The injection of magnetic microbeads into the anterior chamber of adult mice described in this protocol resulted in a robust and reproducible elevation of IOP. One week after the procedure, IOP increased from 10 ± 0.6 mm Hg (mean ± S.E.M.), the average baseline IOP in contralateral eyes, to 19 ± 0.5 mm Hg in hypertensive eyes (Student's t-test; ***p <0.001, n = 12, Table 1, Figure 2). IOP stabilized thereafter and remained elevated at an average of 20 mm Hg for at least 6 weeks, the longest time-point examined in this study. The average peak IOP in microbead-injected eyes at 2, 3, and 6 weeks after surgery was 25 mm Hg. The vast majority of treated mice developed sustained high IOP, therefore this protocol does not require a second injection of microbeads.
To assess the time-course of RGC loss in this model, RGC soma were first quantified by immunostaining with Brn3a, a RGC-specific marker 17. The number of Brn3a-positive cells was quantified on flat-mounted retinas at 1, 2, 3 and 6 weeks after induction of ocular hypertension. Although a significant IOP elevation was detected as early as 1 week after microbead injection, no significant loss of RGC soma was observed within the first 2 weeks of the procedure (Figure 3). Substantial RGC death (22%), however, was evident at 3 weeks (2,430 ± 67 RGCs/mm2, mean ± S.E.M., n = 12) and 6 weeks (2,350 ± 74 RGCs/mm2, n = 10) post-induction of ocular hypertension, compared to intact control eyes from un-operated mice (3,141 ± 49 RGCs/mm2, n = 23) (ANOVA, p <0.001).
Dysfunction and degeneration of RGC axons is a cardinal feature of glaucoma. Therefore, axonal loss was examined at 3 and 6 weeks after microbead injection by quantification of RGC axons in optic nerve cross-sections stained with toluidine blue (Figure 4). A substantial loss of RGC axons (25%) was observed at 3 weeks (28,401 ± 702 axons/nerve, mean ± S.E.M., n = 5) and 6 weeks (29,426 ± 948 axons/ nerve, n = 6) after injection of microbeads compared to intact optic nerves from un-operated eyes (39,467 ± 137 axons/nerve, n = 4) (ANOVA, p <0.001). Collectively, these data demonstrate that injection of magnetic microbeads into the mouse anterior chamber leads to reproducible and sustained IOP elevation that results in RGC soma and axon degeneration.
| Time after OHT surgery | N | Mean IOP (mmHg) ± S.E.M | Peak IOP (mmHg) | ||||
| Contralateral | Glaucoma | Difference | Contralateral | Glaucoma | |||
| 1 week | 12 | 10 ± 0.4 | 19 ± 0.5 | 9 ± 0.6 | 12 ± 0.4 | 22 ± 0.6 | |
| 2 weeks | 13 | 11 ± 0.5 | 20 ± 0.8 | 9 ± 0.5 | 12 ± 0.9 | 25 ± 0.7 | |
| 3 weeks | 10 | 11 ± 0.8 | 20 ± 0.7 | 10 ± 0.9 | 13 ± 0.2 | 25 ± 0.9 | |
| 6 weeks | 12 | 12 ± 0.5 | 20 ± 0.6 | 9 ± 0.7 | 13 ± 0.5 | 24 ± 0.6 | |
Table 1. Elevation of Intraocular Pressure in the Murine Magnetic Microbead Occlusion Model. In awake female C57 BL/6 mice, IOP was measured using a calibrated rebound tonometer. Operated eyes displayed an increase in IOP detected at one week post-surgery that remained elevated for at least six weeks after the procedure.
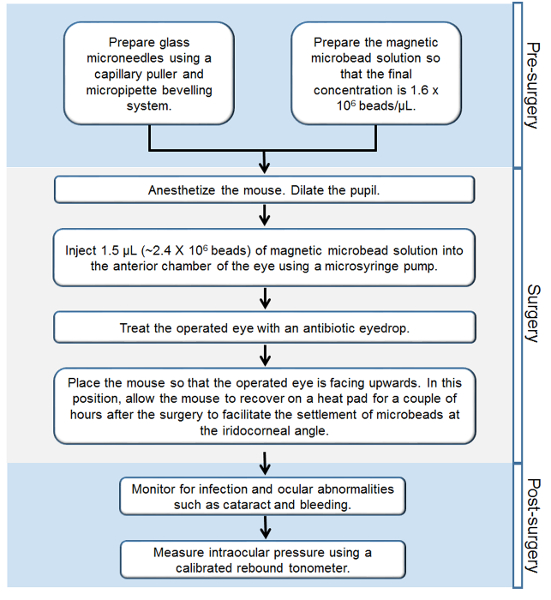
Figure 1. Workflow of the Steps Involved in the Murine Magnetic Microbead Occlusion Model of Glaucoma. Step-by-step outline of all the procedures performed before, during, and after the surgery. Please click here to view a larger version of this figure.
