In contrast to the PVL (protocol steps 2,3,4, and 5), the mice that were subjected to the ALPPS (steps 2,3,4,5, and 6) surgical intervention demonstrated a heightened proclivity towards cellular proliferation. Figure 2 delineates the ischemic demarcation of the middle liver lobe following portal vein ligation, along with the visual field during liver transection, which represents a key distinction between ALPPS and PVL. Notably, the levels of inflammatory mediators, including (Tumor Necrosis Factor-α (TNF-α), interleukins, and hepatic growth factor (HGF), within the hepatic tissue, surpass those observed in the PVL group. This is seen in Figure 4C where the ALPPS group had higher IL-6 levels than the PVL group, suggesting that inflammation may be involved in rapid liver regeneration. To further substantiate these findings, a comparative analysis of the liver-to-body weight ratio and the expression levels of ki67, a widely recognized marker of cellular proliferation, within the hepatic tissue, two days post-operatively, has been done. Figure 4A,B and Figure 5 show that the liver in the ALPPS group demonstrates enhanced proliferative capacity.
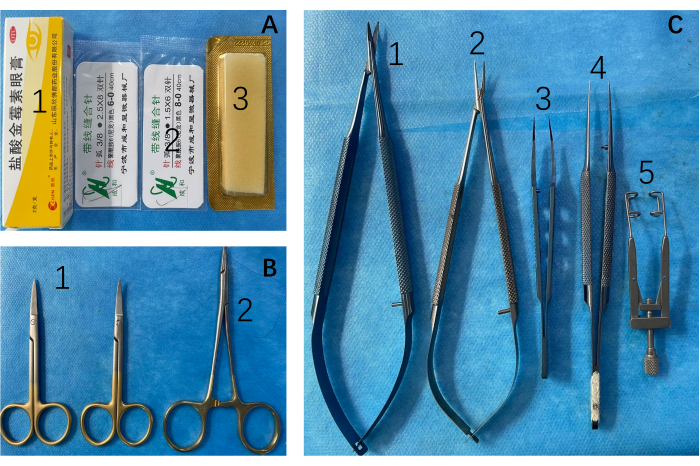
Figure 1: Surgical instruments and consumables. (A) 1: Topical antibiotics for incisions; 2: 6-0, 8-0 Surgical sutures; 3: hemostatic gelatin sponges. (B) 1: Scissors and 2: needle holders are employed for the incision and suturing of the abdominal cavity. (C) Microscopic procedures necessitate the use of 1: scissors, 2: forceps, 3, 4: dissecting forceps, 5: abdominal retractors. Please click here to view a larger version of this figure.
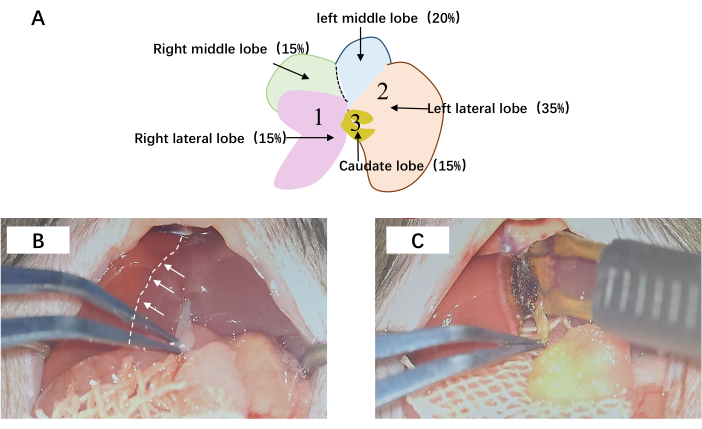
Figure 2: The hepatic surgical procedure. (A) Portal vein ligation and transection. The sequential ligation of 1, 2, and 3 is meticulously executed, concomitantly with the meticulous division of the hepatic parenchyma within the middle lobe. (B) The demarcation line of the middle lobe is visually depicted by the presence of a white dashed line. (C) Subsequent to microscopic examination, the liver is meticulously dissected along the delineated ischemic boundary. Abbreviations: RLL = right lateral lobe; LML = left middle lobe; LLL = left lateral lobe; RML = right median lobe. Please click here to view a larger version of this figure.
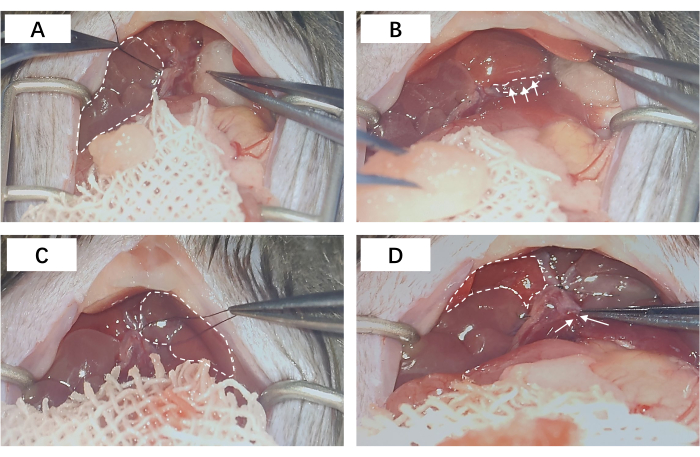
Figure 3: Portal vein ligation. (A) The portal vein ligation of the right lateral lobe; the dashed area corresponds to the ligated RLL. (B) The portal vein ligation of the left middle lobe and the left lateral lobe; the dashed line area represents the entrance for ligation of the portal vein branches. (C) The dashed area corresponds to the ligated LML and LLL. (D) The portal vein ligation of the caudate lobe; the dashed region delineates the physiologically perfused right middle lobe, whereas the arrows demarcate the portal vein branch of the caudate lobe, discreetly ensconced within the hepatic parenchyma. Abbreviations: RLL = right lateral lobe; LML = left middle lobe; LLL = left lateral lobe. Please click here to view a larger version of this figure.
