Block Condition Analyses: Thought Suppression versus Motor Control
ANOVA analyses were used to determine the brain activation associated with block periods of thought suppression (with intrusions removed) relative to a motor control. Contrast results for control and at-risk versus MDD, control versus MDD, control versus at-risk, and at-risk versus MDD are detailed in Table 1. There were no between or within group differences in activity associated with suppression of personally relevant thoughts with distractor thoughts. As a result, all further analyses collapsed the personal and distractor thought suppression conditions in each group. Examining group differences between the control and MDD groups revealed greater activation in the dorsolateral prefrontal cortices (DLPFC) (BA 8), dorsal anterior cingulate, medial prefrontal and superior parietal regions for controls during suppression relative to MDD participants (Figure 2A). Comparisons between the at-risk and MDD groups similarly revealed greater activation of the dorsolateral prefrontal cortices as well as greater inferior prefrontal activation in at-risk participants during suppression as compared to MDD participants (Figure 2B). Collapsing the control and at-risk groups, and contrasting this larger group of healthy young women with MDD patients revealed greater activation in many of the same regions as the separate analyses of controls vs. MDD, and at-risk vs. MDD detailed above. Greater activation was identified in the dorsolateral prefrontal (BA 8), inferior frontal, and anterior insula cortices for the control/at-risk group during suppression as compared to the MDD group. In contrast, greater activation of more dorsal aspects of the insula, inferior parietal cortices and the cuneus were elicited during thought suppression in the MDD group relative to the control & at-risk groups. Finally, group contrasts exploring differences between the control and at-risk participants revealed greater activation for controls in the dorsolateral and dorsomedial prefrontal cortices during suppression relative to the at-risk (Figure 2C).
Event-Related Analyses: Thought Re-emergence versus Re-suppression
An ANOVA was used to examine the brain activation associated with transient re-emergence of target thoughts compared to thought re-suppression. The ANOVA analysis compared control and at-risk versus MDD, control versus MDD participants, control versus at-risk participants, and at-risk versus MDD participants. The results of these analyses are detailed in Table 2. Between group contrasts (thought re-emergence – thought re-suppression) revealed significant clusters of activation in the anterior cingulate cortices (ACC) for the control & at-risk group compared to MDD group. These group differences were attributable to greater activation in the ACC for control and at-risk groups compared to MDD group. The group contrast exploring differences between the control and MDD groups identified greater activation for controls in the anterior cingulate / medial prefrontal cortices, inferior and middle frontal cortices and superior temporal cortices (Figure 3A). The group contrast exploring differences between the control and at-risk participants revealed greater activation for controls in the anterior cingulate, inferior frontal and dorsomedial prefrontal cortices (Figure 3B). Finally, comparisons between the at-risk and MDD groups revealed greater activation of the anterior cingulate, inferior frontal cortices, dorsomedial prefrontal, insula and the uncus in at-risk participants than MDD participants (Figure 3C). These results indicate that the re-emergence and subsequent re-suppression of intrusive thoughts produced a continuum of group activation differences across a consistent set of regions that included the anterior cingulate cortex. Control participants showed the greatest difference in activation between the re-emergence and re-suppression periods followed by at-risk, and then MDD participants displaying the activation changes in these regions (Figure 4).
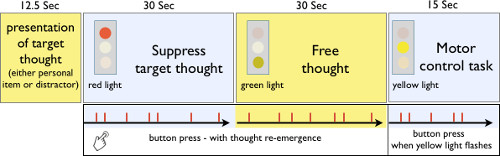
Figure 1: Thought suppression MRI paradigm. Pictorial of the thought suppression paradigm, which included the presentation of the target thought, thought suppression period, free thought period and motor control task. Reprinted with permission30.