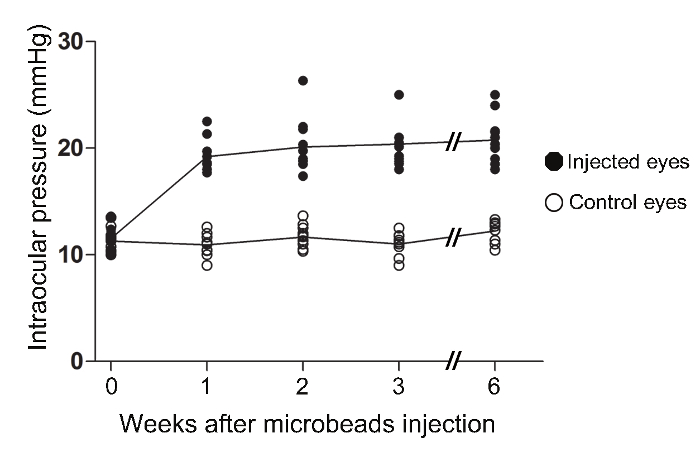
Figure 2. Increase in Intraocular Pressure in the Murine Magnetic Microbead Occlusion Model. In awake female C57 BL/6 mice, IOP was measured using a calibrated rebound tonometer. The IOPs of microbead-injected eyes were significantly elevated at one week post-surgery (ANOVA, p <0.001). The IOPs remained significantly elevated relative to the contralateral eye of injected mice for at least 6 weeks (ANOVA, p <0.001). (Intact: n = 12; 1 week: n = 12, 2 weeks: n = 13, 3 weeks: n = 10, 6 weeks: n = 12). Please click here to view a larger version of this figure.
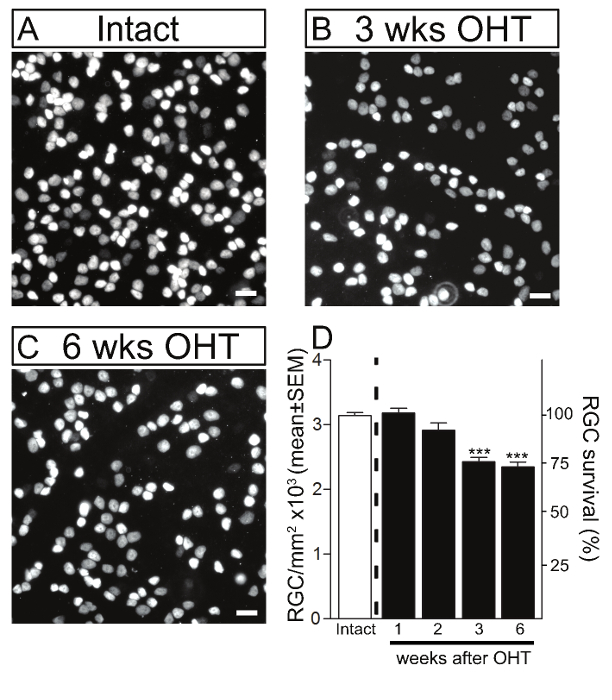
Figure 3. Retinal Ganglion Cell Death in the Murine Magnetic Microbead Occlusion Model. RGCs were visualized by immunostaining of flat-mounted retinas using Brn3a in intact control retinas (A) and glaucomatous retinas at 3 and 6 weeks after microbead injection to induce ocular hypertension (OHT) (B, C). Scale bars: 20 µm. (D) Quantitative analysis confirmed that microbead injection resulted in significant RGC soma loss at 3 and 6 weeks after the procedure compared to control eyes. The density of RGC soma in intact, non-glaucomatous C57/BL6 mice is shown as reference (white bars, 100% survival). Values are expressed as the mean ± S.E.M. (Intact: n = 23; 1 week: n = 6, 2 weeks: n = 6, 3 weeks: n = 12, 6 weeks: n = 10, ANOVA, *** p <0.001). Please click here to view a larger version of this figure.
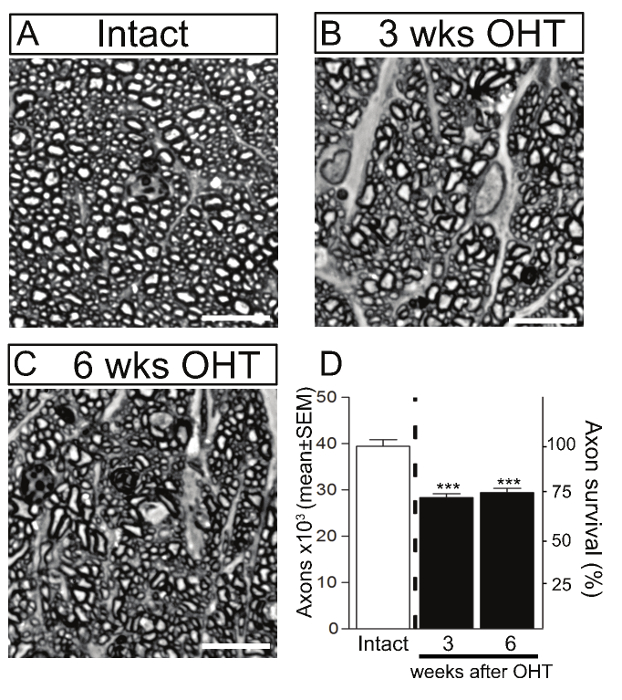
Figure 4. Axonal Degeneration in the Murine Magnetic Microbead Occlusion Model. RGC axons were visualized by staining of optic nerve cross-sections with toluidine blue in intact control (A) and glaucomatous retinas at 3 and 6 weeks after microbead injection to induce ocular hypertension (OHT) (B, C). Scale bars: 10 µm. (D) Quantitative analysis confirmed that microbead injection resulted in significant RGC axon loss at 3 and 6 weeks after the procedure compared to control eyes. The density of RGC axons in intact, non-glaucomatous C57/BL6 mice is shown as reference (white bars, 100% survival). Values are expressed as the mean ± S.E.M. (Intact: n = 4; 3 weeks: n = 5, 6 weeks: n = 6, ANOVA, *** p <0.001). Please click here to view a larger version of this figure.
