Feasability
This piglet model of chronic post-embolic pulmonary hypertension has been established in our laboratory in 2009-2010. Since 2011, we used 70 piglets and we performed 63 completed models. In our experience, the realization of this model required a learning curve.
Regarding the mortality, we observed 5 unplanned deaths (7.1%), mainly in the first part of our experience. The two critical steps were first, the pulmonary embolization and second, the endomyocardial biopsies. Four piglets died from severe acute right heart failure after pulmonary embolization. One piglet died from an unknown cause. Regarding the morbidity, 4 piglets (5.7%) had a major complication during procedures.
Two piglets needed urgent pericardial drainage during the endomyocardial biopsies procedure. They required urgent pericardo-synthesis because of a perforation of the right ventricular free wall. The recovery was uneventful in all cases. Since the use of echographic guidance to perform endomyocardial biopsies, we did not observe this complication anymore.
Two others piglets developed a pyothorax after the pulmonary artery ligation and they required euthanasia 7 days after de surgery.
We used Large White piglets with an average weight of 20 kg. All animals were males and came from a French farm (Gambais, France). The first hours after the surgery, the piglets were placed in a specific room with oxygen and underfloor heating. Then, they were housed alone or with another piglet in a 2 m2 cage.
The model of Chronic Pulmonary Hypertension in piglet was fulfilled 6 weeks after the left pulmonary ligation and 5 repeated embolizations (Figure 1). The left pulmonary artery was ligated through a small lateral thoracotomy. The first embolization of the right lower pulmonary artery was performed 5 days later. Embolizations are repeated weekly during 5 weeks with an average of 3.2±0.8 ml of N-butyl-2-cyanoacrylate per embolization. Effects on hemodynamics, pulmonary vasculature and right ventricle can be described as follows.
The sham animals underwent only a left thoracotomy without left pulmonary artery ligation. They do not have embolization of the pulmonary arteries but underwent repeated hemodynamics, echocardiographic and histologic assessments at the same time as the other animals.
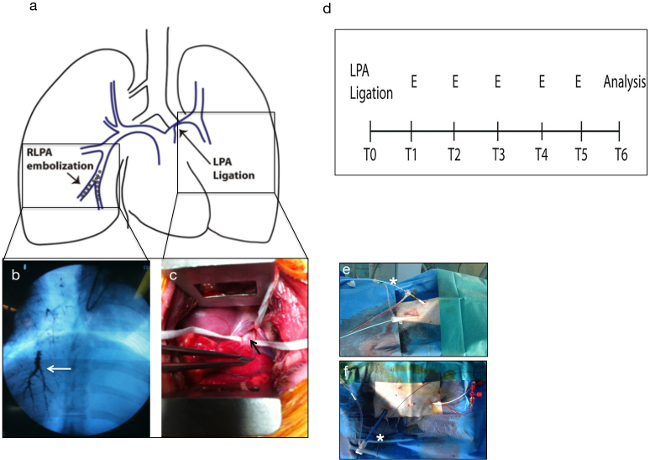
Figure 1. CTEPH animal model design. The left pulmonary artery ligation was followed by repeated embolization of the lower pulmonary lobe artery (A and D). LPA ligation (arrow) was performed through a small left thoracotomy (C). Embolizations were performed with fluoroscopic guidance weekly for 5 weeks (B). All experiments were performed under general anesthesia and percutaneous vascular accesses were used for embolizations and pressure measurements: (E) percutaneous superior veina cava (star) and right carotid artery catherization. (F) 8Fr sheath in the right femoral vein (star) and arterial thermodilution sheath sensor in the left femoral artery. Please click here to view a larger version of this figure.
Hemodynamic results
The mean pulmonary arterial pressure (mPAP) increased progressively after embolizations above 25 mm Hg. Hemodynamic data are summarized in Table 1. The right atrial pressure, the mPAP/mSAP ratio and the pulmonary vascular resistances also increased after repeated embolizations. The Cardiac Index trended to decrease after several embolizations, reflecting the RV dysfunction. The mPAP/mSAP ratio also increased progressively. This ratio must not exceed 0.5 just after acute embolization because of the increased risk of death. For this reason, embolizations must be performed with a maximum of 2 ml per injection. Reinjection of 1 ml can be performed if the previous one was well tolerated hemodynamically. In this model, the PH was only precapillary because the PCWP did not increase.
