Uncontrolled Hemorrhagic Shock Modeled via Liver Laceration in Mice with Real Time Hemodynamic Monitoring
Summary
Uncontrolled hemorrhage, an important cause of mortality among trauma patients, can be modeled using a standard liver laceration in a murine model. This model results in consistent blood loss, survival, and allows for testing hemostatic agents. This article provides the step-by-step process to perform this valuable model.
Abstract
Uncontrolled hemorrhage is an important cause of preventable deaths among trauma patients. We have developed a murine model of uncontrolled hemorrhage via a liver laceration that results in consistent blood loss, hemodynamic alterations, and survival.
Mice undergo a standardized resection of the left-middle lobe of the liver. They are allowed to bleed without mechanical intervention. Hemostatic agents can be administered as pre-treatment or rescue therapy depending on the interest of the investigator. During the time of hemorrhage, real-time hemodynamic monitoring via a left femoral arterial line is performed. Mice are then sacrificed, blood loss is quantified, blood is collected for further analysis, and organs are harvested for analysis of injury. Experimental design is described to allow for simultaneous testing of multiple animals.
Liver hemorrhage as a model of uncontrolled hemorrhage exists in the literature, primarily in rat and porcine models. Some of these models utilize hemodynamic monitoring or quantify blood loss but lack consistency. The present model incorporates quantification of blood loss, real-time hemodynamic monitoring in a murine model that offers the advantage of using transgenic lines and a high-throughput mechanism to further investigate the pathophysiologic mechanisms in uncontrolled hemorrhage.
Introduction
Trauma is the leading cause of death and disability among young people worldwide.1 Uncontrolled hemorrhage remains a leading cause of mortality among severely injured trauma patients.2 Management of the hemorrhaging trauma patient is two-fold: control of surgical bleeding, and resuscitation and replacement of lost blood.
Animal models of hemorrhagic shock have been the cornerstone in trauma research and can be used in the evaluation of the pathophysiology and treatment of traumatic/hemorrhagic shock.3,4 Shock in animal models can be achieved broadly by two methods: controlled-hemorrhage and uncontrolled-hemorrhage.5,6 Controlled-hemorrhage is performed by removal of a fixed volume of blood or by blood removal to achieve a certain blood pressure (fixed-pressure). While these models are useful in the evaluation in the mechanisms and immune alterations in hemorrhagic shock, they are not applicable to the testing of hemostatic agents and do not mimic the clinical scenario of hemorrhage following trauma. To this degree, we sought to develop a model of uncontrolled hemorrhage that would allow us to test hemostatic changes and pro-coagulant agents in a murine model. The liver is an attractive option for uncontrolled hemorrhage in part because of the dual blood supply to the liver and it is one of the most commonly injured intrabdominal organs in both blunt and penetrating trauma. Given the high clinical relevance, the liver has been utilized as a model of uncontrolled hemorrhage, most commonly in rat and porcine models but recently in primates as well.7,8,9,10,11,12 Murine models have also incorporated liver injury, such as a crush model or blunt trauma; however, these models do not result in hemorrhagic shock secondary to the liver injury.13,14
The rat and porcine models of uncontrolled liver hemorrhage, while valuable in looking at resuscitation practices and hemodynamic monitoring, are less advantageous than a murine model for various reasons such as cost, number of animals utilized, and importantly the relative lack transgenic lines available for analysis of specific cellular and molecular signaling. The present murine model shares important similarities to existing liver hemorrhage models including standardized liver laceration, blood loss quantification, hemodynamic monitoring, and the ability to perform survival analysis. Many existing models only incorporate some of these aspects whereas our model was developed to measure many of the physiologic variables simultaneously and in multiple mice. As well, development of a murine model opens the door to investigations beyond resuscitation and into greater pathophysiology mechanisms in uncontrolled hemorrhage with the potential of a cost efficient, high-throughput model using advanced molecular techniques.
Protocol
Mice were housed in accordance with University of Pittsburgh (Pittsburgh, PA, USA) and National Institutes of Health (NIH; Bethesda, MD, USA) animal care guidelines in specific pathogen-free conditions with 12 h light-dark cycles and free access to standard feed and water. All animal experiments were approved and conducted in accordance with the guidelines set forth by the Animal Research and Care Committee at the University of Pittsburgh.