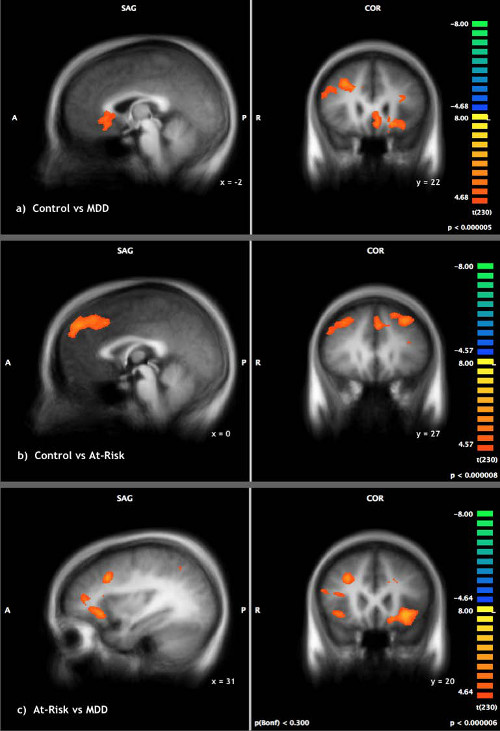
Figure 2: Thought Suppression. Thought suppression compared to motor control in (A) control versus MDD individuals (B) at-risk versus MDD individuals (C) control versus at-risk individuals. Reprinted with permission30. Please click here to view a larger version of this figure.
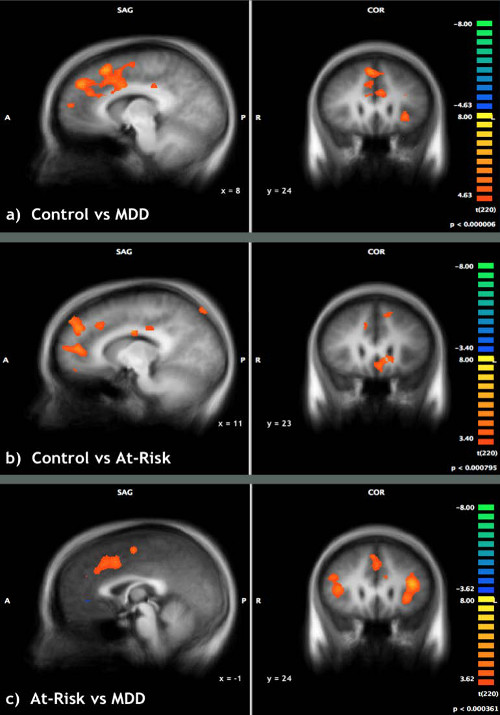
Figure 3: Though re-emergence vs. thought suppression. Re-emergence of target thoughts compared to successful thought suppression in (A) control versus MDD individuals (B) control versus at-risk individuals (C) at-risk versus MDD individuals. Reprinted with permission30.
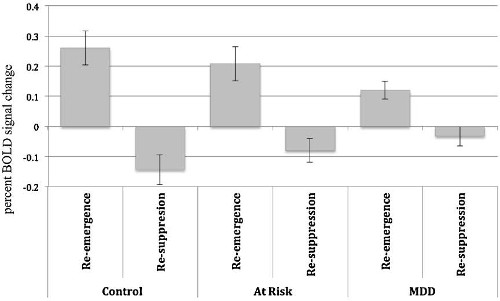
Figure 4: Anterior Cingulate Cortex activity during thought suppression and re-emergence. BOLD signal change in the anterior cingulate cortex for re-emergence and re-suppression of thought conditions. Greatest BOLD differences between the two conditions were elicited by the controls, then at-risk and finally MDD participants. Reprinted with permission30.