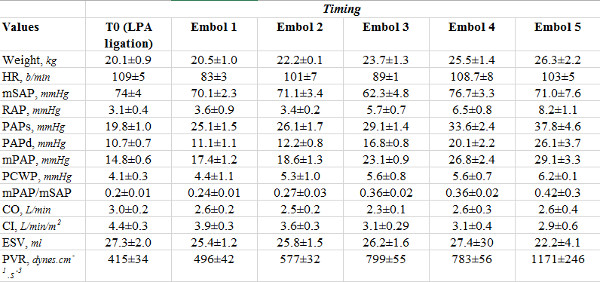
Table 1. Hemodynamic data from 8 piglets models of CTEPH. HR: heart rate; mSAP: mean systemic arterial pressure; RAP: right atrial pressure; PAPs: systolic pulmonary arterial pressure; PAPd: diastolic pulmonary arterial pressure; mPAP: mean pulmonary arterial pressure; PCWP: pulmonary capillary wedge pressure; CO: cardiac output; CI: cardiac index; ESV: ejection systolic volume; PVR: pulmonary vascular resistances.
Remodeling of pulmonary arteries
Bronchial circulation hypertrophy was noted in the left lung, the right lower lobe and along the mediastinal pleura. In pathology, large and numerous submucosal bronchial arteries were observed in the obstructive lungs (left lung and right lower lobe), reflecting the increase of angiogenesis in these territories. (Figure 2) Post obstructive pulmonary vasculopathy with media hypertrophy was also found in obstructed territories (left lung and right lower lobe), while overflow vasculopathy was observed in the non-obstructive territories (right upper lobe). (Figure 3) Pathology also showed the chronic obstruction of the right lower pulmonary artery lobe by an unresolved thrombus of N-butyl-2-cyanoacrylate and fibrin.
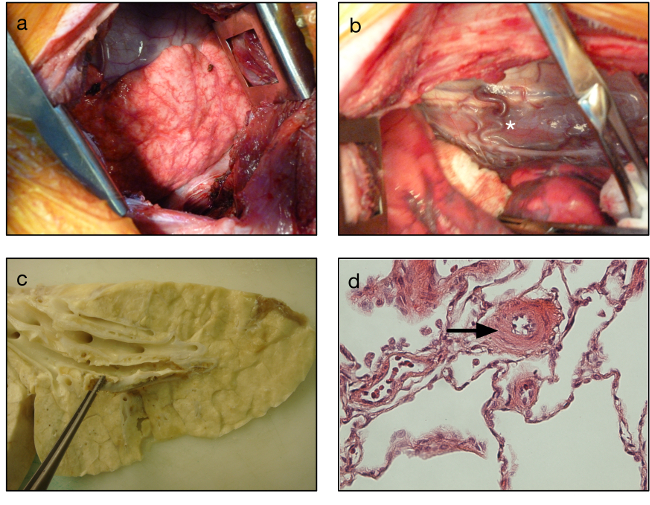
Figure 2. Vascular remodeling in the CTEPH model. Intraoperative views showing the development of bronchial arteries in the left lung and visceral pleura (A) and in the mediastinum (star, B). Gross anatomy of the harvested right lower lobe showing the unresolved intravascular clots (C). Media hypertrophy in the small pulmonary arteries seen in light microscopy (arrow) (D). Please click here to view a larger version of this figure.
