General remarks:
All operations should be performed under an upright dissecting microscope (Olympus, SZX10 with Z-Axis Crank Post with STU2 StandBoom Stand) and using a surgical coagulator. Ventilation is critical for the procedure and therefore a certain amount of time should be spent on choosing the ventilator and optimizing the ventilation technique. Temperature, blood pressure and anesthesia should be stable throughout.
1. Anesthesia, Intubation and Monitoring
- Use C57BL/6 mice that are at least 10 weeks old. Induce anesthesia using sodium pentobarbital at a dose 70 mg/kg body weight i.p. Maintain anesthesia with approximately 10 mg/kg/h sodium pentobarbital. Be cautious with overdosing since this might significantly lower the blood pressure. Re-dosing of pentobarbital – even after hrs- can lead to severe increases in plasma levels. Based on strong evidence regarding isoflurane as cardioprotective compound we recommend the use of the ‘inert’ and well established pentobarbital in a model for myocardial ischemia46-56.
- Place mice on a temperature-controlled heated table (RT, Effenberg, Munich, Germany) with a rectal thermometer probe attached to thermal feedback controller to maintain body temperature at 37°C.
- After anesthesia induction secure mice in a supine position, with the upper and lower extremities attached to the table using a tape and a suture fastened to the ankles. Do the same for the head by using the teeth. A sufficient restraining is important for a successful intubation and well controlled surgery. Prior to surgery, cover the mouse with mineral oil to reduce the risk of mouse hair allergy.
- Expose the trachea surgically and perform a tracheal intubation using bluntpolyethylene cannulae (Insyte 22g, Beckton Dickinson, USA). You will have to blunt the needle to be able to use it as a stylet.
- Pull the tongue out using a pair of forceps and then push gently in a 15-degree angle towards the body. Even after exposure of the trachea and using a microscope, this might require some training. Be aware that a small damage of the trachea might lead to the inability to ventilate the animal throughout the suture. Thus, if you encounter airway problems check the trachea for small holes.
- Confirm correct tube placement by direct visualization of the cannula within the previously exposed trachea above the carina.
- Connect the tube to a ventilator. We recommend a pressure controlled ventilation technique by using a Servo 900 C from Siemens (DRE Veterinary, USA). Animals will then be ventilated using peak inspiratory pressure of 10 mbar, frequency of 110 breaths/min and a positive end-expiratory pressure of 3-5 mbar with a FiO2 = 0.4. Settings might need some adjustments that can be achieved most easily by checking the lungs during open thorax surgery. Make sure that the lungs are not collapsed or overextended. Despite of the fact that the Servo 900 C is built as ventilator for humans, its use in a pressure controlled ventilator setting works excellent for the ventilation of mice.
- Perform Blood gas analysis to confirm normal gas exchange (partial pressure of oxygen, paO2 of 115±15 mmHg and partial pressure of carbon dioxide, paCO2 of 38 ±6 mmHg) after 4 to 6 hours of ventilation time using the i-STAT System (Abbott, USA).
- Monitor heart rate with an ECG (e.g. Hewlett Packard, Böblingen, Germany). Make sure that the heart rate does not drop below 450. If the mouse develops bradicardia check the temperature and the anesthetic dose/concentration. Xylacin/ Ketamin anesthesia induces a heart heart of 250/ min and is therefore not recommended.
- Apply a proper fluid replacement. An infusion with normal saline 0.1 ml/hour via an arterial or venous catheter should be performed prior to the onset of ischemia. Also, a saline bolus of 500 μl could be given i.p. prior to surgery. Thoractomy can induce a drop in blood pressure and may require additional saline boli. After ischemia, an infusion rate up to 1 ml/hour might be necessary to maintain a mean arterial blood pressure above 60 mmHg and to guarantee a sufficient reperfusion critical for infarct staining using TTC.
- Place a carotid artery (PE10, Tip O.D. (mm/”), Tapered>.024 mm/.011″) for continuous recording of blood pressure. The carotid artery will be exposed via blunt dissection of the paratracheal muscles. Following further exposure and careful avoidance of any tissue trauma (particular of the vagal nerve), a catheter is inserted into the vessel using two sutures and a small clamp. Attach the arm to the body before you start dissecting the artery. This will expose a longer piece of the artery. Knot the very end of the proximal part of the carotid artery. Attach a larger clamp to the end of the suture to obtain tension. Place another suture around the artery and dissect the artery to the very distal end. Here, place a small clamp. Use micro scissors to cut a small diagonal opening into the artery. Hold the opening with a fine forceps (Dumont, WPI) and advance the proper sized catheter with your hands/forceps. Make a knot with your second suture and secure the artery. Loosen the clamp and advance the catheter further. Secure the catheter with several knots and tape.
