Design specifications
Stabilization of the rat femur with the external fixation system enables the creation of osteotomies from 0.5 to 5 mm. The external fixator system is a locked external fixator made of polyether ether ketone (PEEK – [the main body]) and titanium-aluminium-niobium alloy (TAN – [the mounting pins]), which offers a simple, reproducible and adjustable design, and is available in four different stiffnesses: 10, 40, 70 and 100% (100% being the standard, most rigid fixator (Figure 7) . Depending on each investigator’s study requirements, whether they will have to do implant stiffness adjustment in vivo as the bone healing progresses, the external fixator plate comes either as one solid piece (Figure 8) or with two connection elements (Figure 9A) and two main modules (Figure 9B) secured with two interlocking screws (Figure 9C) that have to be assembled prior to surgery (Figure 10A-F). The connection elements are of different thickness, and hence stiffness, and were developed to achieve fixation stiffness equivalent to 10% (0.75 mm thick), 40% (1.70 mm thick), 70% (2.10 mm thick) and 100% (2.50 mm thick; Figure 7). The external fixator stiffness of 100% was calculated based upon the 200 g approximate body weight of a mature rat, and then multiplied by a factor of 4, to a mass equal of 800 g. This was done to make sure that after creating a 5 mm defect, the fixator is capable of withstanding the weight bearing of the animal, thereby maintaining alignment and preventing the dislocation of defect fragments. The remaining three fixator stiffnesses were decreased by 30% respectively from the highest (100%) to have a variety of stiffnesses for studies with various purposes.
Each main module has two holes where the Mounting Pins are inserted. The fixator stiffness can be changed while it is still attached to the living animal by changing the connection elements secured with special interlocking screws (Figure 9C) using 0.5 mm square wrench box (Figure 9H) attached to the hand drill (Figure 9K). TAN (Titanium alloy) was used to make for mounting pins (Figure 9D) to secure the stability bar to the femur (Figure 7). The fixator comes in four pieces and needs to be assembled prior to use if a stiffness change is intended for the study (Figure 10A-F), if not, a single solid pieced fixator should be used. The distance between the outer screws is 16 mm and the distance between the middle screws is 11 mm. All holes are predrilled using a 0.79 mm drill bit (Figure 9E). The screws are locked in corresponding holes in the main fixator frame, which is parallel to the bone surface and set at a distance of 6 mm from the bone (Figure 7).
A saw guide was developed to enable the creation of an accurate, reproducible, 5 mm segmental defect in the femur (Figure 9I); it also serves as a positioning guide for the installation of the external fixator. The main frame of the external fixator is clipped on to the saw guide, and then the whole system is clipped onto the bone as shown in Figure 2B,C. The 5 mm gap is generated with a 0.22 mm Gigli wire saw (Figure 9J). Both the saw guide and the Gigli wire saw can be autoclaved at 134 ºC. If a different sized osteotomy is intended for the study, a custom designed saw guide is available. Due to the miniature size of the external fixator, a special set of implantation instruments was designed and acquired; a customized 0.79 mm drill bit (Figure 9E), 1.00 mm counter sinker for the predrilling of the holes (Figure 9F), 0.7 mm square wrench box for application of the mounting pins attached to the hand drill (Figure 9G), 0.5 mm square wrench box for application of the interlocking screws (Figure 9H), hand drill (Figure 9K). An Accu Pen drill (Figure 9L) was also developed. The core diameter of each mounting pin is 0.02 mm bigger than the drill bit to guarantee proper fitting of the mounting pins into the bone. When used together with a self-cutting screw tip, this has been shown to prevent loosening due to bone surface resorption at the bone-screw interface29. The drill bit (Figure 9E) is operated by a miniature electrical Accu Pen drill that produces 2,500 rpm with a power of 500 mW (Figure 9L).