| Suppression vs Motor task | |||||||
| Region | BA | x | y | z | t- value | p-value | No. Voxels |
| a) Control & At-Risk vs. MDD | |||||||
| Control & At-Risk > MDD | |||||||
| Inferior Frontal Gyrus | 9 | 53.85 | 17.34 | 22.29 | 7.408 | <0.001 | 473 |
| Inferior Frontal Gyrus | 47 | 42.19 | 25.85 | -3.22 | 9.044 | <0.001 | 4554 |
| Dorsolateral Prefrontal Cortex | 8 | 26.16 | 21.28 | 34.45 | 7.461 | <0.001 | 1011 |
| Cingulate Gyrus | 32 | 11.46 | 23.68 | 29.97 | 7.223 | <0.001 | 783 |
| Superior Frontal Gyrus | 6 | -8.23 | 13.27 | 47.31 | 8.456 | <0.001 | 11795 |
| Precuneus | 7 | -2.48 | -69.17 | 39.1 | 7.417 | <0.001 | 1534 |
| Insula | 13 | -36.11 | 22.58 | 4.08 | 10.770 | <0.001 | 30885 |
| Middle Temporal Gyrus | 21 | -55.72 | -32.24 | -7.34 | 9.660 | <0.001 | 4080 |
| MDD > Control/At-Risk | |||||||
| Cuneus | 18 | -23.73 | -91.4 | -1.15 | -6.653 | <0.001 | 392 |
| Insula | 13 | -40.53 | -11 | 8.2 | -7.457 | <0.001 | 977 |
| Inferior Parietal Lobule | 40 | -51.62 | -31.52 | 23.08 | -8.290 | <0.001 | 1776 |
| b) Control vs. MDD | |||||||
| Control > MDD | |||||||
| Fusiform Gyrus | 37 | 54.57 | -60.2 | -12.05 | 5.753 | <0.001 | 366 |
| Middle Frontal Gyrus | 9 | 47.84 | 20.07 | 28.47 | 5.563 | <0.001 | 624 |
| Fusiform Gyrus | 20 | 38.21 | -24.52 | -26.78 | 5.990 | <0.001 | 461 |
| Superior Parietal Lobule | 7 | 28.48 | -59.26 | 44.5 | 7.155 | <0.001 | 1617 |
| Middle Frontal Gyrus | 6 | 24.66 | -1.78 | 53.11 | 5.688 | <0.001 | 500 |
| Dorsolateral Prefrontal Cortex | 8 | 28.62 | 21.46 | 35.58 | 6.205 | <0.001 | 1112 |
| Ventromedial Frontal Gyrus | 10 | 16.92 | 32.46 | -8.48 | 5.845 | <0.001 | 973 |
| Anterior Cingulate | 32 | 10.72 | 33.08 | 25.96 | 5.731 | <0.001 | 561 |
| Caudate | -15.22 | 23.75 | -6.17 | 7.428 | <0.001 | 6062 | |
| Superior Parietal Lobule | 7 | -25 | -54.08 | 39.14 | 5.915 | <0.001 | 1183 |
| Middle Frontal Gyrus | 46 | -35.33 | 29.34 | 19.61 | 6.629 | <0.001 | 1693 |
| Inferior Temporal Gyrus | 20 | -54.85 | -34.52 | -12.19 | 7.253 | <0.001 | 2062 |
| c) Control vs. At-Risk | |||||||
| Control > At-Risk | |||||||
| Dorsolateral Prefrontal Cortex | 8 | 35.55 | 28.27 | 38.61 | 5.949 | <0.001 | 5053 |
| Precuneus | 7 | 21.29 | -69.02 | 35.03 | 5.312 | <0.001 | 391 |
| Dorsomedial Frontal Gyrus | 8 | -10.18 | 38.86 | 39.05 | 6.524 | <0.001 | 22307 |
| Cuneus | 19 | 4.55 | -87.54 | 39.61 | 5.127 | <0.001 | 1086 |
| Lingual Gyrus | 18 | 2.46 | -89.17 | -18.33 | 5.475 | <0.001 | 1886 |
| Cingulate Gyrus | 31 | -2.7 | -44.13 | 40.29 | 4.933 | <0.001 | 803 |
| Posterior Cingulate | 29 | -3.85 | -44.61 | 7.25 | 4.966 | <0.001 | 641 |
| Middle Frontal Gyrus | 6 | -27.97 | -0.74 | 56.75 | 5.694 | <0.001 | 5025 |
| Fusiform Gyrus | 20 | -44.03 | -4.97 | -24.44 | 4.710 | <0.001 | 324 |