2. Technique of Coronary Artery Occlusion
- Dissect the skin and expose the left thorax wall using a blunt dissection technique.
- Cut the muscles pectorals majors and minors to expose the thorax wall with a cautery. By pulling the pectoralis major, the lung drops, thereby a forceps from the electrosurgical unit can be inserted, and, 1-3 mm above the lung, a horizontal line crossing the rips should be coagulated.
- By using a blunted scissor, cut the thorax wall. Modified safety pins, where the catch plate is removed and the blunt end is bent, are then used to keep the thorax open.
- To facilitate the final placement of the suture, coagulate and cut the thorax wall along the diaphragm towards the lower left side of the thorax.
- Expose the heart by dissecting the pericardium. To avoid diaphragmatic movements remove and cut the phrenic nerve.
- Use a small wet cotton stick with a forceps and turn the heart towards the right side. Identify the left coronary artery (LCA) and make sure that the lungs are not too inflated. Optimize the opening of the thorax to have a secure hold of the heart when placing the suture. If the blood pressure is too low the identification might be complicated. Additional boli of saline might improve identification of the LCA. The LCA is a bright red vessel crossing the heart horizontally (in contrast to the returning veins). Sometimes, the LCA is seen best without a microscope. Do not use too much light. This can lead to sever reflections making visualization impossible.
- Once the LCA is visually identified, place an 8.0 nylon suture (Prolene, Ethicon, Notiefies, USA) around the LCA. For the purpose of intermittent LCA occlusion, we adopted a chronic model of cardiomyopathy 42using a hanging weight system.
- Thread the suture through a small piece of plastic tube (PE-10 tubing) with blunt edges and attach two small weights (1g, e.g. use Eppendorf tubes filled with water) to each end. With the weights freely hanging over a rod, the LCA should immediately be occluded. In addition, when the weight is relieved, LCA occlusion is terminated at once. Successful LCA occlusion should be confirmed by an immediate color change of the vessel from light red to dark violet, change of color of the myocardium supplied by the vessel (from bright red to white) and the presence of ST-elevations in the ECG. During reperfusion, the changes of color instantly disappear. Keep the heart wet with a 37°C, saline soaked, piece of absorbent cotton throughout (see also Figure 1).
- Chose your ischemia time according your primary interest. In fact, for studies of cardioprotective effects of IP, it would be ideal to use an ischemia time associated with an in infarct sizes of approximately 30 to 40% of the AAR. Thus, it would be possible to demonstrate changes in both directions, e.g. smaller infarct sizes with cardiac IP or larger infarct sizes with an experimental therapeutic or a specific gene deletion. In addition, mice with an infarct size of less than 50% usually survive the experiment, whereas infarct sizes of 60 to 80% are often not survived and the animals die before the reperfusion time is complete. Using our model 10 minute of myocardial ischemia followed by 2 hours of reperfusion result in an infarct size of 3.5 ±1.3 % of the AAR. In contrast, an ischemia time of 60 minutes results in a mean infarct size of 42±5.2% of the AAR (p<0.01)39. Thus, we consider a 60 minutes of ischemia as ideal to study changes in both directions. Nevertheless, you might have to adjust the ischemia time in gene targeted mice with a sever phenotype.
- Chose the right reperfusion time. The reperfusion time is critically important for TTC staining. The colorless dye is reduced to a brick-red-colored precipitate by dehydrogenases in the presence of the co-enzyme NADH. Dying cells lose their ability to retain NADH and, therefore, are delineated as pale areas within the red stained viable myocardium. Infarct size delineation by TTC requires that NADH has been washed out completely from the necrotic area. However, if reperfusion is not long enough, infarct size delineation by TTC staining may result in an underestimation of the actual infarct size 43. In our hands, after an ischemia time of 60 min, the infarct size measurement increased from 11.5 ± 4.5 % after 30 minutes to 42.2 ± 5.1 % after 120 minutes. No further increase in infarct size could be detected with longer reperfusion times (240 minutes)39. Thus, we recommend a 2 hour reperfusion period which seems also reasonable in the context of cardiac enzyme determination.If you consider ischemia preconditioning, we recommend 4 cycles of IP (5 min ischemia, 5 min reperfusion), followed by an ischemia time of 60 min and a reperfusion time of 2 hours. Under these conditions, IP was associated with a 3.2-fold reduction of infarct size from 42.2 ±5.1 % to 13.3 ±3.3 % of the AAR39. However, due to the hanging weight system, different preconditioning regiments could easily be applied.
