A TMS single-pulse device with a 70 mm figure-8 coil was employed for all stimulation sessions. MEPs were acquired using standard amplifiers and software installed on a local computer. All MEPs were obtained by attaching three electrodes targeting the Abductor Pollicis Brevis muscle (APB). The main hypothesis tested was that the Sol method would produce larger amplitudes and AUC compared to unbraided hair. To do this, we used ANOVAs using separate 2 x 9 (Pre/Post x Subject) tests. We predicted larger amplitudes and AUC following braiding compared to no braiding. We also examined variability across the 30 trials in each participant and predicted that the Sol method would decrease variability.
We first ran a 2 x 9 Repeated-Measures ANOVA using Pre/Post and Subject as factors over the 30 TMS pulses sampling at 1,000 Hz for 100 ms post TMS trigger. It is noted that the sample is small and caution must be taken in interpreting these results. It was found using a Kolgoromov-Smirnov test that the data were normally distributed (all p's > .05). For Peak Amplitude, it was found that there was no overall interaction (F(8,232) = 1.82, p = 0.08). We then examined the Main Effect of Pre/Post and found that there was a significant difference (F(1,29) = 8.70, p = 0.006) with the Post Amplitude being 116.99% higher than the Pre. While Subject was significant (F(8,232) = 2.41, p = 0.016), we were interested in the number of subjects in which braiding made a difference. It was found that Amplitude increased in 7/9 Subjects, and in 3, the Pre/Post difference was significant (t(8), p's per Subject= 0.01, 0.01, 0.02, 0.12, 0.55, 0.60, 0.71, 0.76, 0.81; Figure 5).
We ran a similar 2 x 9 ANOVA for AUC (Figure 5). There was no interaction (F(8,232) = 1.30, p = 0.24). There was a significant Pre/Post difference (F(1,29) = 7.39, p = 0.01). The Post AUC was 108.12% greater than Pre AUC. There was also a Subject significant difference (F(8,232) = 2.47, p = 0.01). In 7/9, there was an increase in AUC, and in 2, the Pre/Post difference was significant (t(8), p's per Subject = 0.01, 0.04, 0.10, 0.11, 0.48, 0.71, 0.86, 0.87, 0.96).
Analyzing the variability in Amplitude, it was found that there was non-significant interaction (F(8,232) = 1.41, p = 0.19; Figure 5). There was a trend for less variability looking at Pre/Post scores (F(1,29) = 2.81 p = 0.10). Following braiding, variability was reduced 10.36%. There was no significant effect for Subject (F(8,232) = 1.26, p =. 27). AUC was analyzed for variability and there was no significant interaction (F(8,232) = 1.28,p = 0.25). Pre/Post (F(1,29) = 0.98, p = 0.33) and Subjects (F(8,232) = 1.06, p = 0.39) were non-significant as well. These data indicate a number of important significant findings and trends. The increased amplitude and AUC demonstrate that Motor Threshold (i.e., the level of TMS needed to induce an MEP) would likely be reduced with appropriate braiding. Cornrowing also increased reliability as variability was decreased (though not significantly). Finally, signal strength is increased, which may make clinical applications more efficacious, though this claim is highly speculative.
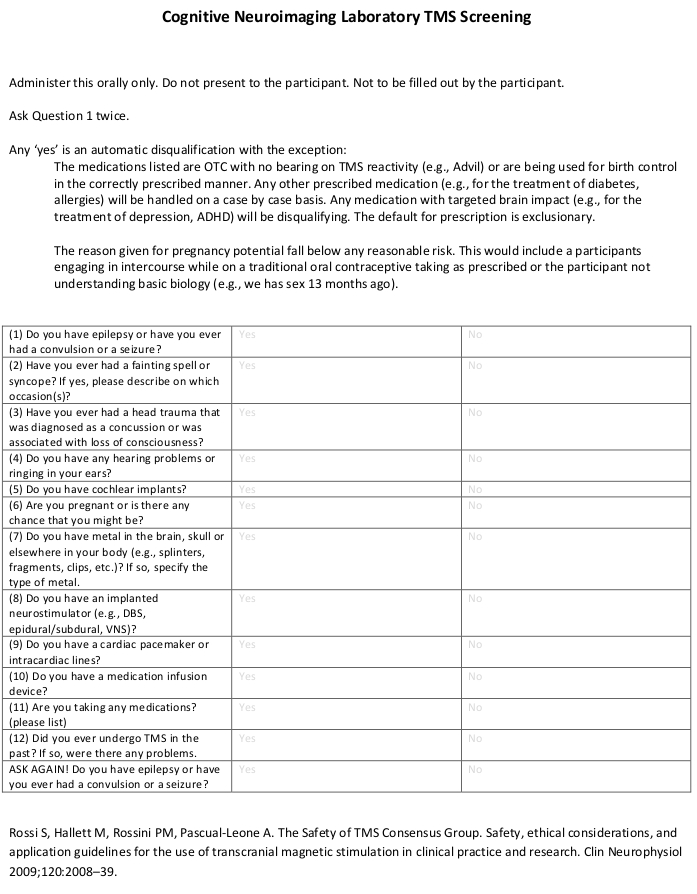
Figure 1: Screening. Typical screening used to ensure patient safety. Please click here to view a larger version of this figure.