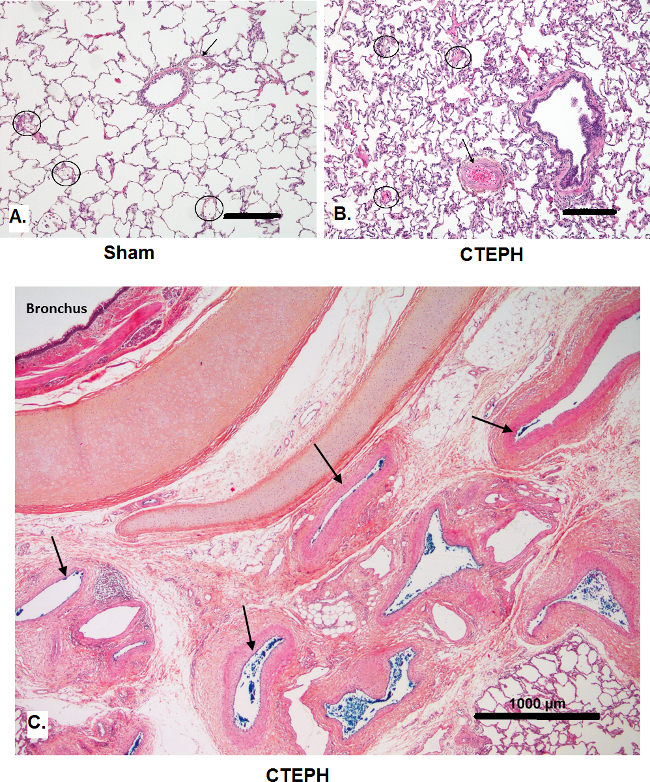
Figure 3. Comparative pulmonary vascular remodeling in Sham and CTEPH animals (Hematoxylin and eosin staining). Histology from a sham piglet (A): the pulmonary artery (arrow) and three microvessels (circles) display slender walls and no hypertrophic changes can be observed. In a CTEPH piglet after 5 weeks (B), pulmonary arteries (arrow) in the periphery of the upper right lobe show medial thickening. However, microvessels (circles) in this territory present with only very mild changes (scale bars, 200 µm). At higher magnification (C), bronchial arteries (arrows) from the upper right lobe (unobstructed territory) appear unremodelled and of normal size in a CTEPH piglet at 5 weeks (scale bar, 1,000 µm). Please click here to view a larger version of this figure.
Remodeling of right ventricle
Significant enlargement associated with right ventricular hypertrophy and fibrosis was observed after 6 weeks (Table 2 and Figure 4 and video 1 and video 2). The RV area, Right Atrial (RA) area, RV diameters were increased after repeated embolizations. The RV wall thickness also increased. RV hypertrophy was confirmed in light microscopy after heart’s harvesting. In echocardiography, Tricsupid Annula Plane Systolic Excursion (TAPSE) and Right Ventricular Fractionnal Area Change (RVFAC) were decreased after 6 weeks reflecting RV dysfunction in this model. RV function impairment was also found with PVL analysis with a decrease of the ventricular-arterial coupling (Table 3).
| Timing | ||
| Values | T0 (LPA ligation) | 6 weeks |
| RV diastole area, cm2 | 4.5±0.2 | 7.1±0.9 |
| RV basal diameter, cm | 1.5±0.8 | 3.7±1.3 |
| RV free wall thickness, cm | 0.3±0.02 | 0.59±0.04 |
| RA area, cm2 | 3.9±0.4 | 5.9±0.3 |
| RVFAC, % | 0.50±0.03 | 25.0±1.0 |
| RV TAPSE, cm | 1.6±0.2 | 1.11±0.07 |
| LV EF, % | 55.7±4.9 | 52.2±6.0 |
Table 2. RV remodeling in echocardiography. RVFAC: right ventricular fractional area change; TAPSE: tricuspid annular plane excursion; LV EF: left ventricular ejection fraction.
| Timing | ||
| Values | T0 (LPA ligation) | 6 weeks |
| RV Stroke Work, mm Hg.ml-1 | 579±55 | 2248±148 |
| RV Elastance, Ees | 0.33±0.06 | 0.40±0.06 |
| Pulmonary arterial Elastance, Ea | 0.32±0.05 | 0.51±0.03 |
| RV coupling, Ees/Ea | 1.33±0.19 | 0.78±1.0 |
Table 3. Functional remodeling of right ventricle in Pressure-Volume Loops analysis.
