In a typical experimentation BDL was performed in 40 male C57BL/6 wild-type mice weighting about 18-20 gram. This experiment was done to investigate hepatic fibrogenesis in the initiation phase (3 and 7 days), during progression (10, 14, and 20 days), and during long-term (30 and 60 days)16. In this model, persinusoidal fibrosis has already developed on day 10 after the surgery, while periportal fibrosis that permanently increased up to the end of the experiment was fully developed after 20 days. In the mentioned experiment, all animals that received a simple sham-operation survived, and only two of the 40 mice (5%) that received BDL developed a poor general condition and were therefore prematurely sacrificed before the planned end point of the experiment. The activity of sham-operated animals was without exception already normal one day after laparotomy, while most of the animals subjected to BDL showed reduced activity during the first three days. Jaundiced skin had been already apparent in all BDL animals one or two days after setting of the BDL16.
The values of both alanine aminotransferase (ALT) and aspartate transaminase (AST) that represent well-established serum markers of hepatic injury rapidly increased and peaked during day 7 and day 20 after BDL (Table 1). Thereafter, ALT and AST decreased steadily until day 30 and remained stable until 60 days after surgery. In line with the cholestatic injury, serum concentrations of total bilirubin were steadily elevated and reached a plateau after 7 days16. Similar time course of ALT and AST serum activities were also reported for rats that underwent BDL. In a recent study it was demonstrating that serum AST and ALT levels increased up to 5 or 10 fold of normal at the first week after the BDL surgery and decreased after two weeks19.
Typically, the livers of sham-operated animals still look smooth at the end of the experiment, while the livers of animals that received BDL show architectural alterations that are mainly characterized by the formation of edema and fibrotic nodules on the surface of corresponding livers and hydrops of the gall bladder that is filled with large quantities of bile (Figure 7). The characteristic morphological alterations of the liver that are induced by the BDL surgery are also demonstrable in standard histological analysis (Figure 8).
In the same set of experiments, development of liver fibrosis was semi-quantitatively assessed based on liver histology evaluated by a blinded pathologist using a scoring system in which periportal fibrosis was staged from 0-4 and perisinusoidal fibrosis from 0-2, giving a maximum value that was equivalent to cirrhosis of 6. As expected, the mean fibrosis score in the group of sham-operated animals was 0.00 ± 0.00. In contrast, in the group of animals that received BDL, the score increased steadily until day 60 to a value of 4.83 ± 0.17. The maximum of 3 for periportal fibrosis was reached at day 20. In all animals analyzed, perisinusoidal fibrosis was absent during the first 10 days of the experiment and was firstly noticeable after two weeks. Thereafter, it increased steadily up to the end of the experiment to values of 1.8 ± 0.17 (Table 1).
Also in several other independent animal experiments that were performed, it was observed that the formation of fibrosis was highly reproducible showing time-dependent increase of intrahepatic collagen expression and deposition as a consequence of ongoing fibrogenesis (Figure 9). Similarly, the process of ongoing fibrogenesis is noticeable in elevated expression of α-smooth muscle actin (α-SMA) that represents a marker of fibroblastic cells, i.e. activated hepatic stellate cells and portal myofibroblasts, and hepatic hydroxyproline, an amino acid abundantly found in collagen matrices18 (Figure 9). In addition, the expression of vimentin that indicates increasing amounts of myofibroblasts or fibroblasts is increased after setting of the BDL surgery20. The concomitance of inflammation in injured livers are further reflected by increased expression of Lipocalin 2 (LCN2) that is strongly induced during acute and chronic liver injury and evolves hepato-protective effects during acute liver injury21,22.
Inflammatory cells that infiltrate the livers of animals that received BDL can be detected by specific staining with an antibody that is specific for CD45 (Figure 10). This cellular surface marker that is also known as PTPRC (protein tyrosine phosphatase, receptor type) is specifically expressed in all differentiated hematopoietic cells except erythrocytes and plasma cells.