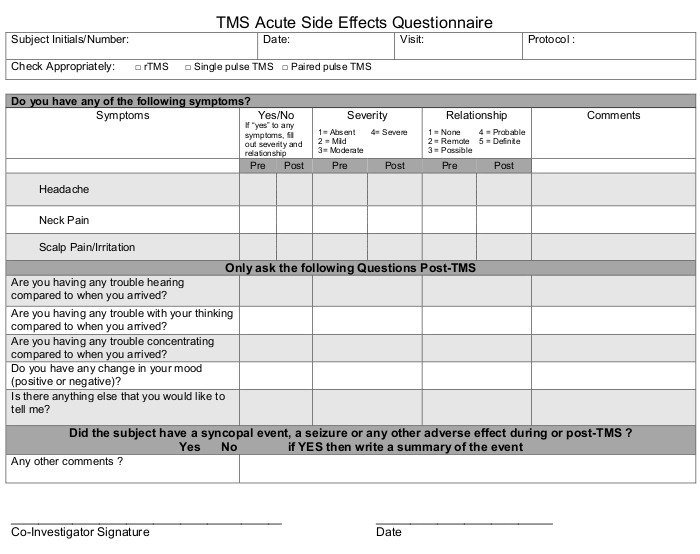
Figure 2: Side Effects. Monitor potential problems before and after TMS. Please click here to view a larger version of this figure.
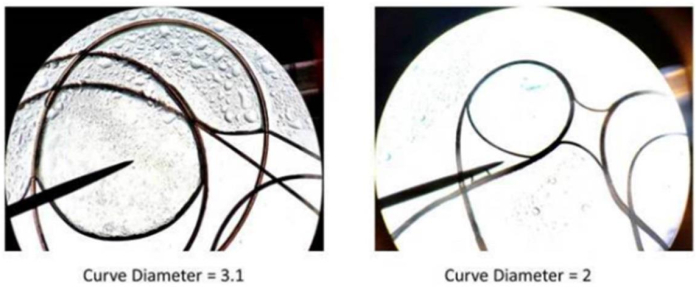
Figure 3: Comparison of differences in curves. The left sample represents a wider curve-longer diameter. This results in less overall hair density. On the right, the 'tighter; curve tends to result in an overall thicker head of hair. Please click here to view a larger version of this figure.
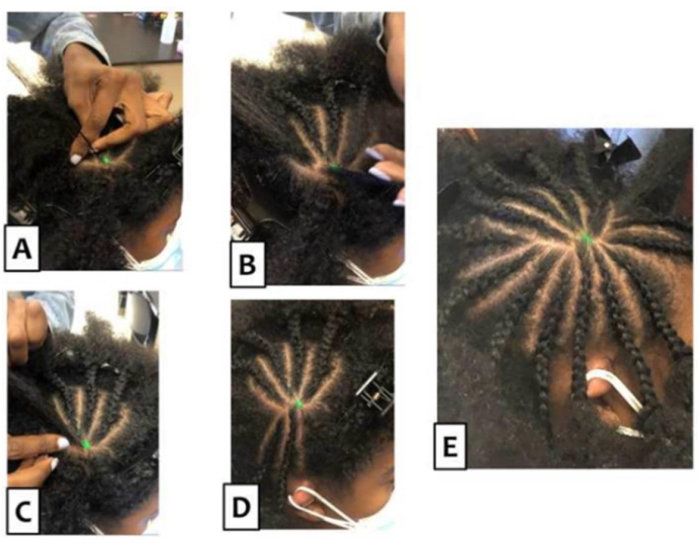
Figure 4: The Sol method. (A) Manageable strands are pulled away from the target point. (B–D) Progressive cornrowing is presented so that a clear pattern emerges. To achieve better motor evoked potentials and (E) a vacated target, it is vital to braid so that the hair is flat on the scalp (this is a cornrow). Starting from the mark point on any side of the hair, separate a clump of hair. Using that section, part the hair 'clump' three more times vertically and begin to cornrow. To cornrow, place the left hair section in the left hand and the right section in the right hand. Let the middle section lay flat on the scalp but using the index finger(s) of one or both hands, press down on the middle section. grab the piece of hair on the right section and go over the middle section, and place it in between the middle and left sections. Then, do the same with the left section and go over the middle section. Continue grabbing sections of the hair one at a time, going over the middle section. While doing so, also add pieces of hair next to the parted section going down the scalp. Continue to do so until the section of the hair is done, ensuring the hair will be adhered to the scalp. Continue the same method of parting the section of hair and cornrowing, going around the marked point of hair until a "Sun" is created. Please click here to view a larger version of this figure.
