Figure 1 shows B-mode images of the aortic arch view of mouse heart subjected to sham (Figure 1A) or TAC surgery (Figure 1B). The aortic arch, innominate artery, left common carotid artery, and left subclavian artery are shown. Note that aortic constriction is clearly visible in TAC but not sham heart. Color Doppler images from aortic view are shown in Figure 2A. The waveforms of aortic flow across the constriction site were captured by PW Doppler imaging (Figure 2B). Successful TAC will lead to a significantly increased flow velocity downstream the constriction site (typically ~4 m/sec in TAC mice). Pressure gradient across the constriction was calculated based on peak flow velocity, according to the modified Bernoulli's equation (Figure 2C).
Figure 3 shows B- and M-mode images of the parasternal long axis view of sham (Figure 3A) or TAC heart (Figure 3B). The upper panel shows the B-mode images of the left ventricle, the interventricular septum, and a portion of the right ventricle from sham or TAC mice. The lower panel shows the M-mode tracings of several cardiac cycles from sham or TAC mice. The measurements of cardiac dimensions are shown, including the left ventricular anterior wall thickness (LVAW), left ventricular internal diameter (LVID), left ventricular posterior wall thickness (LVPW) in diastole and systole. Note significantly increased wall thickness in mouse heart subjected to TAC compared with sham surgery.
Figure 4 shows images of the parasternal short axis view of sham (Figure 4A) or TAC heart (Figure 4B). The upper portion of each panel shows the M-mode axis (the dotted line) placed in the center of the left ventricle. The lower portion of each panel is the M-mode tracing with lines indicating cardiac dimensions as described above. As a marker of hypertrophy, ventricular and septal wall thickness can be accurately determined. Mice subjected to TAC showed increased wall thickness as assessed by LVAWd and LVPWd, ventricular dilatation as assessed by LVISd and LVISs, decreased contractility as assessed by LVFS and LVEF, and increased LV mass (Figure 5).
Figure 6 shows B-mode apical four-chamber view (Figure 6A,B) and PW Doppler images of transmitral flow patterns (Figure 6C,D). Measurements of peak E and A velocity, IVCT, IVRT, and ET are shown. The E/A ratio and MPI are calculated (Figure 6E – I). A healthy mouse heart has an E/A ratio ≥1 and a MPI value ≤0.5. In pathological conditions with diastolic or systolic cardiac dysfunction, such as in mice subjected to TAC, a decreased E/A ratio and/or an increased MPI value are typically observed.
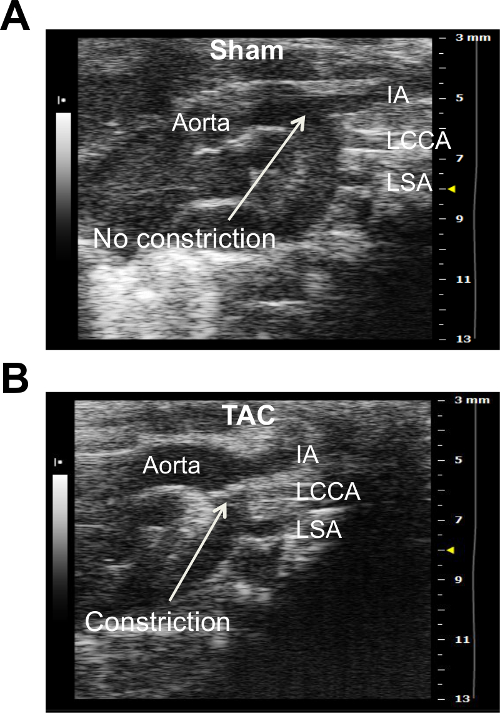
Figure 1. B-mode Image of the Aortic Arch View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). Major aortic branches including innominate artery (IA), left common carotid artery (LCCA), and left subclavian artery (LSA) are shown. Note that transverse aortic constriction (indicated by the white arrow) can be visualized in TAC but not sham heart. Please click here to view a larger version of this figure.