| Dorsolateral Prefrontal Cortex | 9 | -46.06 | 20.83 | 32.63 | 5.336 | <0.001 | 569 |
| Middle Temporal Gyrus | 22 | -54.22 | -47.41 | 1.45 | 5.166 | <0.001 | 1710 |
| d) At-Risk vs. MDD | |||||||
| At- Risk > MDD | |||||||
| Middle Frontal Gyrus | 46 | 45 | 18.86 | 18.56 | 5.393 | <0.001 | 555 |
| Inferior Frontal Gyrus | 47 | 37.93 | 31.63 | -0.06 | 6.854 | <0.001 | 5826 |
| Dorsolateral Prefrontal Cortex | 8 | 28.78 | 18.53 | 34.15 | 6.718 | <0.001 | 889 |
| Inferior Frontal Gyrus | 47 | -27.97 | 24.94 | -5.92 | 8.273 | <0.001 | 8208 |
| Inferior Temporal Gyrus | 20 | -48.48 | -34.62 | -11.66 | 6.695 | <0.001 | 2349 |
| Inferior Frontal Gyrus | 9 | -43.33 | 5.5 | 31.04 | 5.926 | <0.001 | 880 |
| MDD > At-Risk | |||||||
| Precentral Gyrus | 4 | -58.64 | -4.45 | 22.75 | -6.031 | <0.001 | 500 |
| Insula | 13 | -45.77 | -34.9 | 22.43 | -6.123 | <0.001 | 1062 |
Table 1: Thought Suppression. (a) Control & At-Risk: Suppression of personal and neutral statements – Motor condition, MDD: Motor condition – Suppression of personal and neutral statements. (b) Control: Suppression of personal and neutral statements – Motor condition, MDD: Motor condition – Suppression of personal and neutral statements. (c) Control: Suppression of personal and neutral statements – Motor condition, At-Risk: Motor Condition – Suppression of personal and neutral statements. (d) At-Risk: Suppression of personal and neutral statements- Motor Condition, MDD: Motor Condition – Suppression of personal and neutral statements. Reprinted with permission30.
| Re-emergence vs Re-suppresion | |||||||
| Region | BA | x | y | z | t- value | p-value | No. Voxels |
| a) Control & At-Risk vs. MDD | |||||||
| Control & At-Risk > MDD | |||||||
| Superior Temporal Gyrus | 13 | 47.55 | -48.85 | 15.16 | 6.935 | <0.001 | 18665 |
| Inferior Temporal Gyrus | 20 | 50.5 | -11.15 | -34.26 | 6.002 | <0.001 | 804 |
| Fusiform Gyrus | 37 | 38.04 | -46.75 | -17.86 | 5.106 | <0.001 | 531 |
| Anterior Cingulate | 32 | 3.15 | 14.93 | 41.26 | 6.755 | <0.001 | 20349 |
| Cingulate Gyrus | 23 | 7.05 | -18.18 | 25.01 | 6.334 | <0.001 | 568 |
| Insula | 13 | -39.51 | 16.12 | 11.4 | 7.167 | <0.001 | 24746 |
| Supramarginal Gyrus | 40 | -46.36 | -43.59 | 31.1 | 7.248 | <0.001 | 14751 |
| b) Control vs. MDD | |||||||
| Control > MDD | |||||||
| Superior Temporal Gyrus | 22 | 50.2 | -48.65 | 10.5 | 6.480 | <0.001 | 8042 |
| Inferior Frontal Gyrus | 9 | 45.18 | 8.16 | 23.21 | 6.390 | <0.001 | 5739 |
| Insula | 36.95 | -0.51 | -2.36 | 6.222 | <0.001 | 2542 | |
| Dorsomedial Frontal Gyrus/ Anterior Cingulate | 32 | 4.8 | 22.94 | 39.24 | 6.758 | <0.001 | 10780 |
| Cingulate Gyrus | 23 | 7.67 | -14.61 | 26.13 | 7.135 | <0.001 | 406 |
| Anterior Cingulate | 24 | -6.41 | 22.89 | 25.5 | 5.876 | <0.001 | 670 |