| Time after bile duct ligation (days) | Total bilirubin | AST (U/L) | ALT (U/L) | Portal fibrosis | Perisinusoidal fibrosis | Total score |
| (mg/dL) | ||||||
| 0 (n = 3) | 0.17 ± 0.06 | 192.67 ± 30.50 | 50.33 ± 6.03 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| 3 (n = 5) | 6.85 ± 2.21 | 1159.25 ± 319.27 | 566.50 ± 335.25 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| 7 (n = 5) | 14.38 ± 2.14± | 976.60 ± 477.16 | 448.20 ± 259.47 | 0.60 ± 0.25 | 0.0 ± 0.0 | 0.60 ± 0.25 |
| 10 (n = 5) | 15.92 ± 2.60 | 1916.60 ± 868.25 | 560.40 ± 80.88 | 1.40 ± 0.25 | 0.25 ± 0.25 | 1.67 ± 0.25 |
| 14 (n = 5) | 17.90 ± 3.84 | 1088.60 ± 276.32 | 505.00 ± 96.15± | 2.4 ± 0.25 | 1.0 ± 0.0 | 3.40 ± 0.24 |
| 20 (n = 4) | 18.00 ± 2.12 | 1072.67 ± 364.27 | 404.00 ± 195.48 | 3.0 ± 0.0 | 1.0 ± 0.0 | 4.0 ± 0.0 |
| 30 (n = 5) | 16.04 ± 4.79 | 446.40 ± 169.75 | 260.20 ± 126.97 | 2.8 ± 0.2 | 1.4 ± 0.25 | 4.20 ± 0.20 |
| 60 (n = 6) | 16.02 ± 1.19 | 484.67 ± 117.79 | 257.17 ± 50.97 | 3.0 ± 0.0 | 1.8 ± 0.17 | 4.83 ± 0.17 |
Abbreviations used are: ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Table 1: Fibrosis scoring in a representative experiment. The data of this table was reproduced from a study in which liver fibrosis was induced by bile duct ligation in C57BL/6 mice16. In this study, the mortality rate after the BDL surgery was 5% (2 of 40 animals were prematurely sacrificed because poor animal conditions developed).

Figure 1: Experimental setup for performing a bile duct ligation. The animal is kept on a warming plate at a temperature of 37 oC and the operational area is covered overall with fluid-impermeable, self-adhesive drapes. During the complete surgery, the animal is permanently connected to an anesthesia system. All instrumentations and solutions (analgesics, anesthetics, antiseptic solution, 0.9% NaCl) are arranged clearly.
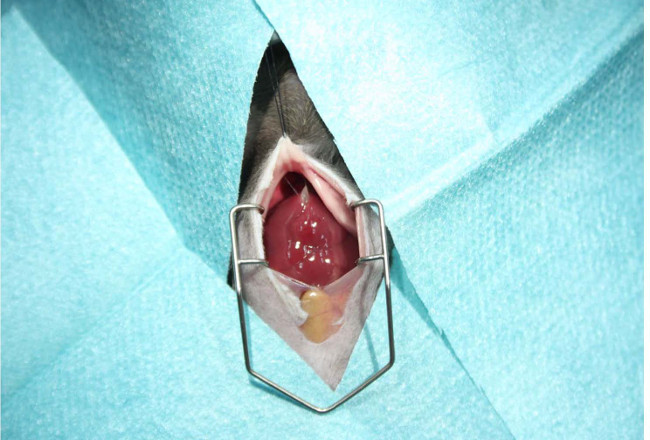
Figure 2: Preparation of the surgery area. Prior opening of the peritoneal cavity, the abdominal skin should be shaved with an electric fur shaver and disinfected with an antiseptic gauze swab. The surgery area is then covered with fluid-impermeable, self-adhesive drapes. The abdomen is opened with a midline laparotomy (~ 2 cm in length). The cavity is enlarged by inserting a holding suture in the sternum and the operation area spread by inserting a Colibri retractor allowing unhindered experimentation during the surgery.
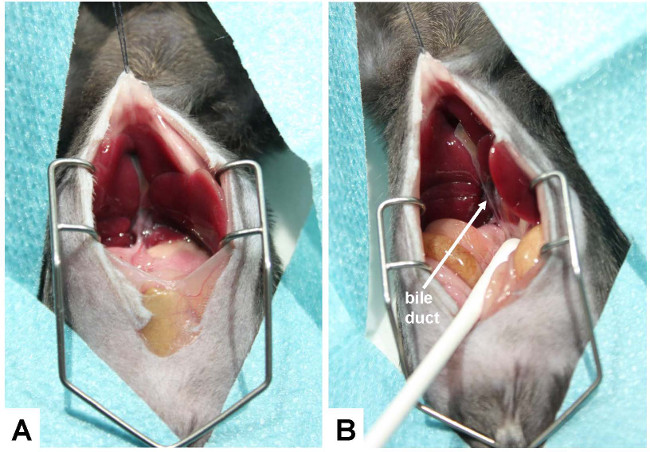
Figure 3: Exposure of the bile duct. (A) For conducting the bile duct ligation, the ventral side of the liver is lifted so that it can stick to the diaphragm and the hepatic hilus becomes clearly visible. (B) To better expose the bile duct, the gut is caudally moved with a humidified cotton swab. The bile duct is marked with an arrow.
