This protocol was approved by the University of Minnesota Institutional Animal Care and Use Committee.
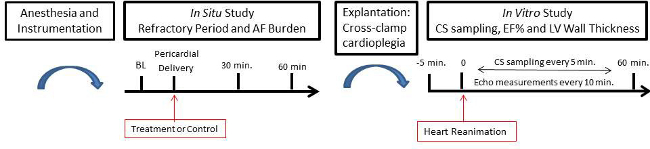
Figure 1. Diagram of Study Paradigm Please click here to view a larger version of this figure.
1. Surgical Preparation of the Swine
- Administer 5-7mg/kg of tiletamine/zilazipam to the swine (70-80 kg) via intramuscular injection. Place an ear vein catheter and administer 5-7 mg/kg methohexital via intravenous access. Intubate the animal with endotracheal tube and ventilate.
- Deliver isoflurane >1.2% MAC in a mixture of house air and oxygen to maintain a surgical plane of anesthesia. Ensure the animal is in a deep plane of anesthesia prior to any manipulations by checking for the absence of jaw tone and keeping the anesthesia above the minimum alveolar concentration for swine. Initial anesthetic depth check is conducted by assuring the absence of jaw tone and the isoflurane levels are monitored continuously throughout the procedure (>1.5 MAC) to ensure a deep plane of anesthesia.
- Carefully access the right external jugular and carotid artery with cautery and blunt dissection. Place an 8.5F Swan-Ganz catheter in the external jugular and inflate the balloon to 1.5 cc. Then traverse through the right atrium, into the ventricle and through the pulmonic valve down the pulmonary artery until a wedge pressure is felt.
- Deflate the balloon and leave the catheter in this position. Record the right atrial pressure and pulmonary artery pressure using the balloon. Additionally, record the wedge pressure or pressure in the lung (or if the lungs are considered normal, then also record the left atrial pressure).
NOTE: This catheter also allows for estimates of the cardiac output. - Place an additional 5.0F balloon pressure catheter in the external jugular and into the right ventricle to continuously record pressure.
- Place a 5.0F balloon pressure catheter in the carotid artery, prolapse through the aortic valve and maintain in the left ventricle. Flush all pressure catheters with 20 units/ml heparanized saline connected to a pressure transducer, and record all pressure data from the left ventricle, right ventricle (and estimated cardiac output), pulmonary artery pressure and right atrial pressure.
- For peripheral monitoring, access a branch of the femoral artery by placing an 18F catheter for real-time blood pressure or blood gas monitoring. Record heart rate and temperature during the procedure.
- Carefully access the left external jugular with cautery and blunt dissection. Place two 11.0F hemostasis introducers in the jugular and secure with 0 silk sutures. Place steerable catheters in the introducers.
- Under fluoroscopic guidance, place active fixation leads in the right atrial appendage and the apex of the right ventricle.
NOTE: A fixation lead is a surgically implanted wire that connects the heart to an implanted pacemaker. - Connectanalyzer cables to the leads and test for capture utilizing a programmer. Set the parameters to 8V, 0.25 msec duration, and set the pacing rate at a minimum of 10 bpm higher than the intrinsic rate at that time. Record the relative impedance for each lead.
- Make a medial surgical incision from the xiphoid process to near the insertion of the sternocleidomastoid muscles. Use a sternal saw to remove the anterior protrusion from the sternum (keel bone) to enable the partial medial dissection of the sternum. Use a shear cut through the remaining portions of sternal bone structure. Dissect the sternal-pericardial ligament and retract the sternum.
- Use blunt dissection to separate the pericardium from the pleural linings. Make a medial sagittal incision (3-5 cm) in the pericardium and create a pericardial cradle with four square knot sutures at each corner (right, left, superior and inferior sites).
- Place a temporary bipolar lead in the apical region of the left ventricle and place a unipolar plunge temporary pacing lead into the left atrial appendage.
- Euthanasia is accomplished by removal the heart under deep anesthesia.
2. Preparation for Electrophysiological Monitoring
- Cardiac Mapping System.
- Select an AF study in a cardiac mapping system Connect the ventricular epicardial bipolar pacing leads and the epicardial leads in the atrial appendage with alligator clips to the appropriate settings in the breakout box. Connect an EKG and ground pads to the system.
- Oscilloscope and Grass Stimulator.
- Connect the bipolar left ventricular pacing lead and unipolar atrial lead in the breakout box to a Grass stimulator which is connected to an oscilloscope for electrical verification.
- Programmed Electrophysiological Stimulation.
- Secure the right atrial leads and right ventricle leads in a pacemaker Place the programmer telemetry head over the pacemaker. Select the pacing electrode stimulation (PES) study and set the parameters to 8V; remove all patient parameters. Set the pacing duration set to 8 pulses at 400 msec (or 300 msec).