In vivo experiments
Radiological examination confirmed that fixators of all stiffnesses maintained a 1 mm (not shown) or a 5 mm femoral defect during the entire 8 weeks of the experiment (Figure 11). This was especially important for the 5mm critical size defects, where spontaneous healing does not occur. No distortion or infections, including pin infections, were observed and pin loosening was absent if the instructions of the application were followed30. A complication of using the external fixator was seen if the weight of the rat at the time of surgery has exceeded 250 g, and a smaller size plate was used. In some of those instances, the loading on the mounting pins increased to a critical level so that the pin pullouts were occurring on the distal side of the femur anywhere from one week to two weeks after the surgery (Figure 12). In addition to that, if a larger sized animal is used, the muscle tissue surrounding the femur is relatively thick, which creates skin tension in the vicinity of the implant after the skin closes. Due to swelling tension, when the skin starts to heal it creates an itching sensation to the animal making some of the rats bite the fixator. Since the fixator is created from PEEK material, which is basically high density plastic, on rare occasions, some rats were known to chew through it. Again, in order to avoid this, it is very important to select the recommended body weight for animal studies or switch to the larger version of external fixator.
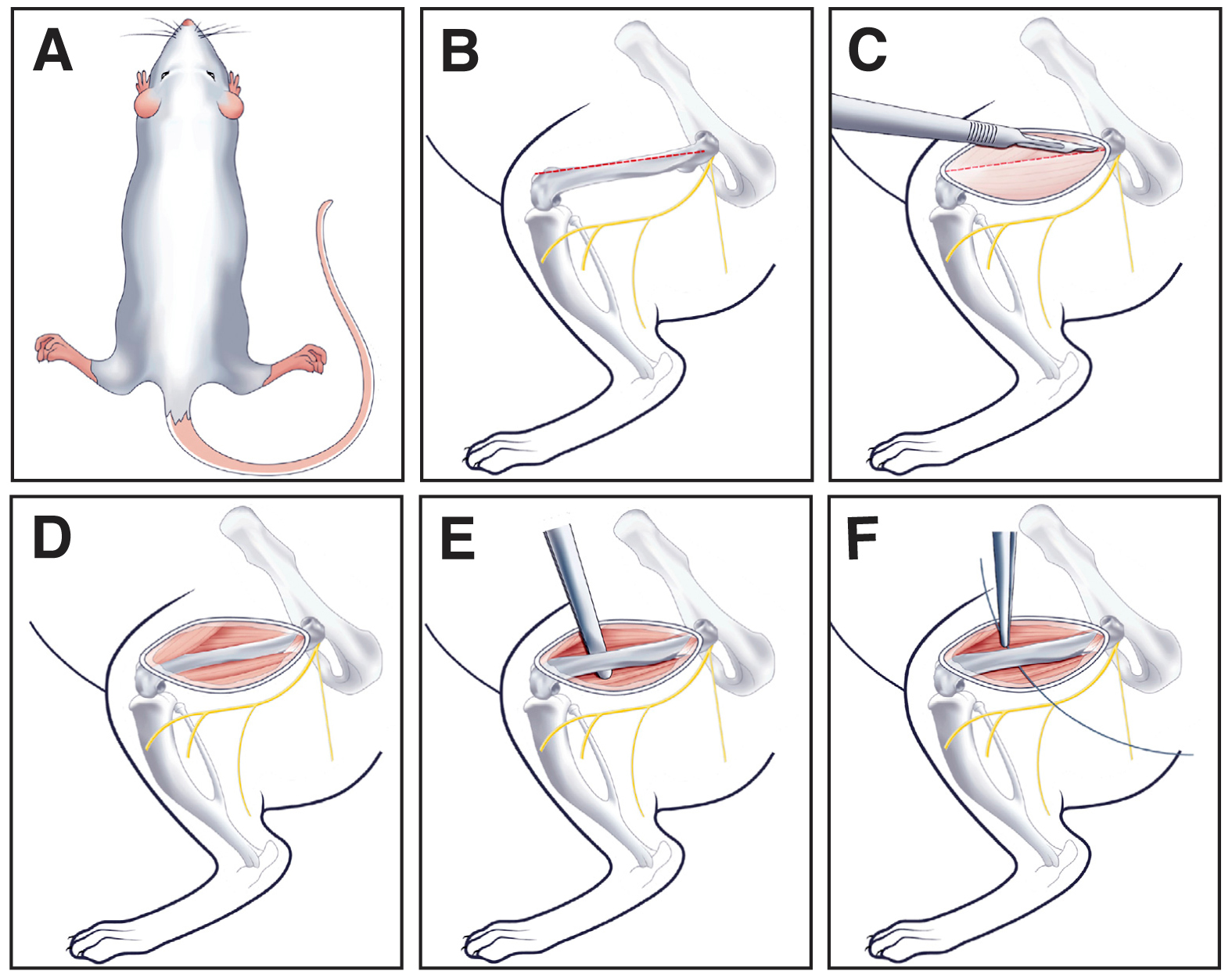
Figure 1. Surgical preparation of the rat femur. (A) Rat positioned in the prone position. (B) Shows the direction of the incision on the femur. (C) Shows incision made in the skin to expose muscle. (D) Shows incision made through the muscle to expose femur. (E) Shows a small clamp positioned under the bone to pass Gigli wire. (F) Shows Gigli wire passed underneath of bone.