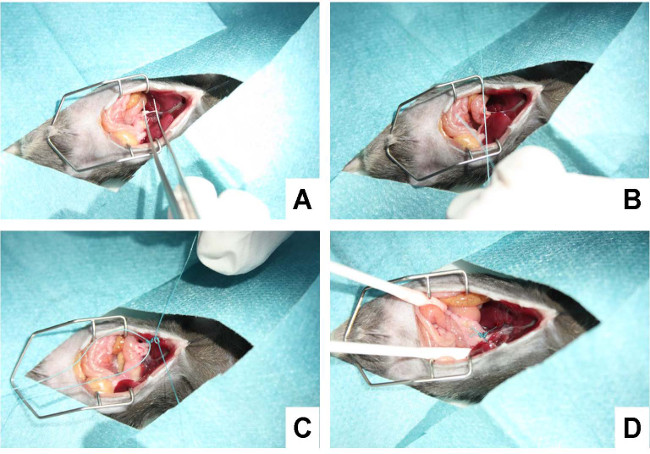
Figure 4: Ligating the bile duct. (A) In a first step, the bile duct is separated carefully from the flanking portal vein and hepatic artery using a micro-serration forceps. (B) Subsequently, a suture is placed around the bile duct and secured with a surgical knot. (C) Thereafter, a second suture is placed in close proximity to the first suture and knotted around the bile duct. (D) The suture is shortened, the cavity rinsed with 0.9% NaCl solution, and all organs replaced to their physiological position.
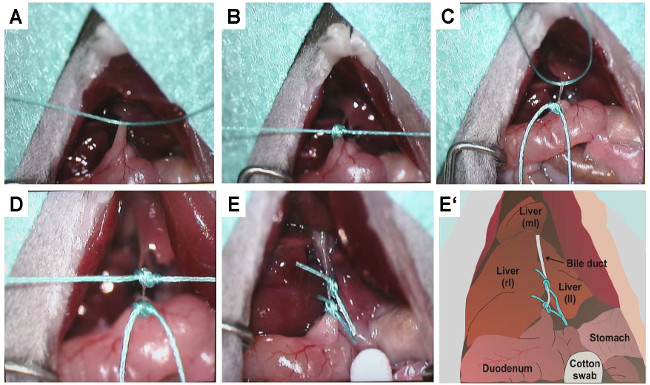
Figure 5: Precise representation of knotting. To document the placement of the sutures and the setting of the two knots that prevent bile flow, the same procedure outlined in Figure 4 was documented under a binocular. (A) Confinement of the bile duct with the first suture. (B) Knotting of the first suture. (C) Confinement of the bile duct with the second suture. (D) Knotting of the second suture. (E) Double-ligated bile duct after shortening of excess sutures. (E') This panel depicts a sketch of (E). The positions of the right (rl), left (ll) and median (ml) lobes of the liver as well as the bile duct, stomach, and duodenum are lettered. In the sketch the bile duct is double ligated by two sutures.
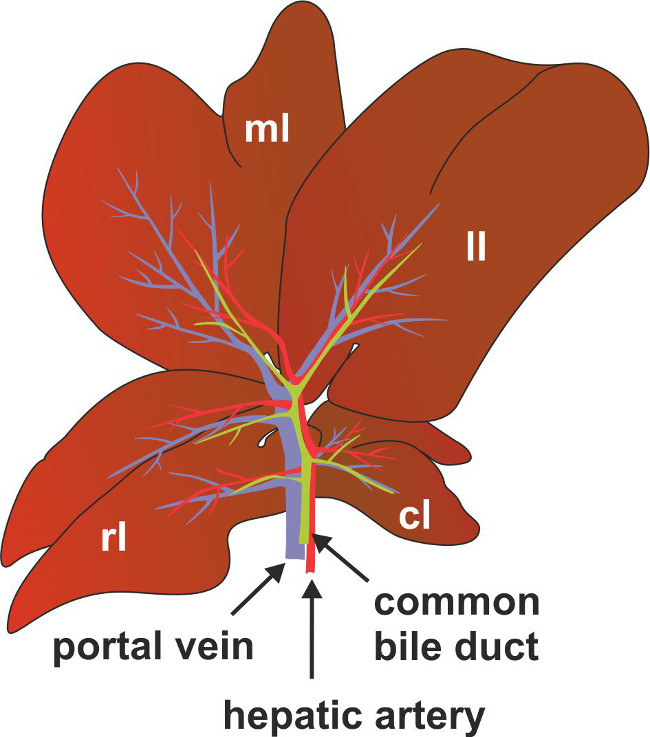
Figure 6: Anatomy of bile duct, portal vein and hepatic artery in mice. For better anatomic location of the common bile duct, portal vein and hepatic artery are depicted as a scheme. Marked are also the positions of the right (rl), left (ll) median (ml) and the caudate (cl) lobes of the liver.