3. In Situ Study
- Refractory Period: Study Paradigm.
- Determine the atrial effective refractory period (AERP), atrial ventricular node refractory period (AVNERP) and the ventricular effective refractory period (VERP) at baseline, and at 30 and 60 min post pericardial delivery of compound/drug/control treatment; additional time points may be added as desired.
- Refractory Period: Programmer Settings.
- Burst induce the PES study parameter to 8 paces (400 msec or 300 msec) followed by a minimum of 300 msec pacing. Reduce the pacing until the ventricles/atrium (respectively) fail to contract. This is noted from the sensing of the pacing leads; thus determining the relative refractory period.
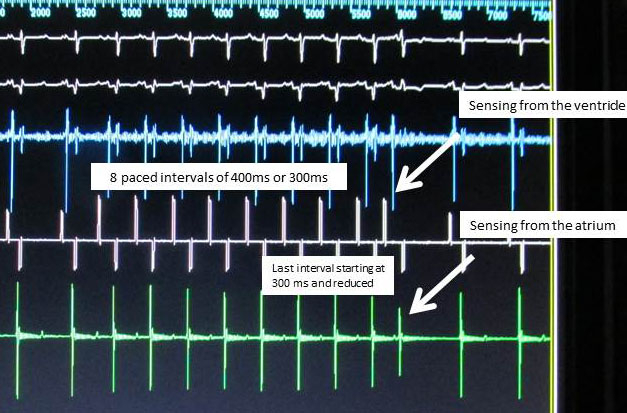
Figure 2. EnSiteSystem: AERP, AVNERP and VERP Determination Please click here to view a larger version of this figure.
- Determination of Relative AF Burden: Parameters.
- Sustain the animal’s heart in AF, after 1 min, allow it to remain in AF for up to 10 min: i.e., before shocking the atria with direct paddles at 5 joules to terminate AF. Elicit AF induction up to 10 times at each time point. Note, in this study. AF is defined as an erratic rhythm with an absence of the P wave.
- AF Burden: Grass Stimulator and Oscilloscope Settings.
- Optimize the parameters for the Grass stimulator to deliver 4 Hz with a 2 sec pulse duration to the left atrial appendage (LAA) via the plunge pacing lead; verify this by a standard oscilloscope. Deliver a single pulse to the LAA to induce AF.
4. Heart Explantation and Reanimation (Transplant Model)
- Aortic Root Cannula.
- Carefully dissect the pericardial tissue around the ascending aorta and remove the pericardium.Suture two points (2-3 cm apart) of 2.0 Ethibond suture in the ascending aorta, and administer 30,000 units of Heparin intravenously.
- Place the aortic root cannula between the suture points and secure the aorta. With the delivery system pressurized, remove the stylet-bevel and place a clamp on the cannula not allowing for flow.
- Cardioplegia Preparation.
- Administer cold St. Thomas cardioplegia solution into the ascending aorta under a pressure of 150 mm/hg via a pressurized bag. Secure an irrigation catheter that is attached to the pressurized cardioplegia with a 3-way stop cock on the distal end. Secure the stop cock to the aortic root cannula, release a steady flush of cardioplegia through the catheter and secure to the aortic root cannula.
- Cross-Clamp.
- Clamp the inferior vena cava with an atraumaticclamp 1-2 cm just superior to the diaphragm. Clamp the ascending aorta with atraumatic angled camp 1-2 cm on the ascending aorta superior to the aortic root cannula.
- Cross-Clamp/Cardioplegia.
- Remove the clamp from the aortic root cannula and flush the cardioplegia at 150 mm/hg toward the aortic valve, closing the aortic valve and perfusing the coronaries.
- Clamp the superior vena cava and make a small incision in the pulmonary artery, so as not to over pressurize the heart. Once the heart is stopped (asystolic), excise and remove heart from the chest and place in a bath of cold Krebs-Henseleit buffer (~3-8 °C).
- Reanimation.
- Cannulate the great vessels and prepare the heart utilizing Visible Heart methodologies (3). Once the perfused heart reaches 37±5 °C, restore a native sinus rhythm by delivering 34 J shocks to the ventricles via epicardial patch electrodes.
5. In Vitro Study Paradigm
- Continuously monitor cardiac function for 60 min post reanimation. Continuously monitor echocardiography in 2D mode with a short-axis view: an LV view just below the mitral valve.
- Calculate ventricular wall thickness and ejection fractions every 10 min post reanimation (see below). Take samples from the coronary sinus (1 cc) at -5 min and every 5 min during the evaluation period.