| Cingulate Gyrus | 24 | -10 | 2.38 | 35.19 | 5.888 | <0.001 | 380 |
| Middle Frontal Gyrus | 10 | -32.54 | 34.35 | 21.99 | 5.870 | <0.001 | 2918 |
| Insula | 13 | -39.56 | 4.6 | 2.22 | 6.740 | <0.001 | 8142 |
| Inferior Parietal Lobule | 40 | -41.12 | -30.05 | 35.15 | 6.189 | <0.001 | 936 |
| Middle Temporal Gyrus | 21 | -48.87 | -32.53 | -5.01 | 5.960 | <0.001 | 591 |
| Superior Temporal Gyrus | 39 | -53.69 | -53.65 | 23.97 | 5.547 | <0.001 | 1144 |
| c) Control vs. At-Risk | |||||||
| Control > At-Risk | |||||||
| Insula | 13 | 38.49 | -10.73 | -2.5 | 6.743 | <0.001 | 7591 |
| Inferior Frontal Gyrus | 47 | 24.74 | 33.12 | -3.47 | 5.159 | <0.001 | 1135 |
| Hippocampus | 27.45 | -40.77 | 1.97 | 4.207 | <0.001 | 630 | |
| Dorsomedial Frontal Gyrus | 9 | 0.45 | 46.97 | 29.98 | 6.248 | <0.001 | 13057 |
| Cingulate Gyrus | 31 | 10.4 | -25.45 | 34.63 | 4.061 | <0.001 | 439 |
| Anterior Cingulate | 32 | -2.93 | 38.46 | -6.89 | 5.453 | <0.001 | 4329 |
| Cuneus | 18 | 3.55 | -94.91 | 24.44 | 4.708 | <0.001 | 339 |
| Cingulate Gyrus | 31 | -10.53 | -36.01 | 34.5 | 4.541 | <0.001 | 453 |
| Caudate | -17.99 | -31.31 | 16.85 | 4.488 | <0.001 | 489 | |
| Superior Temporal Gyrus | -47.13 | -24.52 | 3.47 | 5.639 | <0.001 | 8162 | |
| d) At-Risk vs. MDD | |||||||
| At-Risk > MDD | |||||||
| Superior Temporal Gyrus | 39 | 47.02 | -48.19 | 14.17 | 6.649 | <0.001 | 15860 |
| Inferior Frontal Gyrus | 9 | 43.17 | 9.48 | 21 | 6.122 | <0.001 | 16140 |
| Inferior Temporal Gyrus | 20 | 52.27 | -10.57 | -33.72 | 4.815 | <0.001 | 584 |
| Dorsomedial Frontal Gyrus | 32 | 4.87 | 7.97 | 46.92 | 5.688 | <0.001 | 8580 |
| Anterior Cingulate | 32 | -9.46 | 18.24 | 24.38 | 5.869 | <0.001 | 494 |
| Uncus | 36 | -24.63 | -3.52 | -27.89 | 5.165 | <0.001 | 827 |
| Insula | 13 | -40.1 | 15.42 | 16.26 | 7.314 | <0.001 | 21421 |
| Superior Parietal Lobule | 7 | -30.73 | -54.74 | 40 | 6.175 | <0.001 | 3551 |
| Inferior Parietal Lobule | 40 | -46.34 | -36.74 | 33.83 | 6.364 | <0.001 | 4717 |
| Middle Temporal Gyrus | 37 | -52.46 | -54.47 | 1.43 | 5.899 | <0.001 | 1484 |
Table 2: Though re-emergence vs. thought suppression. (a) Control & At-Risk: Re-emergence – Suppression of personal and neutral statements, MDD: Suppression – re-emergence of personal and neutral statements. (b) Control: Re-emergence – Suppression of personal and neutral statements, MDD: Suppression – re-emergence of personal and neutral statements. (c) Control: Re-emergence – Suppression of personal and neutral statements, At-Risk: Suppression – re-emergence of personal and neutral statements. (d) At-Risk: Re-emergence – Suppression of personal and neutral statements, MDD: Suppression – re-emergence of personal and neutral statements. Reprinted with permission30.