Figure 2. (A) Saw guide. (B) External fixator clipped on the Saw guide. (C) Saw guide with the external fixator clipped onto femur.
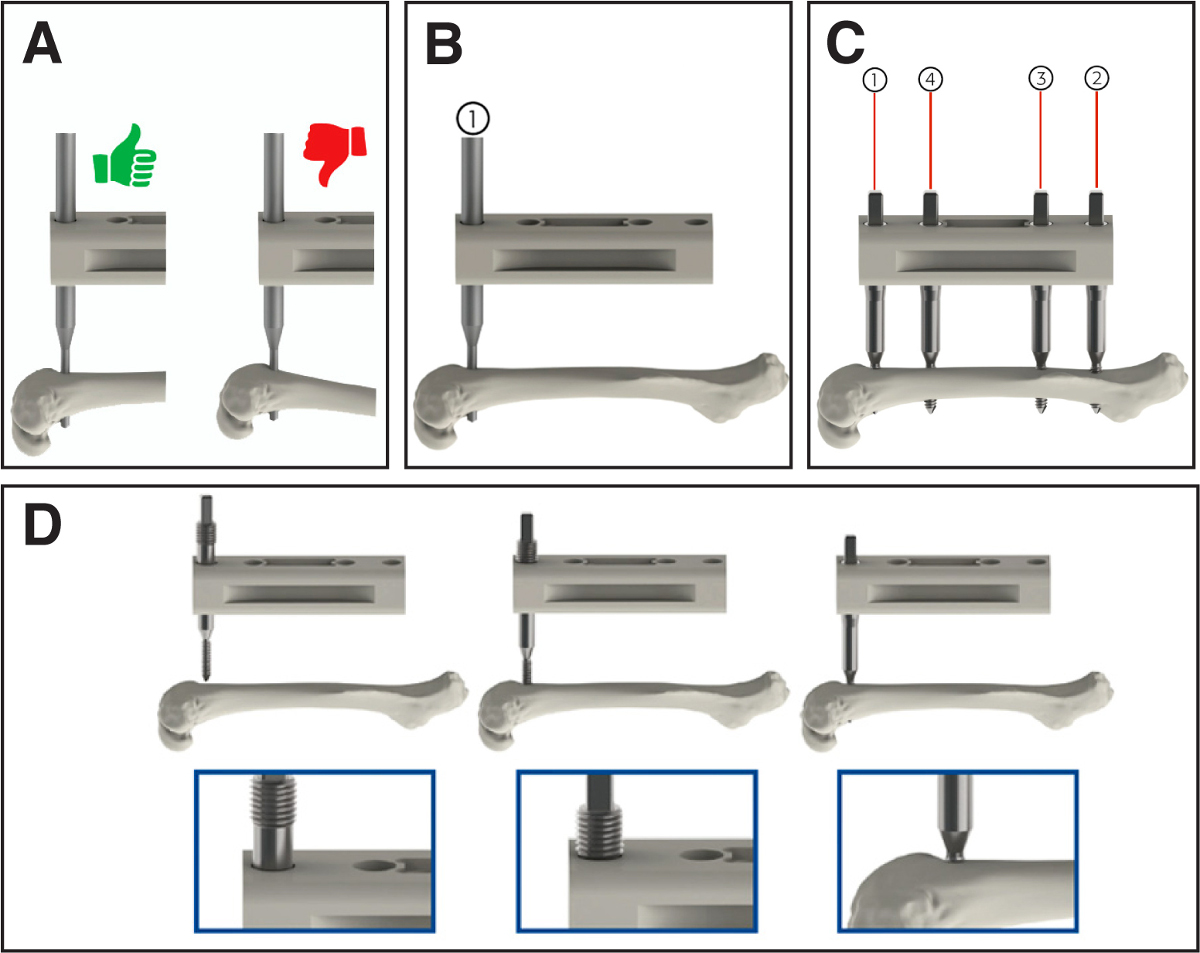
Figure 3. Application of external fixator. (A) Shows correct application of the first mounting pin with the plate reclining antero-laterally and parallel to the bone – green hand, and the incorrect application – red hand. (B) Shows insertion of the first Mounting Pin in the outer distal position. (C) Shows insertion of the remaining Mounting Pins starting with the most proximal position, followed by the two middle mounting pins. (D) Shows insertion of Mounting Pin – more detailed description in the protocol section 4.4.