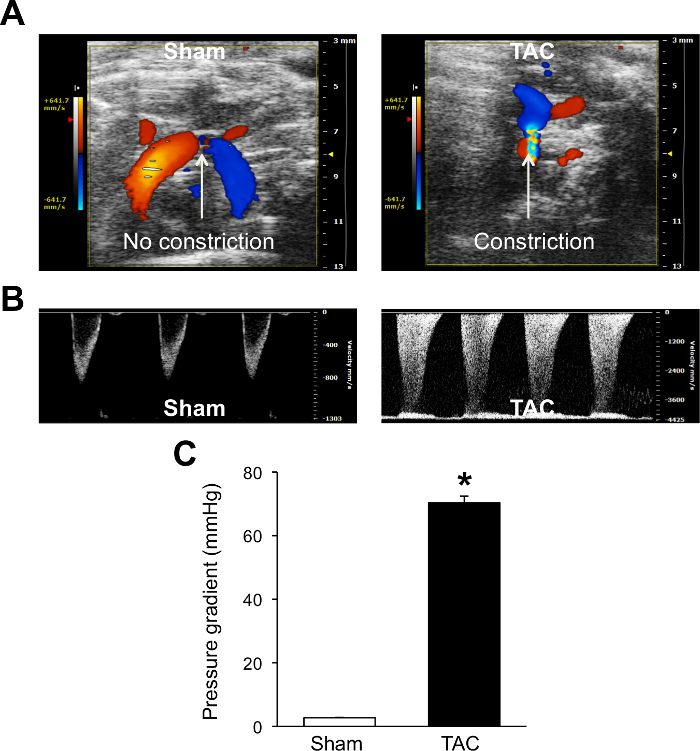
Figure 2. Color/PW Doppler Imaging of the Transverse Aorta Blood Fow from the Aortic Arch View. Color (A) and PW (B) Doppler images from sham and TAC hearts are shown. Peak aortic velocity obtained from PW Doppler imaging is used to calculate pressure gradient according to the modified Bernoulli equation (C). These data confirm a successful TAC surgery with the pressure gradient of ~70 mmHg. *P <0.05 vs. Sham. Data are expressed as mean ± s.e.m. n = 15 for Sham and n = 13 for TAC. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
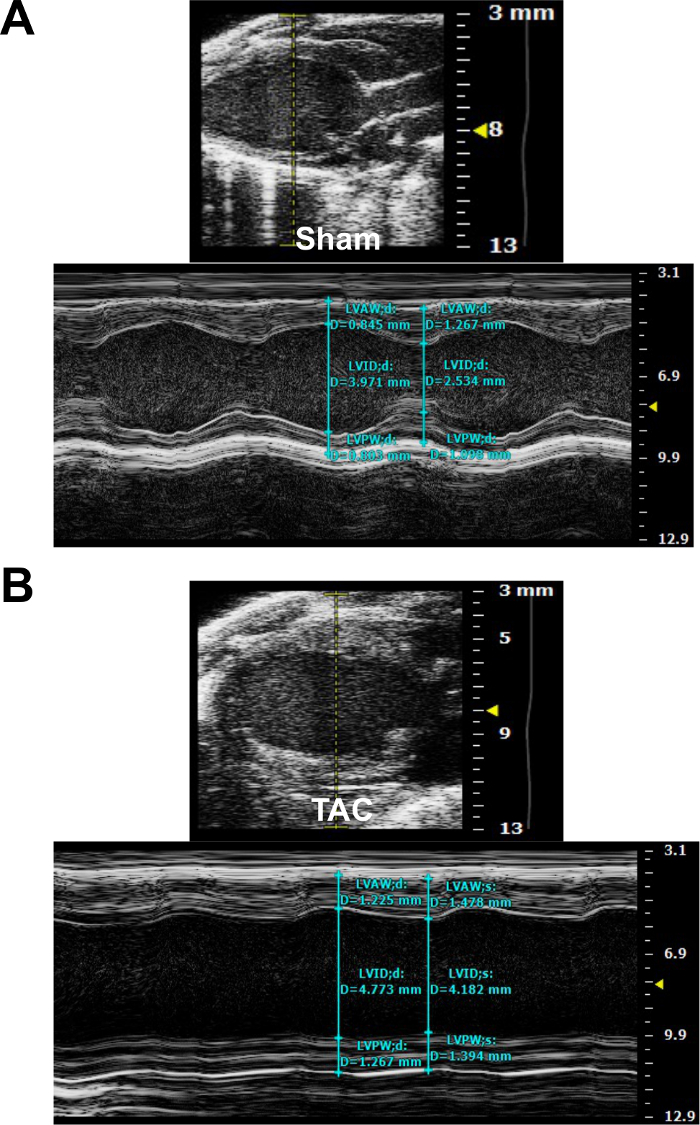
Figure 3. Parasternal Long Axis (PLAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). Please click here to view a larger version of this figure.
