As subcutaneous trigeminal nerve field stimulation (sTNFS) is not a standard treatment and the number of patients that can potentially benefit from it is rather small compared to other diseases, there are only smaller case series that present results of sTNFS. In one series, 10 patients underwent test stimulation for sTNFS. Eight of the patients responded to the therapy and received permanent implantation of electrodes and an IPG11. The patients suffered from trigeminal neuralgia, trigeminal neuropathy associated with multiple sclerosis, post-herpetic trigeminal neuropathy, radiogenic trigeminal neuropathy and persistent idiopathic facial pain (Table 1). Pain was reduced from 9.3 point to 0.75 points on the VAS after 11.3 months of follow-up.
In another recently published series, 8 patients were tested with sTNFS (Figure 1). Six of the 8 patients proceeded to permanent implantation10. The patients suffered from trigeminal neuralgia with and without concomitant persistent facial pain and post-herpetic trigeminal neuropathy. Pain according to VAS was reduced from 8.5 to 1.4 points after a mean follow-up of 15.2 months. This series is also the first to describe a 73% reduction in the mean number of painful daily attacks. All but one of the patients was able to reduce or even stop all pain medication.
We provide an updated chart of all patients with permanent implantations treated at our department in Table 2. We were able to achieve a mean reduction of 6.8 VAS points (-79%; mean VAS preOP: 8.6, mean VAS postOP: 1.8) and a mean reduction in the number of daily attacks of 12.2 (-75, 3%; mean number of attacks preOP: 16.2, mean number of attacks postop: 4.0). reduction of pain medication was possible in 72.7% of patients.
The largest series published so far is comprised of 35 patients that were tested with 15 patients that received permanent implantation. Average pain reduction was 73% over a follow-up of 15 months12. However, in this series patients were treated also for conditions that do not affect the trigeminal nerve as such like temporomandibular joint (TMJ) disorders and general "headaches" that are not further specified.
In a series of 60 implanted patients a combination of subcutaneous supra- and infraorbital electrodes with occipital ones is also described as a treatment for chronic headache disorders13.
The surgical procedure is described similarly in all series however not all authors report on the duration between trials stimulation and permanent implantation.
We believe that a 4-6-week interval is crucial to reduce the number of false-positive results at the end of the test trial when patients overestimate the therapeutic effect. There is not a single parameter for outcome in pain treatment. VAS is a basic tool to subjectively quantify pain intensity. Documentation of the number of daily attacks, the amount of pain medication can help to assess outcome.
Although constant and paroxysmal pain can be both reduced by sTNFS, we observe a trend that patients with a strong neuropathic and constant pain component such as in post-herpetic trigeminal neuropathy are the most satisfied with the therapy. We lack a proper explanation for this observation as the exact mechanism of action of sTNFS is still unclear.
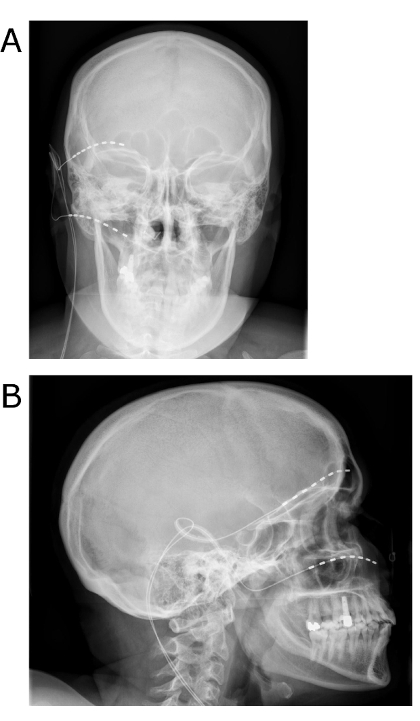
Figure 1: Postoperative x-rays after sTNFS. The patient underwent first and second trigeminal branch sTNFS for refractory trigeminal neuralgia A/P view (a) and lateral view (b). Please click here to view a larger version of this figure.
| Possible indications for sTNFS |
| trigeminal neuralgia |
| post-herpetic trigeminal neuropathy |
| multiple sclerosis associated trigeminal neuropathy |
| radiogenic triogeminal neuropathy |
| persistent idiopathic facial pain |
Table 1: Possible indications for sTNFS as reported in the literature. In all cases the pain should be chronic and be refractory to standard treatment before applying sTNFS.
| Effects of sTNFS | ||||||||
| # | age/sex | Disorder | Affected Branches | VAS preOP | VAS last Follow-Up | Daily attacks preOP | Daily attacks last Follow-Up | Redution of pain medication |
| 1 | 27/f | Postherpertic Neuropathy | V1 & V2 , right | 8 out of 10 | 2 out of 10 | 10 | 2 | yes |
| 2 | 34/f | Classical Trigeminal Neuralgia | V1 & V2, left | 10 out of 10 | 2 out of 10 | 3 | 1 | yes |
| 3 | 25/f | Classical Trigeminal Neuralgia | V1 & V2 , right | 8 out of 10 | 1 out of 10 | 30 | 2 | yes |
| 4 | 77/m | Classical trigeminal Neuralgia | V1 & V2, right | 10 out of 10 | 1 out of 10 | 50 | 2 | no |
| 5 | 81/f | Postherpertic Neuropathy | V1, right | 8 out of 10 | 1 out of 10 | 20 | 10 | yes |
| 6 | 80/f | Classical Trigeminal Neuralgia | V1 & V2 , right | 8 out of 10 | 1 out of 10 | 10 | 1 | yes |
| 7 | 52/m | Classical Trigeminal Neuralgia | V2 & V3, right | 10 out of 10 | 5 out of 10 | 10 | 2 | no |
| 8 | 66/f | MS associated Neuropathy | V2 & V3, left | 8 out of 10 | 1 out of 10 | 15 | 1 | yes |
| 9 | 78/f | Postherpetic Neuropathy | V1, right | 5 out of 10 | 2 out of 10 | 5 | 1 | no |
| 10 | 60/f | MS associated Neuropathy | V2 & V3, right | 10 out of 10 | 1 out of 10 | 10 | 2 | yes |
| 11 | 38/m | Classical Trigeminal Neuralgia | V2 & V3, right | 10 out of 10 | 3 out of 10 | 15 | 2 | yes |
Table 2: Results of sTNFS on reduction of pain intensity and attack frequency for different etiologies of trigeminal pain.