Figure 4. Surgical implantation of the external fixator on the rat femur. (A) Demonstrates completion of the surgical procedure with external fixator in place with the Gigli wire. (B) Demonstrates created 5 mm segmental defect. (C) Demonstrates sutured muscle layer with exposed external fixator stability bar. (D) Demonstrates sutured skin with exposed external fixator stability bar.
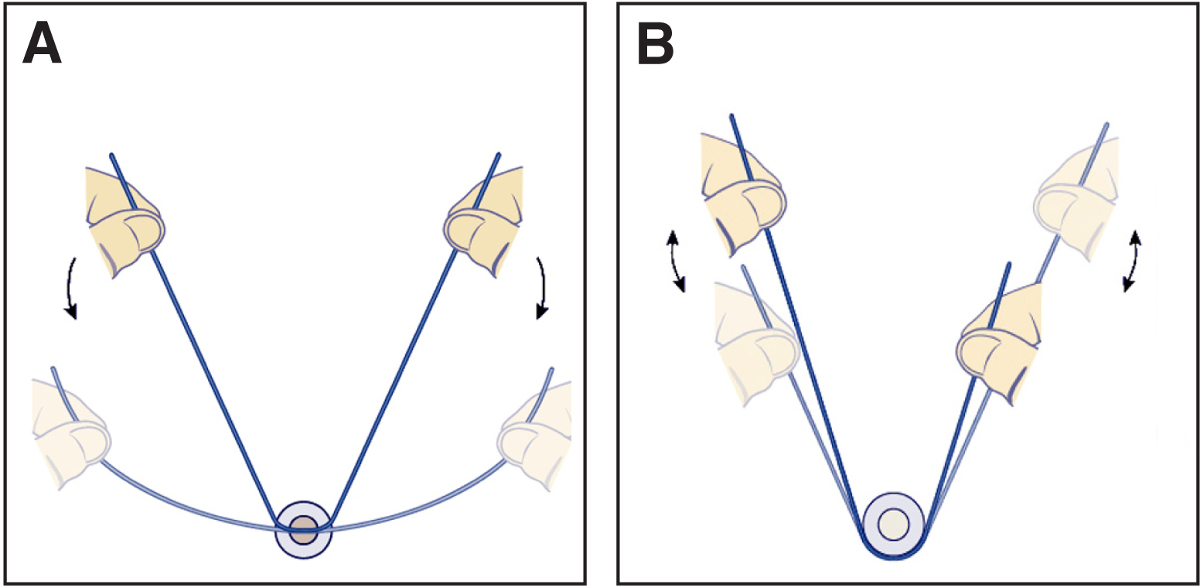
Figure 5. (A) Initial position of Gigli wire for defect creation. (B) An image showing reciprocal motion of Gigli wire.
