tDCS is currently being investigated as a therapeutic instrument for varied neurological conditions, which includes major depression 14, 15, post-traumatic stress disorder 16, craving for food 17, marijuana 18, alcohol 19 and smoking 20, as well as pain 21, tinnitus 22, migraine 23, epilepsy 24, Parkinson’s disease 25, 26, stroke rehabilitation 27, 28 and cognitive dysfunction 6, 29. Table 1 shows the evidence-based tDCS electrode montages to be used as treatment for different clinical conditions.
In most cases, clinical improvement after tDCS is mainly attributed to its cortical effects. There are several ways to quantify cortical changes and the most frequently used ones are functional magnetic resonance imaging (fMRI), TMS-indexed cortical excitability and the electroencephalography (EEG). In comparison with fMRI, EEG has poorer spatial resolution, but superior temporal resolution 30, reflecting timing of neuronal activity more accurately. In addition, as compared with TMS-indexed cortical excitability, EEG provides a greater spatial resolution. For instance, using the tDCS/EEG device, it is possible to detect ongoing changes on the raw EEG in response to tDCS. Figure 9 shows the attenuation of cortical activity, mainly on the parietal region, after the tDCS was turned on (channels C3 and C4). Note that during stimulation it is not possible to record brain activity in the same channels used for stimulation.
The effects of tDCS on EEG have been recently studied by several authors (see Table 3), but only one has applied tDCS and EEG concomitantly 31. Most of the studies showed significant EEG changes upon tDCS by analyzing the EEG power spectrum in response to active versus sham-tDCS. Using power spectrum analysis, EEG signals can be decomposed into a sum of pure frequency components using FFT analysis. In this way, the signals can be analyzed in terms of its power spectrum, which provides information on the signal’s power at each frequency (Table 2).
Figure 7 shows a representative example of an ongoing EEG activity during tDCS (red bracket on the bottom) and after FFT analysis (red circle). The first peak activity corresponds to theta (5-7 Hz) and the second to alpha (8-10 Hz) band frequencies. The amplitude of EEG peaks is measured in μV2.
Another example comes from the study by Maeoka et al. 36, in which the authors found a local decrease in alpha and an increase in beta band amplitudes after anodal stimulation of the dorsolateral prefrontal cortex combined with emotional stress.
Figure 10 shows an illustrative example of the effects of tDCS on quantitative EEG (power spectrum). The size of frontal alpha amplitude was significantly higher in response to active-tDCS when compared to sham-tDCS of the left dorsolateral prefrontal cortex.
Therefore, using the automatic FFT analysis (Figure 7) the investigator is able to determine and measure the amplitude of the predominant EEG frequency activities (delta, theta, alpha, beta, gamma) during and after tDCS. Depending on the region of stimulation and other experimental conditions, the amplitude of specific EEG frequency bands is expected to change after tDCS (Table 3). Indeed, adding the FFT analysis function to the EEG recording during tDCS offers a unique opportunity to understand the cortical neuromodulatory effects in real time.
Finally, EEG signals can be analyzed with a technique called a time-frequency based, or spectrogram image. This technique has been considered promising for research purposes; however, this type of EEG analysis is still not fully validated for diagnostic intentions and should be interpreted with caution for this purpose 8.
Figure 8 shows an illustrative example of an EEG spectrogram processed by the same device.
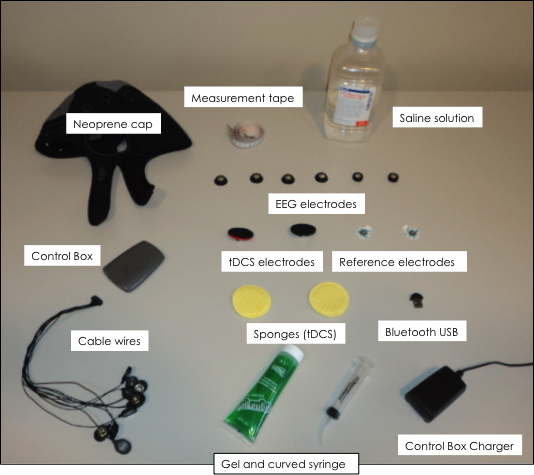
Figure 1. List of required materials for simultaneous EEG monitoring during tDCS: neoprene cap, Control Box, cables, electrodes, measurement tape, saline solution and Bluetooth USB.
