The placement of the bandage on the recipient mouse is an important step of the procedure. The skin graft is positioned on the recipient trunk, between the shoulder, hip, and spine (Figure 1). The bandage is made with folded gauze and the combination of two plastic adhesive bandages. The recipient mouse is placed with the graft down over the gauze on the center of the bandage. Using two curved micro forceps, the lower end of the bandage is pulled first, and then the top of the bandage is wrapped over the mouse to the abdomen.
In complete mismatch models, full-thickness skin grafts are usually rejected in 8 to 12 days. In minor mismatch models, rejection responses are slower, more variable, and the skin graft appearance is characterized by less distinct changes, such as contraction or loss of hair (Figure 2). Acute graft rejection generally begins with swelling and erythema of the graft. These events are followed by graft desiccation, shrinkage, and scab formation (Figure 2B and C). Depending on the degree of MHC mismatch and the immunosuppression protocol, rejection can occur by a subacute process, marked by subtle changes such as loss of hair, pigmentation, dermal ridges, and graft volume. In these cases, a rejected graft appears shiny, white, and hairless, with uneven edges (Figure 2F)14.
Utilizing this model of skin transplantation, we investigated a novel approach targeting T-cell metabolism to prevent graft rejection15. It is well known that metabolic signaling pathways play critical roles in dictating the outcomes of T-cell responses16. Naive T cells rely on mitochondrial oxidative phosphorylation to generate the energy necessary for basic immune surveillance. However, upon activation, effector T cells metabolically reprogram to aerobic glycolysis and exhibit increased glutamine metabolism16,17. Using Balb/c as donors and C57BL/6 as recipients, we observed that inhibiting glycolysis and oxidative phosphorylation (2DG+metformin) or glutamine metabolism alone (DON) prolonged skin graft survival, but blocking the three pathways simultaneously resulted in significantly-increased graft survival (Figure 3C). Moreover, triple metabolic therapy was more effective than conventional cyclosporine or rapamycin (Figure 3A and B). Permanent acceptance was not achieved, and further strategies, including depletion therapy, costimulation blockade, or newer metabolic therapies, may promote better induction of transplant tolerance. However, the study provided two novel insights: the use of non-specific inhibitors to target selective immune cells with increased metabolic demands, as well as the requirement to block the three metabolic pathways simultaneously to obtain more robust immunosuppression in graft rejection.
Calcineurin inhibitors and mammalian target of rapamycin (mTOR) inhibitors constitute most of the conventional immunosuppressive therapy used in clinical transplantation. Median graft survival rates of Balb/c to C57BL/6 skin transplants treated with cyclosporine and rapamycin were 17 and 16 days, respectively. In comparison, recipients treated with metabolic inhibitors that inhibit T cell glycolysis, mitochondrial oxidative phosphorylation, and glutamine metabolism had prolonged survival: the median graft survival was 29 days. Furthermore, the histology of skin grafts from the metabolic therapy group exhibited more intact tissue alignment and less lymphocytic inflammatory infiltrate (Figure 4).
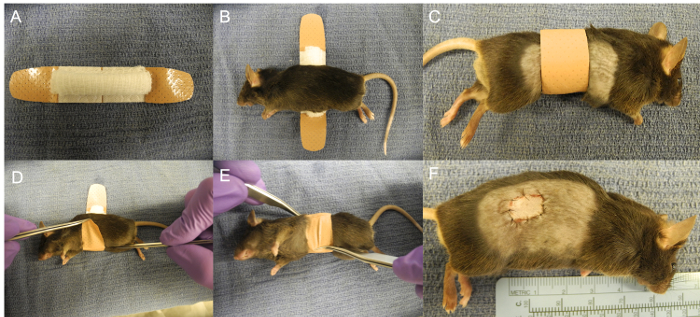
Figure 1: Covering of the Graft with the Bandage. (A) Skin graft placed on the right trunk. (B) Bandage made with a folded gauze and two plastic strips bandages. (C) Recipient mouse placed on the gauze. (D-F) Bandage wrapped around the mouse. Please click here to view a larger version of this figure.
