left and right side (A, black *) and the internal jugular vein as proximal landmark for preparation of the right side (B, white *). Please click here to view a larger version of this figure.
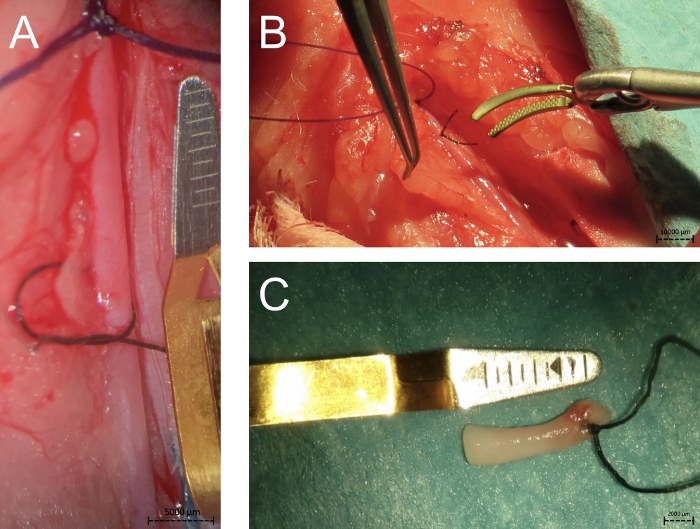
Figure 5: The photographs show the proximal 4-0 and 6-0 ligations of the right carotid artery for creating a new vital arterial pouch (A), the clip placement on the right carotid artery above the two ligatures (B) and the autologous harvested pouch (C). Please click here to view a larger version of this figure.
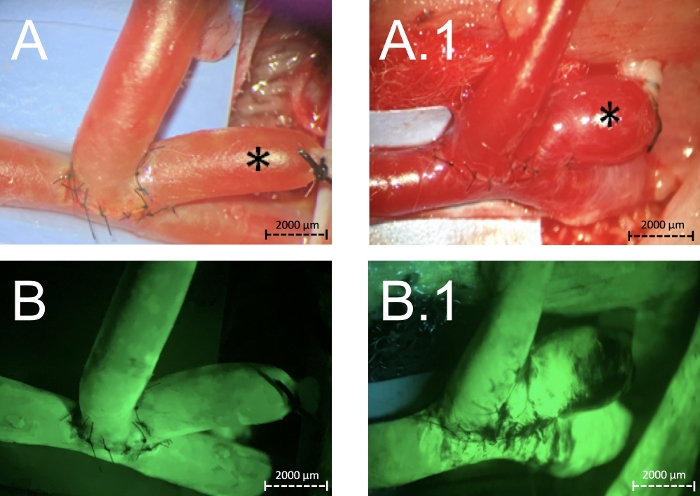
Figure 6: Creation of complex arterial vital (A) and after elastase pretreatment (A.1) bifurcation aneurysms (*).
The same situation after performing a fluorescence angiography showing patency of the parent arteries and of the aneurysms itself (B, B.1). Please click here to view a larger version of this figure.
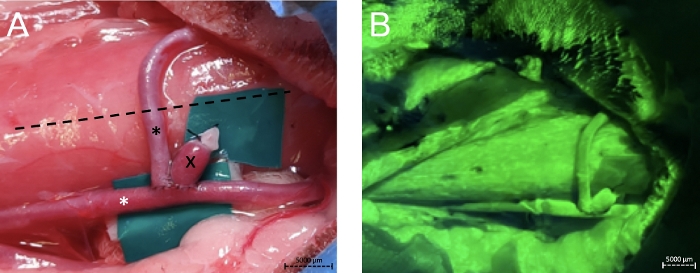
Figure 7: Fluorescence angiography of the vessel complex.
Zoomed out photograph (A) from the operative situs after creation of an elastase pretreated complex bifurcation aneurysm (x). Black * depicts the right common carotid artery, white * the left. The dotted line shows the middle of the neck. The same situation after performing a fluorescence angiography showing patency of the parent arteries and of the aneurysm itself (B). Please click here to view a larger version of this figure.
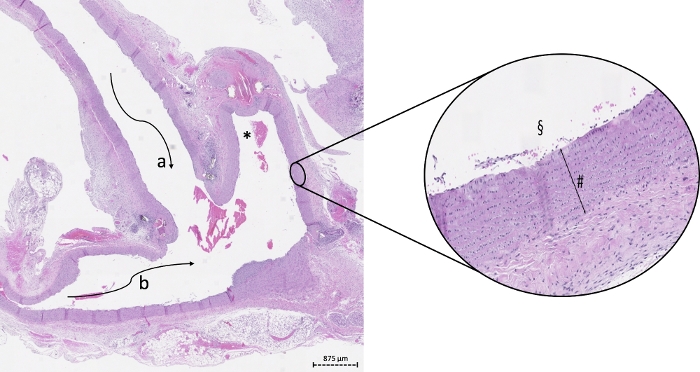
Figure 8: Example of histology on a 2-fold and 20-fold digital zoom of a vital aneurysm in bifurcation constellation.