- Monitoring.
- Monitor the hemodynamics for both the left and right ventricles, including pressures, flows and volume changes.
- Echocardiography: Ejection Fraction.
- Place a transthoracic echo probe directly on the heart, capturing a mid-papillary short-axis view. Calculate the ejection fraction (EF %) in 4-chamber working mode every 10 min using the equation: LV End Diastolic Volume − LV End Systolic Volume X 100/LV End Diastolic volume
- Echocardiography: Left Ventricular Wall Thickness.
- Measure ventricular wall thickness (cm) from a mid-papillary short-axis window at 10 min intervals for an hour post reanimation. Measure four corners of the left ventricle using a screen calipers and take the average.
- Myocardial Metabolism.
- Place a steerable catheter in the coronary sinus (CS). Sample 1 cc from the CS 5 min before reanimation and every 5 min post reanimation for 1 hr. Test the samples for lactate and glucose levels; other blood gases can also be assessed.
These results are characteristic of the data that can be collected utilizing this target delivery model of pharmacological agents in the swine. This data demonstrated notable increases in these ventricle effective refractory periods (VERP) following a DHA infusion in situ. In addition, the data establishes an increase in left ventricular pressure of DHA compared to control in vitro. The LV pressure in the DHA treated hearts were significantly higher compared to control at several time-points. This data validates a pharmacological window for testing treatment strategies in situ and in vitro.
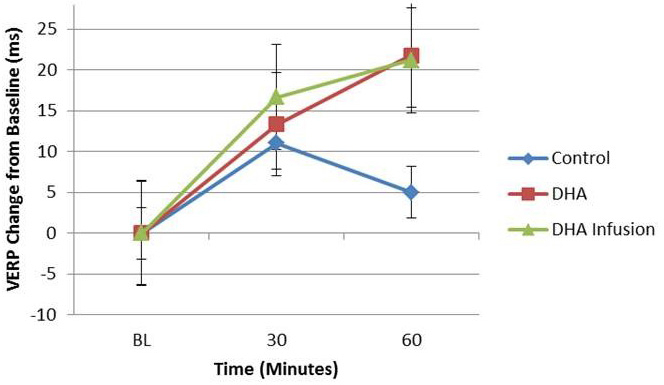
Figure 3. Change in the Ventricle Effective Refractory Period (VERP). The Ventricle Effective Refractory Period (VERP) was determined 5 min before pericardial delivery of control agent (saline) or docosahexaenoic acid (DHA), or DHA infusion, in addition to 30 and 60 min post-pericardial delivery of either the treatments or control. The VERP of the DHA group trended toward increasing compared to controls. Please click here to view a larger version of this figure.
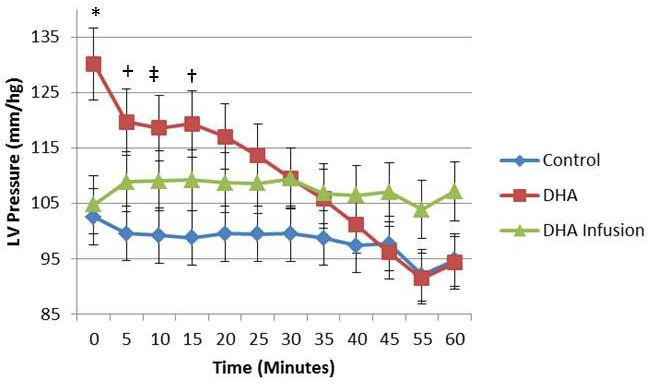
Figure 4. Pressure of Left Ventricle in 4-Chamber Working Model The maximum pressure (mmHg) was determined every 5 min for 60 min after the heart was reanimated using the visible heart methodologies. DHA and DHA infusion (treated for over 10 min) treated hearts trended to elicit initial higher pressure than control for the majority of the testing period. An un-paired T-test was completed for each time-point. (*, P=0.065, +, P=0.056, †, P=0.059 ‡.P=0.058) Please click here to view a larger version of this figure.
The Ventricle Effective Refractory Period (VERP) was determined 5 min before pericardial delivery of control agent (saline) or docosahexaenoic acid (DHA), or DHA infusion (over 10 min), in addition to 30 and 60 min post-pericardial delivery of either the treatments or control. The VERP of the DHA group trended toward increasing compared to controls.
The maximum pressure (mmHg) was determined every 5 min for 60 min after the heart was reanimated using the visible heart methodologies. DHA and DHA infusion treated hearts trended to elicit initial higher pressure than control for the majority of the testing period. An un-paired T-test was completed for each time-point. (*, P=0.065, +, P=0.056, †, P=0.059 ‡.P=0.058)