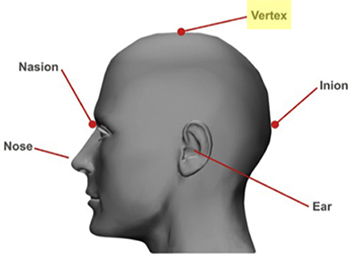
Figure 2. Localization of vertex (Cz) on the scalp 11: Measure the distance of nasion to inion and mark halfway using a skin marker.

Figure 3. Stimulation Screenshot: a) Electrical stimulation mode (tDCS, tACS, tRNS, sham); b) Total duration of electrical stimulation; c) Electrode positioning according to channels; d) tDCS and EEG channel configuration; e) tDCS ramping duration; f) EEG recording durations.
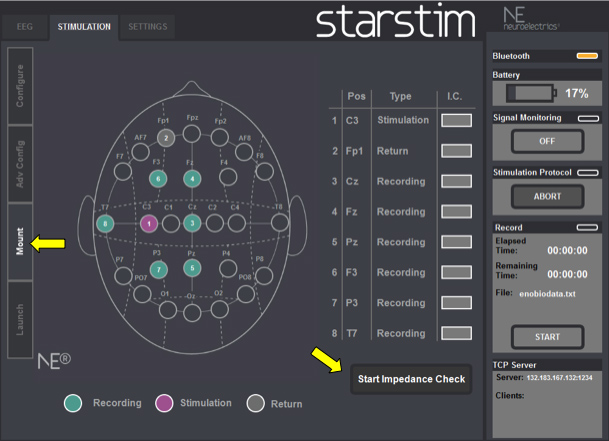
Figure 4. Mount Screenshot: Check electrodes impedance before stimulation begins.
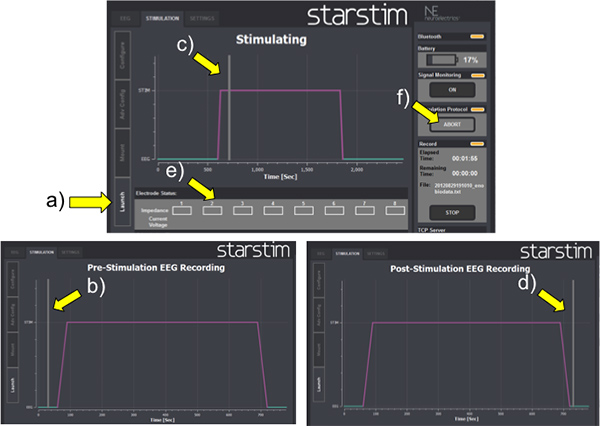
Figure 5. Launch Screenshot: a) LAUNCH button; b) Vertical gray bar before tDCS; c) Vertical gray bar during tDCS; d) Vertical gray bar after tDCS; e) Impedance re-checking; f) ABORT button.

Figure 6. EEG Time domain: check the baseline ongoing EEG activity and select EEG band frequencies if needed (yellow arrow at the right bottom).

Figure 7. EEG power spectrum: check the predominant EEG frequency band (red circle) after automatic Fast Fourier Transform (FFT) analysis over the raw ongoing EEG activity (red rectangle on the bottom).
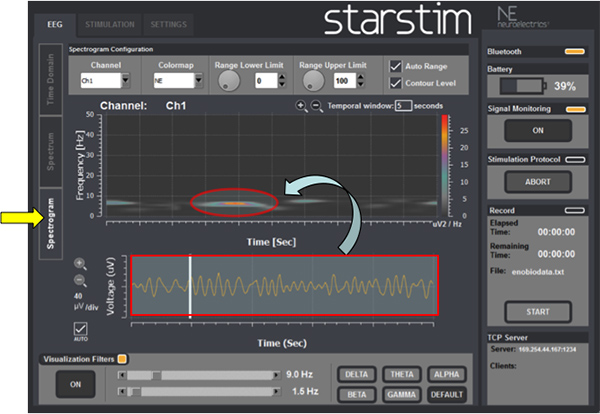
Figure 8. EEG spectrogram: EEG signals (red rectangle on the bottom) can also be transformed into images (red circle) using a technique called time-frequency based.