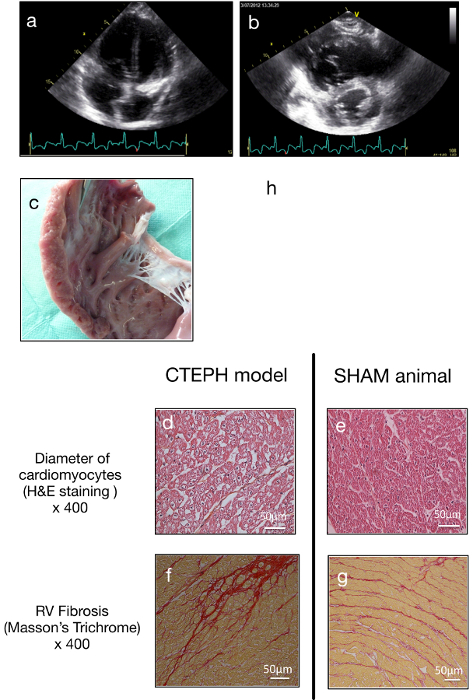
Figure 4. Right ventricular remodeling. Echocardiography showed enlargement of the right ventricle in the four cavities view (A) and short parasternal axis (B). Note the shift of the interventricular septum and the compression on the left ventricle. RV hypertrophy was confirmed macroscopically (C) and by light microscopy with enlargement of transversal axis of cardiomyocytes compared with sham (D and E). As showed in (H), the Fulton ratio correlated with the mean pulmonary arterial pressure. RV fibrosis rate was increased in the CTEPH animals compared to SHAM (F and G). Please click here to view a larger version of this figure.
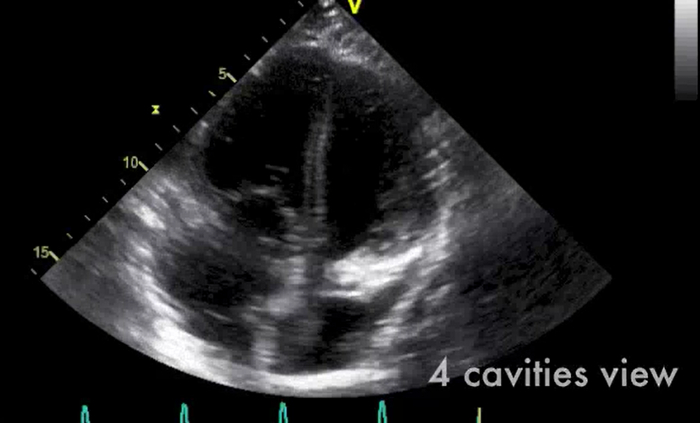
Video 1: Transthoracic 4 cavities and short axis views showing enlargement of the right ventricle. Please click here to view this video.
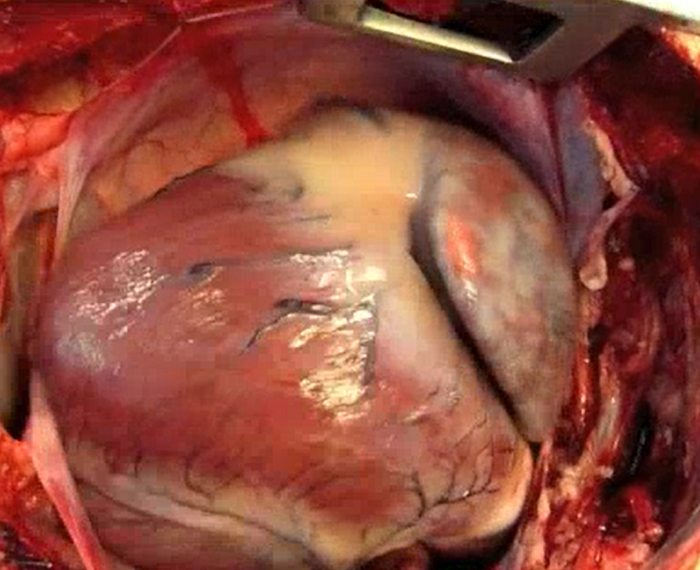
Video 2: Operative view after median sternotomy. The dilated right ventricle fill the pericardium. Please click here to view this video.
In order to perform a genetic and metabolic study, a technique of endomyocardial biopsies of the right ventricle was developed in the present model of chronic pressure overload. This technique is safe and allows repeated fresh myocardial sampling in anesthetized piglets. Echocardiographic and fluoroscopic control reduced the risk of RV wall perforation with the biotome. The long catheter technique is a good strategy to avoid tricuspid valve injury (Figure 5).