The vital wall (#) is marked by high cell density. * depicts the lumen of the aneurysm, a the lumen of the right, b the lumen of the left proximal carotid artery, § the magnified luminal side of the aneurysm. Please click here to view a larger version of this figure.
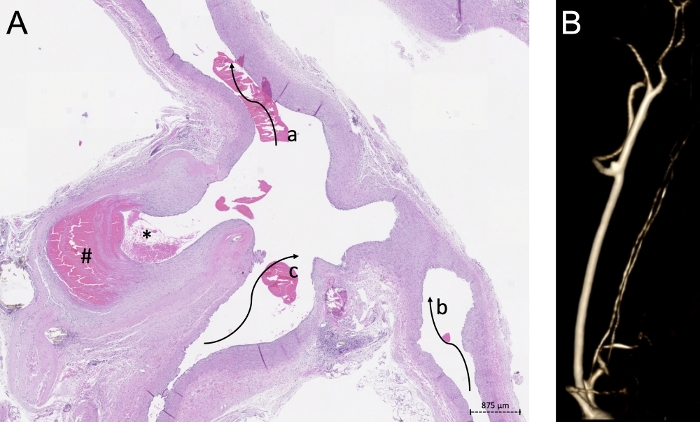
Figure 9: Histological findings correlated with MR-imaging.
(A) Example of 2-fold digital zoom of modified arterial pouch sewn on an arterial bifurcation The partial thrombosed aneurysm dome (#), the lumen of the aneurysm (*), the lumen of the left proximal (b) and distal (a) as well the lumen of the right carotid artery (c) is shown. (B) depicts the CE-3D-MRA morphometric measurements of the aneurysm after 28 days. Please click here to view a larger version of this figure.
| n | Operation Time (min) |
Weight (g) | # of Sutures (n) |
Diameter Parent Artery proximal to the Aneurysm (mm) |
Suture Time (min) |
Diameter Parent Artery distal to the Aneurysm (mm) |
Diameter Aneurysm baseline (mm) |
Volume baseline (mm3) |
Diameter Aneurysm follow-up (mm) |
Volume follow-up (mm3) |
|
| Vital pouches | |||||||||||
| 1 | 187 | 4100 | 24 | 2.5 | 54 | 2.8 | 1 | 1.96 | 1.5 | 5 | |
| 2 | 183 | 4200 | 24 | 3.3 | 53 | 2.9 | 1 | 2.35 | 2.8 | 7.73 | |
| 3 | 163 | 3800 | 26 | 3.4 | 66 | 3 | 1.5 | 4.71 | 3.1 | 28.03 | |
| 4 | 122 | 3600 | 22 | 2.8 | 42 | 2.8 | 2 | 6.28 | 3.2 | 47.37 | |
| 5 | 180 | 3700 | 24 | 3.2 | 45 | 3 | 2 | 10.99 | 2 | 15.82 | |
| 6 | 149 | 3700 | 21 | 2.3 | 47 | 2.2 | 2 | 12.56 | 3.1 | 15.11 | |
| Mean ± SEM | 164.00 ± 10.22 | 3850.00 ± 99.16 | 23.50 ± 0.72 | 2.92 ± 0.19 | 51.17 ± 3.52 | 2.78 ± 0.12 | 1.58 ± 0.201 | 6.48 ± 1.81 | 2.62 ± 0.29 | 19.85 ± 6.40 | |
| Elastase pouches | |||||||||||
| 1 | 158 | 3400 | 26 | 2.9 | 76 | 2.6 | 2 | 9.42 | 2.1 | 12.26 | |
| 2 | 180 | 3400 | 27 | 3.5 | 43 | 2.8 | 2 | 10.99 | 3.3 | 46.16 | |
| 3 | 250 | 3900 | 27 | 3.5 | 70 | 3.2 | 1.4 | 6.59 | 2.2 | 10.1 | |
| 4 | 208 | 4200 | 28 | 3 | 45 | 2.6 | 2 | 9.42 | 2.6 | 24 | |
| 5 | 192 | 3660 | 18 | 2.8 | 53 | 2.8 | 2 | 8.24 | 2.7 | 4.03 | |
| 6 | 217 | 3200 | 24 | 2.7 | 58 | 2.8 | 1.5 | 3.53 | 2.2 | 25.16 | |
| Mean ± SEM | 200.83 ± 13.00 | 3626.67 ± 151.58 | 25.00 ± 1.51 | 3.07 ± 0.14 | 57.50 ± 5.43 | 2.80 ± 0.09 | 1.82 ± 0.12 | 8.03 ± 1.08 | 2.52 ± 0.19 | 20.29 ± 6.16 | |
| p-value | 0.06 | 0.22 | 0.14 | 0.46 | 0.42 | 0.5 | // | 0.46 | // | 0.87 | |
Table 1: Surgical characteristics and CE-3D-MRA morphometric measurements.