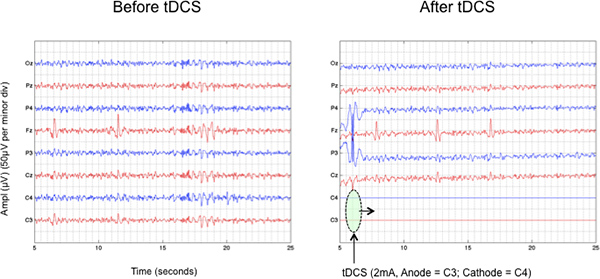
Figure 9. Attenuation of parietal EEG activity in response to anodal tDCS (Anode = C3; Cathode = C4). Note that during stimulation it not possible to record brain activity in the same channels used for stimulation. Click here to view larger figure.
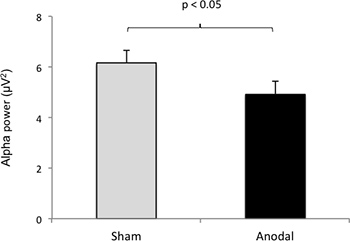
Figure 10. tDCS effects on EEG power spectrum: Note differences in frontal alpha (a) and beta (b) amplitude in response to active-tDCS when compared to sham-tDCS over the left dorsolateral prefrontal cortex.
| Disease | Auteurs | Anode electrode positioning | Cathode electrode positioning |
| Depression | Boggio et al., 2008; Loo et al., 2012 | DLPFC | Supraorbital |
| Pain | Fregni et al., 2006 | M1 | Supraorbital |
| Stroke | Lindenberg et al., 2010 | M1 | M1 |
| Boggio et al., 2007 | M1 (affected side) | Supraorbital | |
| Supraorbital | MI (non-affected side) | ||
| Tinnitus | Fregni et al., 2006 | LTA | Supraorbital |
| Parkinson | Benninger et al., 2010 | M1/DLPFC | Mastoid |
| Fregni et al., 2006 | M1 | Supraorbital | |
| Migraine | Antal et al., 2011 | V1 | Oz |
| Alcohol abuse | Boggio et al., 2008 | R/L – DLPFC | L/R – DLPFC |
Table 1. tDCS electrode montages in different clinical conditions. Legends: LTA, left temporoparietal area; V1, Visual cortex; DLPFC, Dorsolateral prefrontal cortex; M1, Motor cortex, R, Right; L, Left.
| Bands | Symbol | Frequency (Hz) | Best recording site | More prominent during… |
| Delta | δ | 1-4 | Frontal (adults), Posterior (children) | Deep stages of sleep (3 and 4) |
| Theta | θ | 5-7 | Diffuse in the scalp | Drowsiness |
| Alpha | α | 8-12 | Posterior regions | Awakens, with eyes closed |
| Beta | β | 13-30 | Frontal | Mental effort, deep sleep |
| Gamma | γ | 31-45 | Somato-sensory cortex | Short term memory tasks and tactile stimulation |
Table 2. EEG frequency bands.
| Auteurs | Anode electrode positioning | Cathode electrode positioning | EEG Channels (number) | Main Findings |
| Ardolino et al., 2005 | Fp1 | C4 | 4 | Bilateral increase of frontal delta and theta bands. |
| Keeser et al., 2011 | F3 | Fp2 | 25 | Decrease in frontal and prefrontal delta band. |
| Marshall et al., 2011 | F3/F4 | Mastoids | 7 | – Non-REM sleep: frontal decrease of delta band. – REM sleep: global increase of gamma band. |
| Wirth et al., 2011 | F3 | Right shoulder | 52 | Global decrease in delta band. |
| Zaehle et al., 2011 | F3 | Mastoids | 32 | – Anodal: local increase of theta and alpha bands. – Cathodal: local decrease of theta and alpha bands. |
| Jacobson et al., 2011 | Between T4-Fz | Fp1 | 27 | Decrease in right frontal theta band. |
| Polania et al., 2011 | C3 | Fp3 | 62 | – Global synchronization of all studied bands. |
| Maeoka et al., 2012 | F3 | Fp2 | 128 | Local increase in beta and decreased alpha bands. |
Table 3. Studies analyzing the effects of tDCS on EEG recordings.