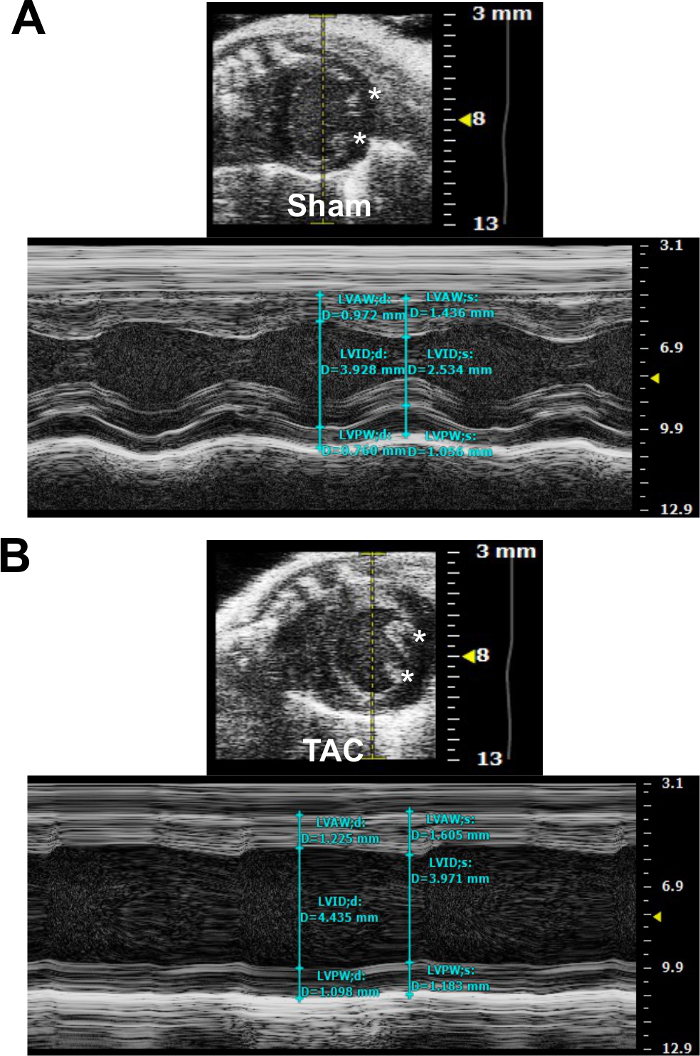
Figure 4. Parasternal Short Axis (PSAX) View of Mouse Heart Subjected to Sham Surgery (A) or TAC (B). M-mode images indicate the placement of the sample volume (dotted yellow line in the upper panel) and measurement of cardiac dimensions in diastole and systole (blue lines in the lower panel). The asterisks indicate papillary muscles. Please click here to view a larger version of this figure.
