We initiated our investigation by examining AOA's effect on embryos' developmental capability. A schematic illustration of the experimental design is shown in Figure 1A. Before the spermatozoon injection, the oocytes underwent either AOA (A-ICSI) or remained untreated (ICSI). Detailed data on embryonic development is presented in Table 1. The results revealed no significant differences in cleavage, blastocyst, or birth rates between the A-ICSI and ICSI groups (P > 0.05; Figure 1B). These findings indicate that AOA using 10 mM SrCl2 for 20 min did not affect the developmental potential of the embryos.
It was previously reported that there were no discernible differences in the developmental efficiency of ROSI embryos selected either by FACS or by direct visual examination under a microscope22. Our experiments employed FACS technology to identify RS (Figures 2A,B). Under the microscope, mouse round spermatids were approximately 10 µm in diameter and displayed a protrusion-like nucleolus structure in the middle (Figure 2C). We posit that selection through FACS is more accurate than direct visual examination under a microscope. Additionally, the literature supports the direct exploration of RS through morphological differences. ROSI embryos were generated using two distinct methods: the A-ROSI group, where oocytes were subjected to AOA before the round spermatid injection, and the ROSI-A group, where oocytes were subjected to AOA after the round spermatid injection. The schematic diagram of the experimental design is shown in Figure 1C. Notably, no significant differences in the cleavage and blastocyst rates were found among the A-ROSI, ROSI-A, and ICSI groups (P > 0.05; Figure 1D). The blastocyst rates of the A-ROSI, ROSI-A, and ICSI groups were significantly higher than those of the activation group (P < 0.05; Figure 1D). However, the birth rate of the ROSI group was lower than that of the ICSI group, irrespective of whether the oocytes were activated before or after injection (P < 0.05; Figure 1D). Importantly, the birth rate of the A-ROSI group was slightly higher than that of the ROSI-A group (Figure 1D). Further details on embryo development data are presented in Table 1.
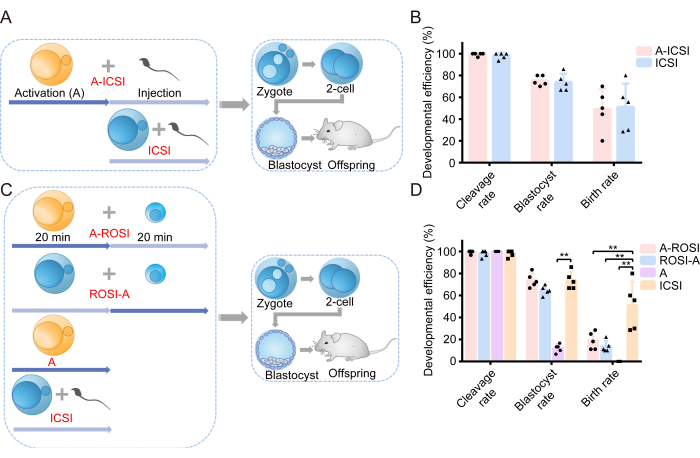
Figure 1: ROSI embryos displayed reduced developmental efficiency compared to ICSI embryos. (A) Schematic illustration of the experimental protocol assessing the effect of activation on ICSI embryonic development. Blue = Oocytes were not activated; Yellow = Oocytes were activated. (B) Developmental efficiency of embryos derived from A-ICSI and ICSI. (C) Schematic illustration of the experimental protocol for generating different types of embryos. (D) Developmental efficiency of embryos derived from A-ROSI, ROSI-A, A, and ICSI. **, P < 0.01. Abbreviations: A= Activation E= Embryonic day; ROSI= Round spermatid injection; ICSI= Intracytoplasmic sperm injection. The error bars show standard deviation. The comparison of rates is conducted using the chi-square test. Please click here to view a larger version of this figure.
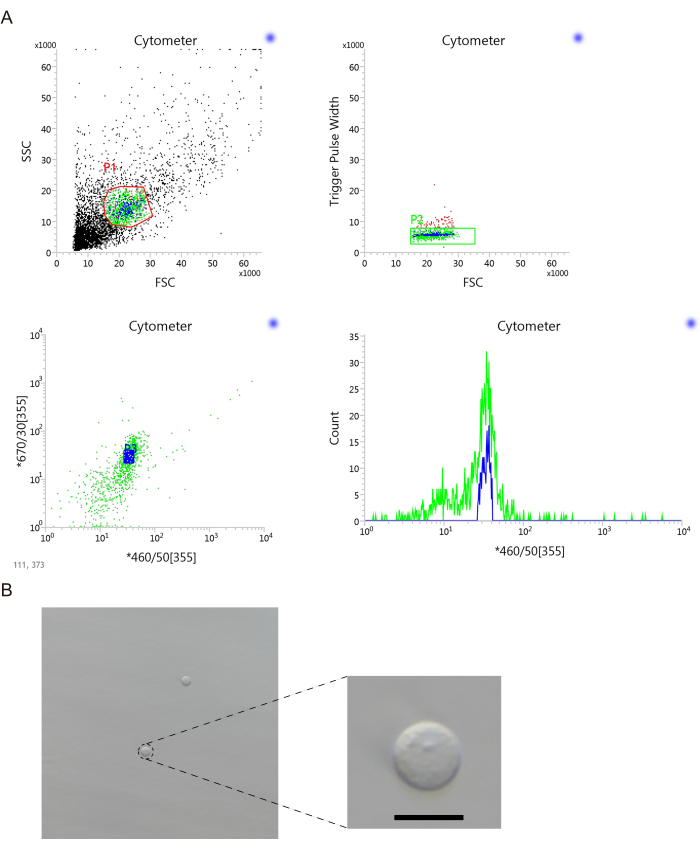
Figure 2: Round spermatids were selected via flow cytometric sorting. (A) A flow cytometric sorting diagram was utilized for the selection of round spermatids. (B) Representative images showcasing the selection of round spermatids. Scale bar: 10 µm. Abbreviations: FSC = Forward scatter; SSC = side scatter; 355 is the excitation wavelength; 460/50 and 670/30 are two detection channels under 355 wavelength laser. Please click here to view a larger version of this figure.
| Groups | Pre-implantation development | Post-implantation development | |||
| Replicates | Cleavage rate (%) | Blastocyst rate (%) | 2-cell embryos transferred/ No. of recipients | Birth rate (%) | |
| A-ICSI | 5 | 99.33 (149/150) | 75.17 (112/149) | 49/5 | 48.98 (24/49) |
| A-ROSI | 5 | 99.33 (149/150) | 73.83 (110/149) | 44/5 | 18.18 (8/44) ** |
| ROSI-A | 5 | 98.00 (147/150) | 64.63 (95/147) | 45/5 | 13.33 (6/45) ** |
| Activation | 5 | 100.00 (150/150) | 12.00 (18/150) ** | 51/5 | 0.00 (0/51) ** |
| ICSI | 5 | 98.00 (147/150) | 73.47 (108/147) | 46/5 | 52.17 (24/46) |
Table 1. The developmental efficiency of embryos derived from different groups.
Supplementary Table 1. The proportion of different cell populations sorted by flow cytometry.P3 part is round spermatids. Please click here to download this File.