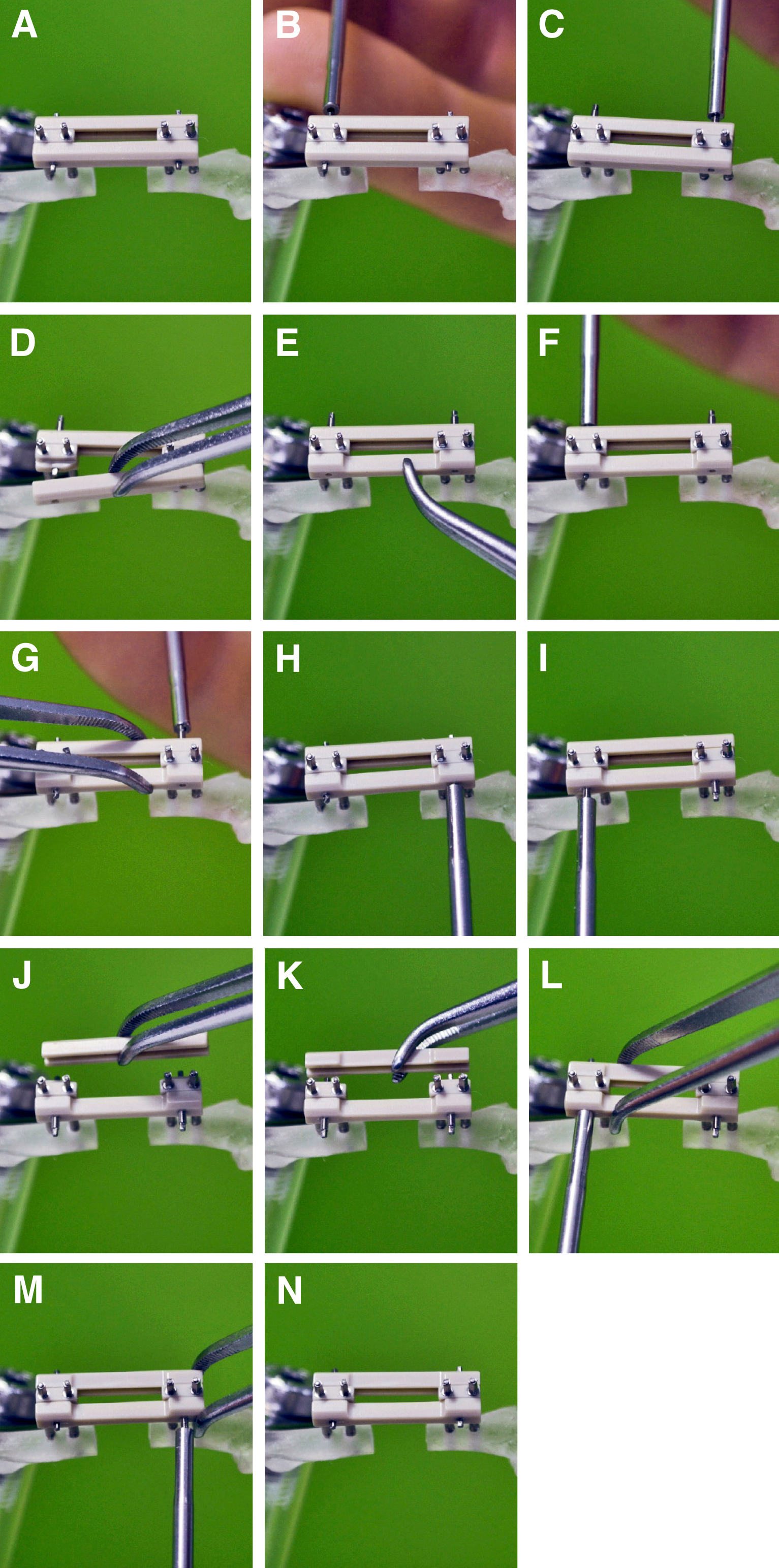
Figure 6. Change of External Fixator stiffness in vivo. (A) External fixator implanted on the femur. (B) Shows removal of the first interlocking screw by carefully turning it counter clockwise until the pin is half way out. (C) Shows removal of the second interlocking screw by carefully turning it counter clockwise until the pin is half way out. (D) Demonstrates removal of the connection element on the opposite side. (E) Demonstrates replacement of desired stiffness connection element in place of the removed one. (F) Demonstrates how to secure the first replaced connection element from the opposite side by turning the square box wrench until the interlocking screw is half way out of the opposite side. (G) Demonstrates how to secure the second replaced connection element from the opposite side by turning the square box wrench until the interlocking screw is half way out of the opposite side. (H, I) Demonstrates switching to the opposite side of the plate to make sure that both interlocking screws are half way out on the side where the connection element was replaced. (J) Demonstrates removal of the second connection element. (K) Demonstrates replacement of the second stiffness connection element in place of the removed one. (L, M) Demonstrates driving of both interlocking screws until the interlocking screw end exits the opposite side of the plate. (N) Demonstrates completed procedure.