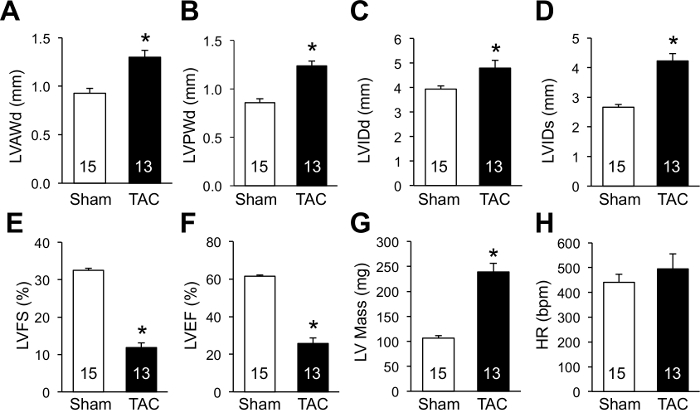
Figure 5. Echocardiographic Assessment of Cardiac Morphological and Functional Changes Following TAC. M-mode imaging in short axis view was performed as in Figure 4. (A) LVAWd, left ventricular anterior wall thickness in diastole. (B) LVPWd, left ventricular posterior wall thickness in diastole. (C) LVIDd, left ventricular internal diameter in diastole. (D) LVIDs, left ventricular internal diameter in systole. (E) LVFS, left ventricular fractional shortening. LVFS (%) = (LVIDd-LVIDs)/LVIDd x100%. (F) LVEF, left ventricular ejection fraction. LVEF (%) = (LVEDV-LVESV)/LVEDV x100%. LVEDV and LVESV denote left ventricular end-diastolic and end-systolic volume, respectively. LV volume and ejection fraction are precisely assessed by Simpson's method. LV volume is estimated by fitting numerous disks into the ventricle: Simpson volume = [area(1) + area(2) + … + area(n)] x length. Simpson area and length are obtained by tracing the endocardial border of the LV in the long axis and short axis view. (G) LV (left ventricular) mass. LV mass (mg) = 1.05 x [(LVIDd + LVPWd + IVSd)3 – (LVIDd)3]. The factor 1.05 represents the specific density of the myocardium. (H) HR, heart rate. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
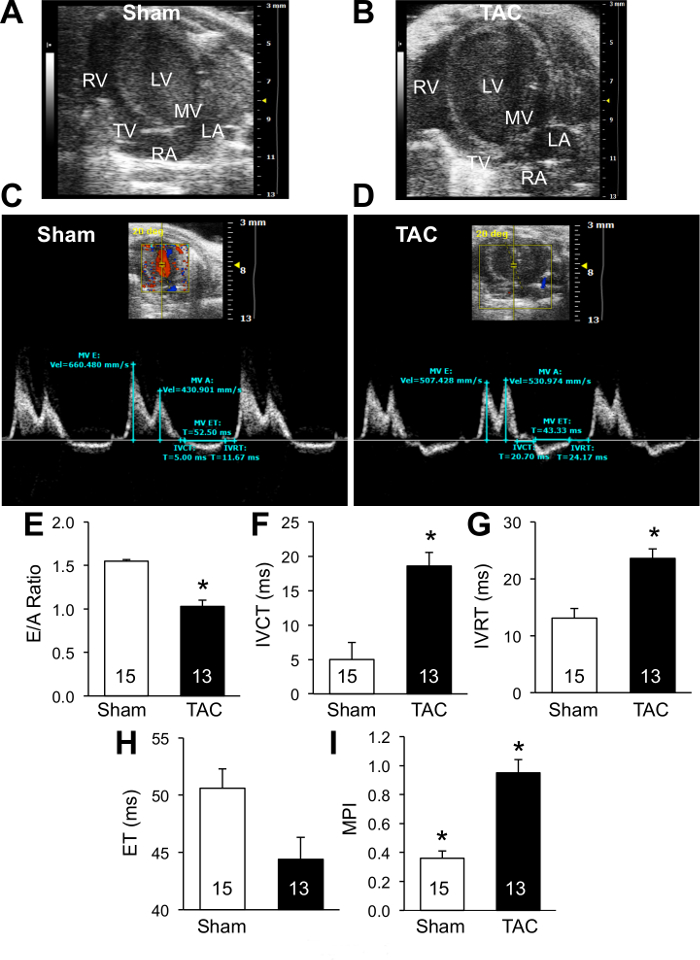
Figure 6. Assessment of Transmitral Blood Flow by Doppler Imaging. (A and B) B-mode apical four-chamber view of sham (A) or TAC (B) heart. LV, left ventricle; RV, right ventricle; MV, mitral valve; TV, tricuspid valve; LA, left atrium; RA, right atrium. (C and D) PW Doppler waveform of trans-mitral blood flow in sham (C) or TAC (D) heart. Relevant measurements are shown. (E) E/A, peak E and A velocity ratio. (F) IVCT, isovolumic contraction time. (G) IVRT, isovolumic relaxation time. (H) ET, ejection time. (I) MPI, myocardial performance index. *P <0.05 vs. Sham. The number of mice analyzed is shown in the bars of each panel. Data are expressed as mean ± s.e.m. Student's t-test was used to determine statistical significance. Please click here to view a larger version of this figure.