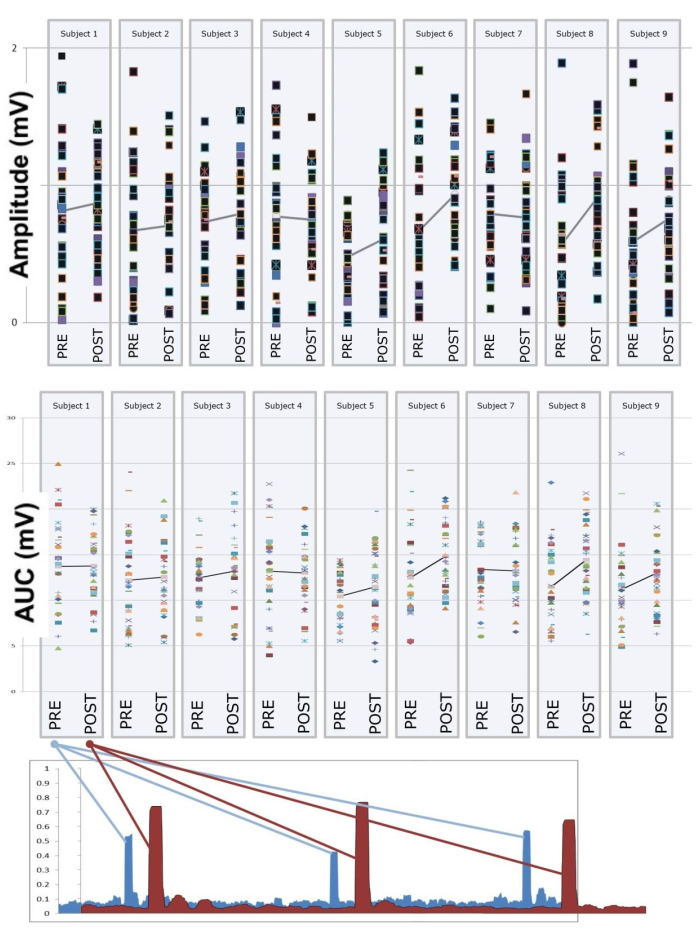
Figure 5: Amplitude, area under the curve, and three sample pre/post motor evoked potentials. The data for all nine participants are presented before and after braiding with the Sol method. Presented are the 30 TMS pulses delivered to M1. The line connecting Pre/Post is the mean of each sample. Abbreviation: TMS = transcranial magnetic simulation. Please click here to view a larger version of this figure.
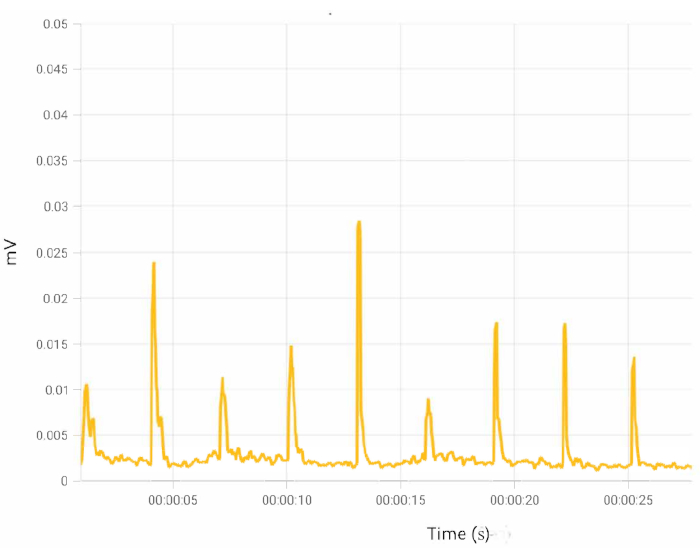
Figure 6: Sample MEPs. Following braiding, MEPs should be consistent and robust. Abbreviation: MEPs = motor evoked potentials. Please click here to view a larger version of this figure.
