A number of observations and analyses can be performed on the liver during perfusion, including direct real time observations, such as flow rates and bile production; real time measurements, such as gas analysis of the perfusate, and post-hoc measurements that are made after sample collection including biochemical analysis of the perfusate and tissue and histological analysis. Results mentioned here are from 22 perfused human livers. Livers were rejected for transplantation for various reasons, including donor age, excessive warm ischemic time, biopsy results (steatosis, inflammation, fibrosis) and for logistical reasons. 18 livers were procured following cardiac death, and 4 following brain death. In both cases, donors were pretreated with 30,000 units of heparin and flushed in situ and on the back table with UW solution. Mean cold ischemic time was 531 ± 237(SD) min and the mean warm ischemic time was 27 ± 10(SD) min, measured from withdrawal of life support to cold flush. Real time observations and measurements can be used to assess the liver during perfusion, while post-hoc measurements are revealed after the perfusion.
Real time observations
Flow through the liver begins lower than the target flow rates, as a result of a higher resistance in the cold liver. Using a pressure of 3 mmHg on the PV and 30 mmHg on the HA the target flows can generally be achieved once the liver has warmed up to 21 °C after 60 min of perfusion (Figure 1A). Bile flow can generally be observed within 10 min of perfusion and is produced steadily during perfusion (Figure 1B). Bile quantity depends on the quality of the liver and ranges from 0.3 ml/ hr/ kg liver to 18 ml/min/kg. In livers with longer warm ischemic time, bile flow will tend to taper off, while shorter warm ischemic time results in a more steady or even increasing bile production.
Real time measurements
Direct and frequent measurement of the perfusate by blood gas analysis in essential for both experimental purposes as well as maintaining adequate perfusion conditions, importantly oxygenation and pH. Dissolved oxygen partial pressure should be greater than 700 mmHg on the inflow of both the PV and HA. Outflow oxygen pressure, measured in the vena cava, generally decreases with longer perfusion, reflecting an increasing oxygen uptake. Oxygen uptake rates can be calculated as described previously 13 and ranged from 0.5–2.2 ml O2/ min/ kg at the beginning of perfusion to 2.4-9.7 ml O2/ min/ kg at t =3 hr (Figure 1C). A drop in pH is observed in the first 30 min (Figure 1D), primarily as a result of lactate release in the perfusate. This can be supported by supplementation with 8.4% sodium bicarbonate and after about 90 min the pH falls back into normal range. Commonly, 30-50 ml of 8.4% sodium bicarbonate is required. Lactate concentration increases rapidly in the first 15-30 min, but begins to decease after the first hour (Figure 1E).
Post-hoc measurements
Hepatic transaminases such as ALT can be measured in the perfusate. In the first 30 min a large increase of ALT is generally observed which reflects the washout of ALT that was released during ischemia (Figure 1F). ALT was shown to correlate well with warm ischemic time 13. Machine perfusion increased ATP content 2.8 fold, reflecting a recovery energy status (Figure 1G). H&E histological analysis reveals no additional injury sustained during machine perfusion (Figure 1H, I). It should be noted that the biopsy regimen proposed in this protocol is for research purposes and may not be applicable for clinical purposes.
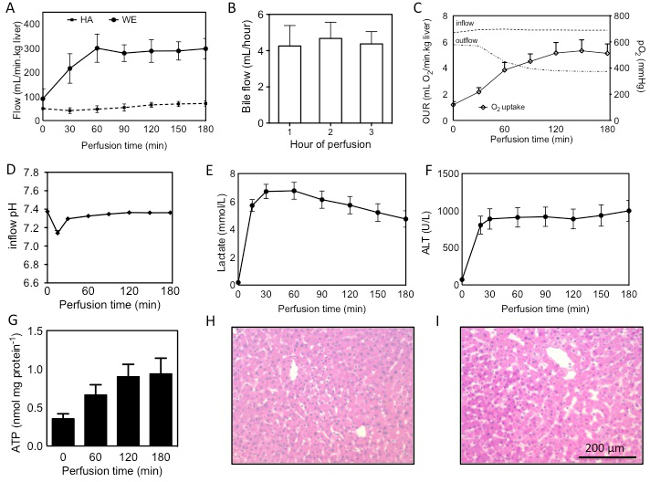
Figure 1: Assessment of human livers during machine perfusion. Flow through the PV and HA during SNMP (A), bile production, quantified per hour of perfusion (B), oxygen uprate rate (OUR), calculated from the difference in inflow (PV+HA) and outflow (vena cava), interrupted lines show partial oxygen pressures in the in- and outflow during perfusion (C), pH and lactate during perfusion (D, E), release of ALT into the perfusate (F), ATP content measured in tissue from hourly biopsies (G) and H&E stains of the liver (54 year old DCD, 19 min warm ischemia, 559 min cold ischemia) before (H) and after (I) perfusion. Results are presented as mean ± SEM. Please click here to view a larger version of this figure.