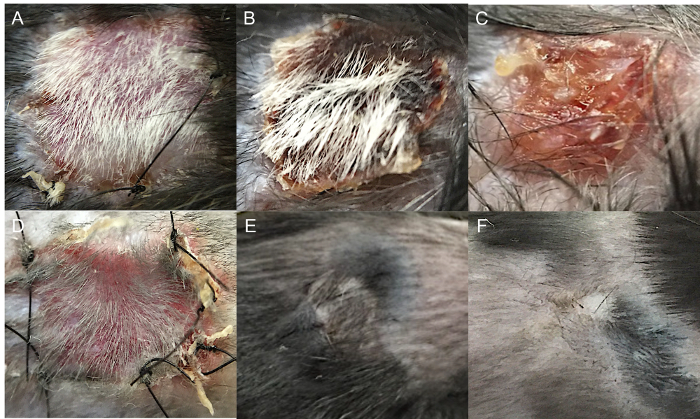
Figure 2: Skin Graft Appearance during Acute and Chronic Rejection. (A) Balb/c to C57BL/6 (complete mismatch) full-thickness skin transplantation without evidence of rejection (day 8). (B) Balb/c to C57BL/6 full-thickness skin transplantation with 50% graft rejection (day 13). (C) Balb/c to C57BL/6 full-thickness skin transplantation with complete graft rejection (day 18). (D) Syngeneic full-thickness skin transplantation (day 8). (E) Syngeneic full-thickness skin transplantation (day 30). (F) C57BL/10 to C57BL/6 (minor mismatch) full-thickness skin transplantation with chronic graft rejection (day 100). Please click here to view a larger version of this figure.
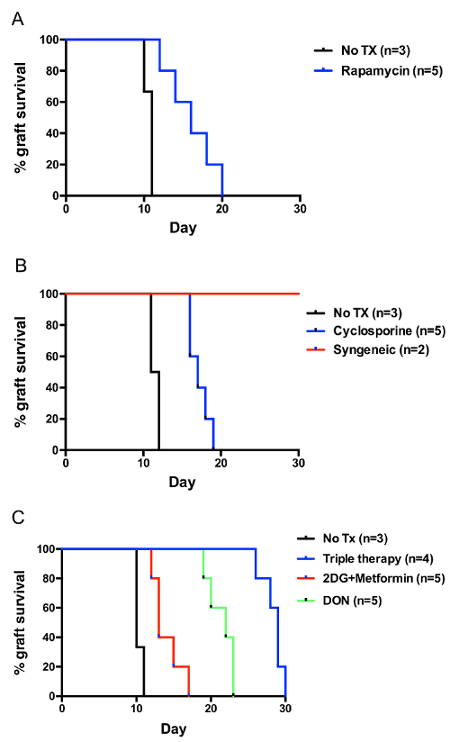
Figure 3: Balb/c to C57BL/6 Skin Graft Survival. (A) Treatment with cyclosporine (25 mg/kg QD). (B) Treatment with rapamycin (3 mg/kg QD). (C) Treatment with metabolic inhibitors, 2-Deoxy-D-glucose (2DG) 500 mg/kg QD, metformin 150 mg/kg QD, and 6-Diazo-5-oxo-L-norleucine (DON) 1.6 mg/kg QOD. All treatments were administered from the day of transplantation until rejection. Please click here to view a larger version of this figure.
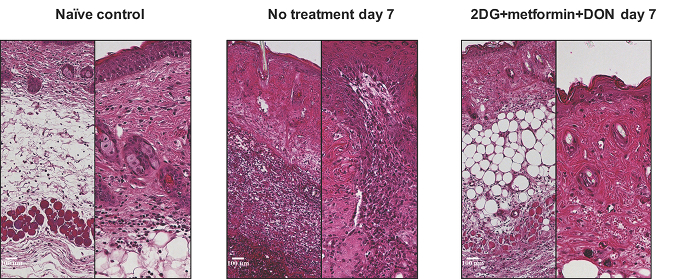
Figure 4: Hematoxylin and Eosin Stain (right, X100; left, X200) of Skin Grafts with Metabolic Therapy at Postoperative Day 7. Please click here to view a larger version of this figure.
