1. Preparation
- Prepare Xylazine-ketamine solution (Ketamine is a controlled substance. Detailed records should be kept and solutions stored in a safe, locked location).
- Clean and sterilize equipment.
- Prepare surgery area by wiping with aseptic agent and then covering with sterile paper toweling, and set up the micromanipulator.
2. Preparation of Cells for Transplant
- Cells should be resuspended to a concentration of 100,000 cells/É l and, although only 250,000 cells are transplanted per mouse, an excess of cells is required for syringe loading purposes (prepare at least 300,000 cells per mouse receiving cells).
- Wash cells to be transplanted 3 times in HBSS in a 50 ml conical vial. Count the cells before the final spin.
- After the final spin down, decant HBSS and leave vial in upside down position to prevent droplets from reaching the pellet.
- Dry inside walls with a UV-irradiated, sterile Kimwipe. Do not allow the pellet to dry.
- Holding the tube upright, slowly and very delicately resuspend the cells in half the final desired volume of HBSS.
- Measure the total volume by pipetting the majority of the suspension into a pipette tip and then adjusting the dial on the pipetter until the entire suspension is in the pipette tip. This will tell you how much more HBSS is needed for the desired concentration.
- Bring volume to the desired amount by adding HBSS.
- Place back on ice. Check viability of cells if they must be on ice for longer than 2 hrs.
3. Preparation of mice for surgery and transplantation
- Anesthetize the mouse by intraperitoneal injection of ketamine (100mg/kg) and xylazine (10mg/kg) in ~100 μl doses or an equivalent anesthetic. The entire procedure from surgical prep to suturing will take 30-40 minutes.
- (Optional: apply numbered, colored tape to the tail of each mouse to ensure identification)
- Shave the dorsal area of the mouse from the lower back to the neck, and extending 2 cm bilateral from the midline, with electric clippers. The hair should be cut as close as possible (it may be necessary to go over the area several times).
- To remove the remaining hair, apply a thin layer of hair removal cream (Nair) with a gauze tipped applicator.
- After 1-2 minutes, wipe Nair off with gauze wetted lightly with soapy water. The prepared area should be clean bare skin without any stray pieces of hair that could get into the wound during the subsequent surgical procedure.
Sterilize the prepared area with iodide solution.
4. Laminectomy
- Frequently change and/or sterilize gloves throughout the procedure. Position the mouse dorsal side up with head pointing to the left (if you are right handed). Drape animal to ensure sterility and that only the shaved area is exposed. Make a vertical incision (˜1.3cm) over the laminecomy site spanning from about thoracic vertebrae T8 to T12.
- With the graefe forceps held in the left hand, firmly secure the spinal column at T9 (Figure 1A) and lift the mouse up to exaggerate the spinal curvature.
- Use the scalpel to score the junction between T10 and T11, the space between the two spiny protrusions. Further expose the junction by carefully scrapping the muscle layer away to expose the bone (see Figure 1B,C).
- Use the scissors to further clear muscle away from the lamina and around the pedicle with small snips. This will open up a small space between the vertebrae. Slowly and delicately insert one blade of the scissors into this gap and snip the pedicle. Make sure the curvature of the scissors is always positioned laterally, away from the cord. Repeat on the other side. (see Figure 1D,E)
- Lift the lamina to expose the cord and carefully snip it off. Be sure not to leave any free or jagged bone fragments behind. (see Figure 1F)
- Prior to injection, clean any blood away with sterile cotton swabs.
5. Injection of cells
- Attach the needle with needle nut to the Hamilton syringe and clean them by flushing several times with water, then 70% ethanol, and finally HBSS. Insert plunger after each fill with water, 70% ethanol, or HBSS.
- Prepare the Hamilton syringe for cell loading by removing the plunger and loosening the needle nut and pulling the needle away from the syringe to prevent backpressure. Ensure that careful handling of the needle and nut are done with sterile gloves.
- Load 15μl of cells into pipette tip and press the tip tightly into the back end of the syringe to load the cells into the syringe.
- Insert the plunger about 5mm and then tighten the needle nut.
- Depress plunger until some of the cell suspension is seen exiting the needle.
- Make sure there are no bubbles in the syringe and lay the syringe down in the horizontal position to prevent the cells from making a gradient by gravity.
- Grab hold of the laminectomized mouse by the spinalis dorsi muscle connecting the spines of T8 and T9 (Figure 2B, C).
- Clamp the hemostat to the left (vertical) micromanipulator arm so that the mouse’s front paws are in the air and its rear paws lightly touching a platform of sterile paper towels as in Figures 2A and 2B.
- Attach the syringe to the right micromanipulator arm (at a 70° angle) and slide the syringe to the lowest position possible before clamping.
- Stabilize the mouse by pinning its tail against the paper towels and slowly lower the syringe (Figure 2B).
- Lower the needle towards the cord and insert the needle 1mm into the opposite hemisphere through the dorsal midline (Figure 2C). The tip of the needle should be in the gray matter close to the central canal.