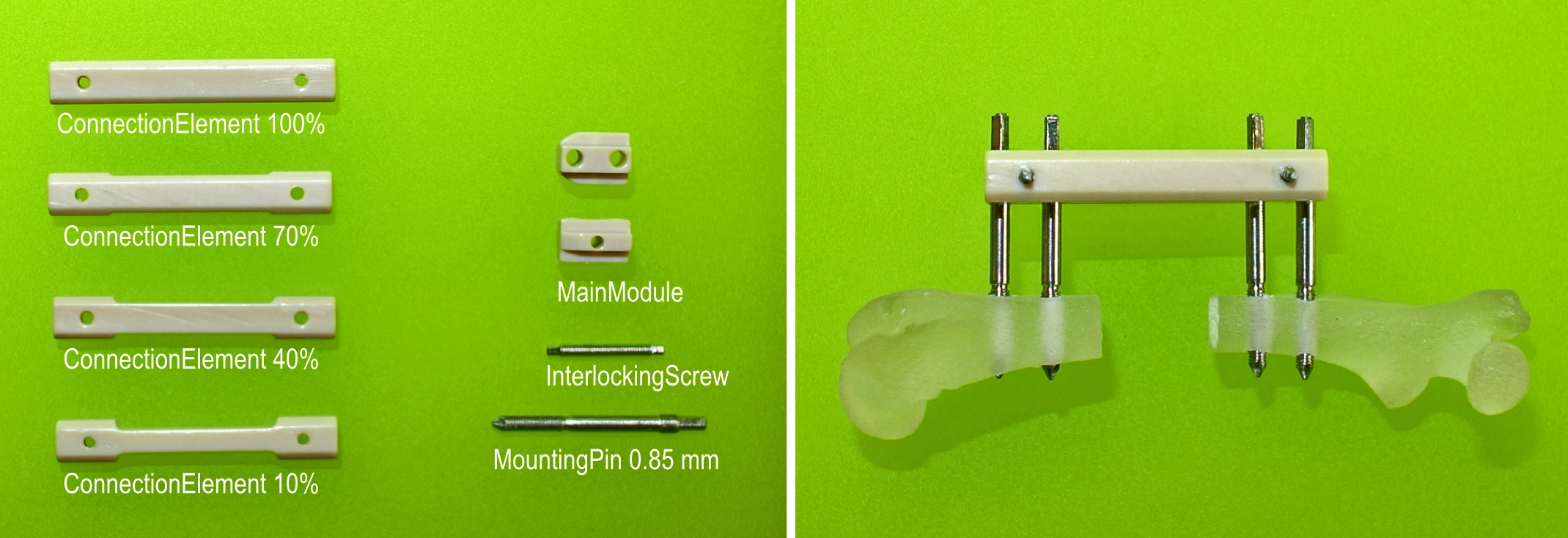
Figure 7. Components of the external fixators. Left: Stiffness is determined by connection elements of different thicknesses. The fixator is attached to the bone with titanium alloy mounting pins. Right: Assembled fixator in place on rat femur with 5 mm segmental defect.

Figure 8. External fixator as a one unit.
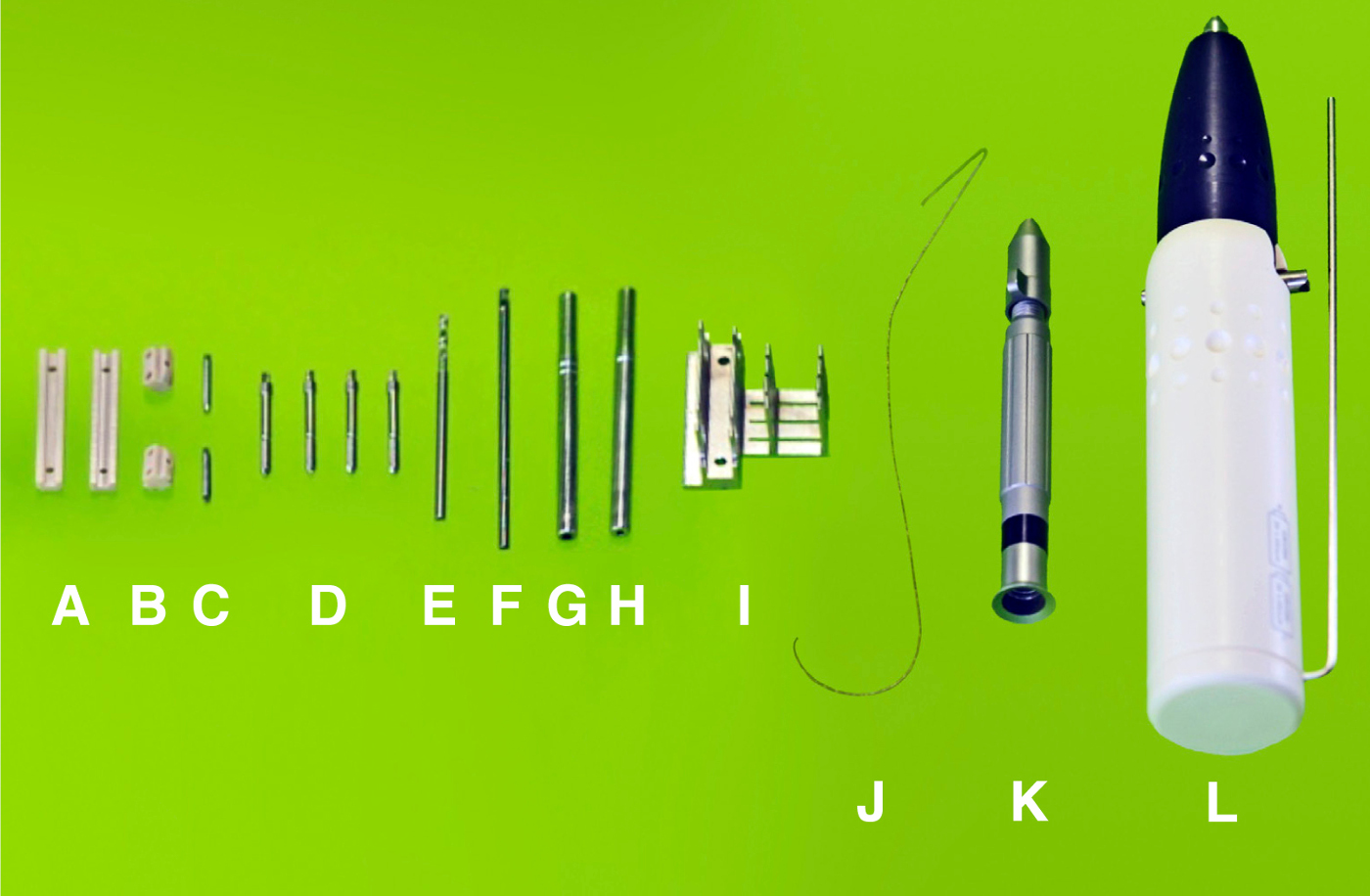
Figure 9. Parts and instruments designed for use with the external fixator. (A) Two connection elements. (B) Two main modules. (C) Two interlocking screws. (D) Four mounting pins. (E) A 0.79 mm drill bit. (F) A 1.00 mm counter sinker for the predrilling of the holes. (G) A 0.7 mm square box wrench for the application of mounting pins. (H) A 0.5 mm square box wrench for the application of interlocking screws. (I) A 5 mm saw guide. (J) A 0.22 mm Gigli wire saw for creation of defect. (K) Hand drill for the attachment of drill bits, 0.70 and 0.50 mm square box wrench. (L) AccuPen 6V+ (Miniature electrical pen drill) used to drive the drill bits.

Figure 10. Assembly of the external fixator. (A) 70% stiffness connection element. (B) The connection element and one of the main modules. (C) demonstrates how one of the main modules slides inside of the connection element. (D) Demonstrates how both of the main modules slide inside of the connection element. (E) Demonstrates both of the main modules and both connection elements in place. (F) demonstrates fully assembled stability bar – main modules and connection elements secured with interlocking screws.

Figure 11. In vivo X-ray images of defects in rats immediately post-surgery and 8 weeks later. External fixators of all 3 stiffnesses were surgically implanted on rat femora and 5 mm segmental defects created. The defects were X-rayed immediately after surgery (t = 0) and at weekly intervals until 8 weeks (t = 8 weeks) when the experiment was terminated. Reproduced with kind permission from eCM journal (http://www.ecmjournal.org). Please click here to view a larger version of this figure.

Figure 12. In vivo X-ray image of the defect in rat 9 days post-surgery with the distal pins pulled out (at the time of the surgery the body weight of the rat was 340 g). Please click here to view a larger version of this figure.