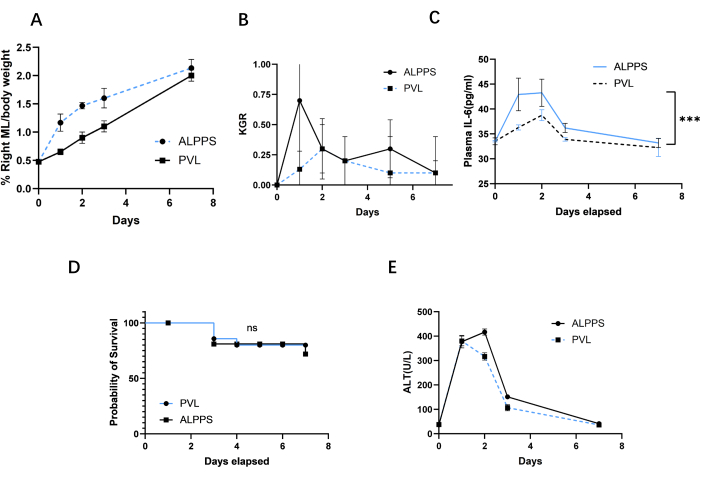
Figure 4: Comparison of future liver remnants, kinetic growth ratio, survival rate, and plasma ALT during the first week between ALPPS and PVL. (A) FLR was assessed in the PVL group and PVL+T group post surgery. (B) KGR was assessed as the gain of LMR/bodyweight ratio per day. KGR in the ALPPS group increased rapidly within 2 days after surgery, then gradually decreased, but was still higher than that in the PVL group. (C) Plasma IL-6 between PVL and ALPPS. (D) Survival curve after PVL and ALPPS. (E) Plasma AST between PVL and ALPPS. Abbreviations: FLR = future liver remnants; PVL = portal vein ligation; PVL + T = portal vein ligation + transection; KGR = kinetic growth ratio; LMR = left ; ALPPS = associating liver partition and portal vein ligation for staged hepatectomy; ALT = Alanine aminotransferase. Please click here to view a larger version of this figure.
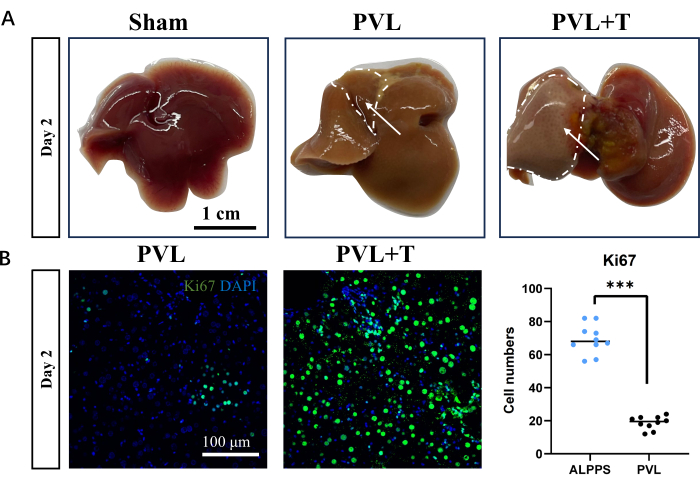
Figure 5: Markers and morphology of liver regeneration following portal vein ligation or combined transection. (A) Hepatic morphology was assessed in the sham surgery group, PVL group, and PVL+T group 2 days post surgery. The delineated area signifies the regenerated hepatic lobes; scale bar = 1 cm. (B) Fluorescence staining unveiled heterogeneous levels of cellular proliferation across distinct surgical cohorts of the liver; scale bar = 100 µm, ***P < 0.001. Please click here to view a larger version of this figure.
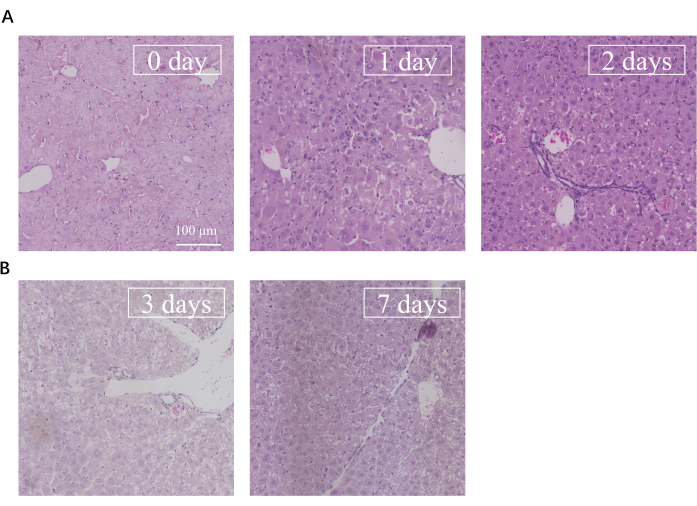
Figure 6: HE images from portal vein to central vein after ALPPS. (A) The liver of ALPPS HE staining from 0 day to 2 days. (B) HE staining from 3 days to 7 days. Scale bar = 100 µm. Abbreviations: HE = hematoxylin and eosin; ALPPS = associating liver partition and portal vein ligation for staged hepatectomy. Please click here to view a larger version of this figure.