- Slowly inject 2.5μl of cells. Inject at a rate of 1μl / 5 seconds. After injecting the cells, wait a 10 seconds and retract the needle a tenth of a turn at a time every 10 seconds until the needle is out of the cord. Pay attention to possible efflux of cell suspension.
- Quickly retract the syringe and detach it from the micromanipulator arm. Lay the syringe down horizontally.
- Release the mouse and transfer to suturing table.
- Repeat steps 5.7-5.14 for each mouse until the syringe is emptied. Sterilize tools (in the sterilizer) and the needle (by wiping with ethanol) between animals. Discard cells and reload if clumping is visible.
- Clean the syringe as in step 5.1 between loads.
6. Sutures and post-op care
- Suture the incision. Suture needle is inserted into the superficial fascia on both sides of the incision. The thread is strung through, pulling superficial fascia together (Figure 3A), thereby covering the exposed spinal cord at the site of removed lamina. Do not suture the cutaneous muscle attached to the skin or the skeletal muscle of the back. Pull the entire thread through, leaving approximately 1/2″. Using the needle holder, three knots are formed and thread is trimmed as close to the knot as possible.
- Close the incision by applying two to three staples (depending on size of incision) to the skin (Figure 3B). Carefully pull skin away from the mouse to avoid stapling the underlying muscle.
- Using a 26G3/8 needle inject 0.5ml Lactated Ringers sub-cutaneously in the lower back away from the incision.
- Place mouse back in its cage. To ensure it is able to breathe comfortably while under anesthesia, the mouse should be placed on its side in the cage, avoiding contact between the surgery site and cage bedding. Cages should be placed on heating pads.
- Mice are monitored after anesthesia wears off to ensure bleeding subsides, sutures remain closed, and that mice return to pre-surgery mobility.
- Treat mice one time with the analgesic buprenorphine (0.05-0.1 mg/kg) following surgery.
- Ensure impaired mice have sufficient access to food and water: water bottles are fitted with extended 3.5 inch spouts and mice that are unable to walk are hand fed water and/or high-calorie dietary supplement (Nutri-Cal, Tomlyn).
7. Representative Results:
Desired results will be identifiable by the lack of efflux of the cell suspension during the injection and by the intact appearance of the spinal cord following the procedure. To this end, it is vital to have bright and direct lighting on the mouse’s spine during the laminectomy and during the injection. Optimal lighting is facilitated by fiber optic lighting (Figure 2A).
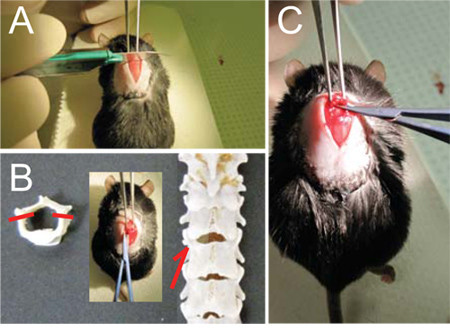
Figure 1- Laminectomy. (A) Once vertebra T9 is solidly held with the Graefe forceps, (B, C) score the spine with scalpel between T10 and T11 to facilitate entry of the micro scissors. (D) Carefully slide the micro scissors through the space between T10 and T11(arrows and inset, E) and cut the pedicles on each side (dashes, E) to free the dorsal lamina. (F) Flip the lamina up rostrally and cut it off.
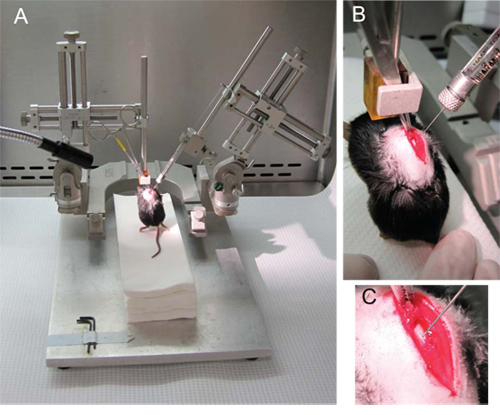
Figure 2. Injection of NSCs. (A) The general setup of the micromanipulator with the hemostat holding the mouse attached to the left arm and the Hamilton syringe on the right arm at a 70 angle. (B) The hemostat hold the spinalis dorsi muscle connecting the spines of T8 and T9. (C) The needle is lowered through the midline and into the gray matter on the opposite hemisphere, proximal to the central canal.
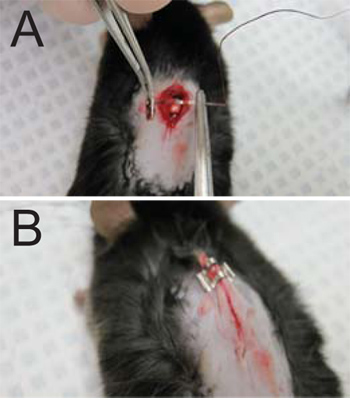
Figure 3. Sutures and wound closure. (A) Sutures are applied to the superficial fascia on both sides of the incision. (B) The incision is closed with 2-3 staples as needed (one staple shown on a wound needing 3).