Figure 7: Representative appearance of livers 2 weeks after sham operation and BDL. C57BL/6 mice were subjected to sham operation or BDL surgery. After two weeks the visceral cavity was opened. While the livers of sham-operated animals showed no sign of fibrosis, the livers of animals receiving ligation of the biliary duct had an irregular surface structure with formation of edema and fibrotic nodules on the surface of corresponding livers.
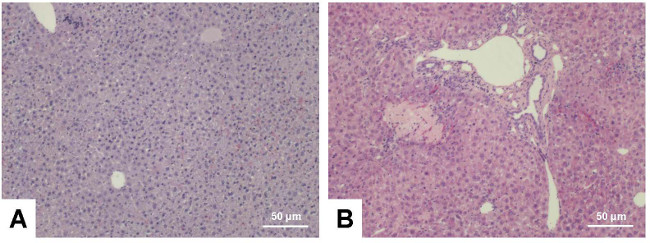
Figure 8: Hematoxylin and eosin stain. Liver sections were prepared from C57BL/6 wild type animals that were sham-operated (A) or received BDL for three weeks (B). The sections were stained with hematoxylin and eosin following standard procedures. Please note the typical alterations within the BDL liver that include signs of inflammation (infiltrating cells), parenchymal (hepatocyte) necrosis, and proliferation of bile ducts. The scale bar in each figure panel represents 50 µm. Please click here to view a larger version of this figure.
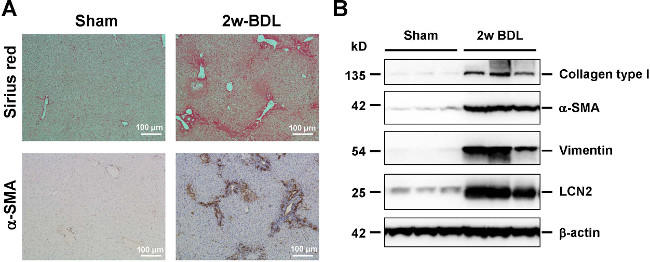
Figure 9: Histological and biochemical readouts for hepatic fibrogenesis. (A) Liver sections were prepared from animals that received sham operation or BDL for 2 weeks and stained with Sirius Red (upper panel, collagen fibers in red) or analyzed for expression of α-smooth muscle actin (α-SMA) (lower panel, α-SMA positive cells in brown) by immunohistochemistry. The scale bar in each figure panel represents 100 µm. (B) Protein extracts from livers were subjected to Western blot and analyzed for expression of collagen type I, α-SMA, and Vimentin that are well established markers of hepatic fibrogenesis. The expression of Lipocalin-2 (LCN2) indicates the inflammatory response that is associated with ongoing fibrogenesis. In this analysis, equal protein loading was demonstrated by probing the blots with an antibody specific for β-actin. Please click here to view a larger version of this figure.
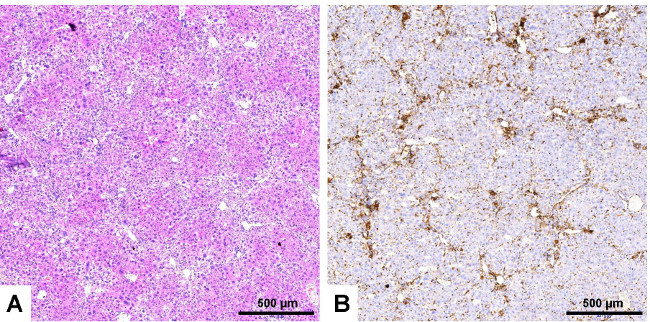
Figure 10: Immunological staining of infiltrating inflammatory cells. Serial liver sections were prepared from a liver of an animal that received bile duct ligation for 3 weeks. The sections were stained with hematoxylin and eosin (A) or with an antibody that is specific for CD45 (B). Please note, the high number of CD45 positive cells surrounding the bile ducts. These massive infiltrates that indicate inflammation are not visible in liver sections derived from sham-operated animals (not shown). The scale bar in each figure panel represents 500 µm. Please click here to view a larger version of this figure.