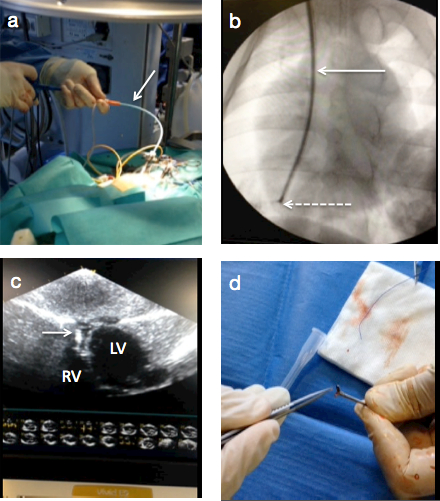
Figure 5. Endomyocardial biopsies in the CTEPH model. (A) a 55 cm jugular biotome is insert in the right ventricle through a transcutaneous 7 Fr long catheter sheath. Forceps progression was controlled with echocardiography (C) and fluoroscopy (B) and a 6mm3 myocardial piece is extracted (D). Please click here to view a larger version of this figure.
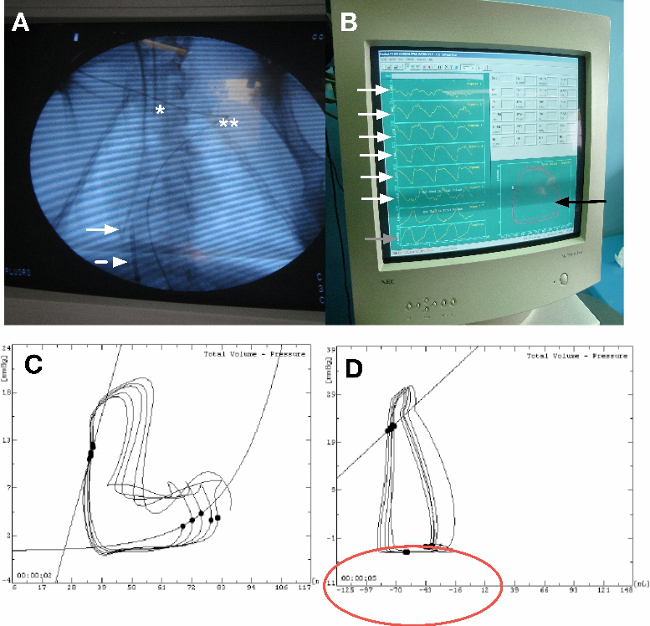
Figure 6. Appropriate placement of the conductance probe for PV loops assessment. (A) Place the end of the probe at the apex of the right ventricle under fluoroscopic guidance (solid arrow). Insert minimum 3 segments in the right ventricle and the probe has to be straight line. Insert an occlusion balloon in the inferior veina cava through the femoral vein. The end of the balloon must be just at the right atrium entry (dashed arrow) (*: intubation probe; ** EKG wire. (B) Verify that the volume segments of the probe must be in phase in diastole and systole and the “good shap of the loop on the screen. (C) Example of bad shape of the PV loop due to a wrong placement of the volume segments in the right ventricle. (D) Example of a bad volume calibration. The ventricular volumes are negatives. Please click here to view a larger version of this figure.
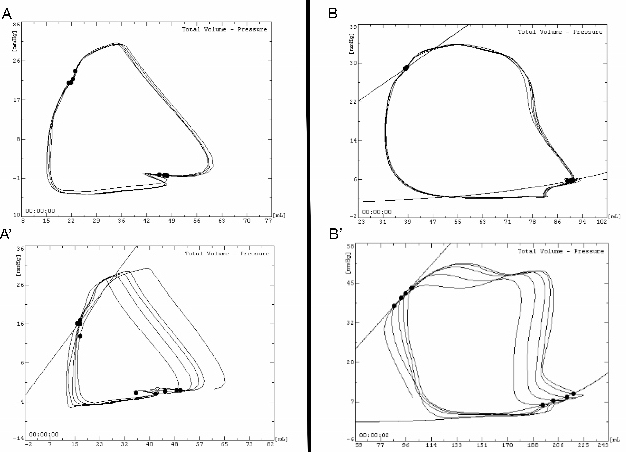
Figure 7. Example of PV loop shape at basal state and during inferior veina cava occlusion in SHAM (A and A’) and CTEPH piglet (B and B’). PV loop in normal right ventricle has a triangle shape, with lower pressure and volume values compared with right ventricle under pulmonary hypertension. Please click here to view a larger version of this figure.