3. Determination of the Area At Risk (AAR) and Myocardial Infarct Size
After induction of a myocardial infarct (with or without IP), the area is perfused by the LCA (area at risk, AAR) and the size of the infarct itself will be determined using a staining technique. Subsequently, infarct will then be calculated as percentage of myocardial infarction compared to the AAR. To do this, a previously described double staining technique with Evan’s blue and triphenyltetrazolium chloride (TTC) is used 44.
- Determine the AAR by retrograde injection of 1 % Evan’s blue dye into the aorta while the LCA is occluded. Alternatively, if a carotis catheter is in place, use this route for Evans blue injection. Evans blue will stain all myocardial tissue blue, except the AAR. It is critical for this step to avoid air bubbles within the catheter, as they would be injected into the coronary circulation and prevent Evan’s blue staining. Prior to the Evans blue staining you might want to collect blood for cardiac enzyme measurements. In addition, removal of blood by injecting 5 ml of saline via an aortic or carotis catheter is recommended.
- Excise the heart and wash in ice cold 0.9% saline
- Embed into 2% agarose. Do not use hot agarose since this will prevent successful staining.
- After 30 minutes at +4°C (or 15 minutes -20°C), cut the heart into slices of 1 mm using a heart matrix or microtome. If you place the heart into the freezer avoid dry freezing which will lead to non stained hearts.
- Incubate the slices with 1% TTC at 37°C for 10 min using a 15 ml blue cap in a water bath. This will allow the infarcted area to be demarcated as a white area, while viable tissue stains red.
- Fixate the stained slices with 10% fomaldehyde over night. By doing so, the infarcted area is better contrasted improving quality of pictures.
- Determine the area at risk (AAR) and the infarct size via planimetry using the NIH software Image 1.045.
- Calculate the percent of infarcted myocardium from the area at risk.
4. Cardiac Enzyme Measurement
Due to limitations associated with TTC staining we recommend as additional readout for myocardial infarct severity the determination of cardiac troponin I (cTnI) levels in the serum of mice. The blood will be obtained from the portal vein and serum cTnI levels are then determined with a quantitative rapid cTnI assay(Life Diagnostics, Inc., West Chester, PA, USA).
5. Representative Results:
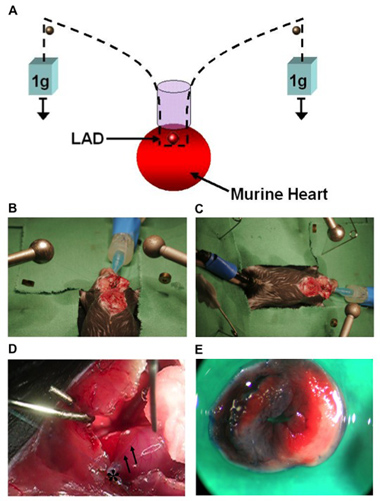
Figure 1. (A) Model of cardiac IP using a hanging-weight system of coronary occlusion. This technique does not require a knot for coronary occlusion. (B, C) Surgical setup. (D) Image of a murine heart with the left coronary artery (LCA, arrows) after occlusion. Visual identification of the LCA is necessary for ligation and ischemic preconditioning in mice. An 8.0 nylon suture is placed around the LCA 1-2 mm beneath the left auricle. The suture is threaded through a small plastic tube (*).The end of each suture is attached to a small weight (1g) and the suture is placed over rods on both sides. (E) Determination of the AAR after LCA occlusion and retrograde injection of Evan’s blue dye into the aorta. The AAR remains unstained while the rest of the myocardium is blue. After incubation of AAR tissue with TTC, the infarcted area stained white, while viable tissue stained red.