1. Surgical Field and Instrument Setup
- Sterilize all surgical instruments, suture, gauze, cotton tip applicators, tubing, and tubing connectors prior to the procedure.
- Sterilize surgical instruments, suture, gauze, and cotton tip applicators in an autoclave. Sterilize tubing and tubing connectors with ethylene oxide.
- Surgical field
- Turn on a water-circulating heating pad and set to 37 °C. Place a surgical blue pad on top of it and then a sterile drape on top of the surgical blue pad.
- Open all sterilized instruments onto the sterile drape. Use sterile gloves to avoid breaking sterility during this step.
- Fill a stainless steel bowl with 70% ethanol and set aside. This will be used to clean instruments between animals.
- Turn on microbead sterilizer and allow to heat to 150 °C. This will also be used to clean instruments between animals. If performing surgery on more than 5 mice, be sure to change instruments to a new sterile set.
- Transducer Set-up
- Connect a sterile transducer, PE-50 tubing, two 23G needles, and male-male luer, and a three-way stopcock.6
- Calibrate and zero the transducer per manufacturer instructions.
2. Liver Laceration Surgical Procedure
- Anesthesia Induction and Positioning
- Inject sodium pentobarbital intraperitoneally at dose of 70 mg/kg. Anesthesia should take effect between 5-10 min; assess depth of anesthesia with a toe pinch. If the mouse has response to the toe pinch, additional time or anesthesia is needed. If additional anesthesia is needed during the procedure, supplement sodium pentobarbital. Do not give supplements in larger quantities than 0.05 mL to prevent overdose.
- After the mouse is completely under anesthesia, position the mouse supine on a surgical board. Secure all four limbs of the mouse to the board with tape.
- Shave the abdomen and bilateral groins with a razor.
- Soak sterile gauze with betadine and apply to the abdomen and bilateral groins for surgery. For survival experiments, prep the abdomen and groins with betadine followed by ethanol for a total of three prep cycles.
- Insert a rectal temperature probe to monitor core temperature throughout the procedure. Keep the core temperature between 35-37 °C.
- Femoral artery and venous cannulation
- For venous catheter set-up: fill PE-10 tubing, a 30 G needle, and a three-way stopcock with Lactated Ringer's solution from an IV bag.
- For arterial catheter set-up: fill PE-10 tubing and 30G needle with heparinized saline (1:10 dilution of 1,000 U heparin). Heparin-saline is required to prevent clotting.
- Place the mouse under a dissecting microscope.
- Make a 4-5 mm longitudinal incision over the groin muscle using surgical Iris scissors. Using Dumont forceps grab the adipose tissue connected to the adductor muscle and pull laterally for a clean exposure of the femoral bundle. Do not dissect through the adipose tissue as this will lead to vascular injury.
- Carefully dissect the nerve away from the artery and vein with the Dumont forceps. There is a fat pad adjacent to the nerve. Grab this with one Dumont forcep and pull laterally; this pulls the nerve away from the artery creating a plane for dissection. With other Dumont forcep bluntly dissect the connective tissue between the nerve and the artery.
- Do not grab the nerve during this part of the dissection.
- Loop three 6-0 silk sutures around the artery and vein proximal to the profunda femoris take off.
- Place suture 1 most proximally and leave loose.
- Place suture 2 most distally and tie immediately.
- Place suture 3 between Suture 1 and 2 and leave loose.
- Make an arteriotomy on the ventral surface of the vessel. Use of microvascular scissors is recommended to make the arteriotomy to avoid transection of the vessel.
- Insert the three-way catheter into the artery. Immediately tie off Suture 1 and 2 to secure the catheter in place.
- Connect the three-way catheter to the transducer and collect baseline blood pressure data.
- Repeat steps 2.2.4 – 2.2.6 on the opposite groin. Cannulate the femoral vein in a similar manner to the artery. Perform a venotomy on the ventral surface of the vessel followed by catheter insertion. This catheter can be utilized for fluid or drug administration.
- Liver Laceration
- Pre-weigh a tube containing 0.5 mL of PBS, three absorption triangles, and one weigh boat per mouse.
- Make a ventral midline laparotomy incision starting at the xiphoid process and extending caudally to allow exposure of the liver completely.
- Insert one absorption triangle in the abdomen against the right abdominal wall. Repeat on the left side.
- Make sure the absorption triangle is away from the liver to avoid a packing hemostatic effect after the liver is lacerated.
- Carefully grab the left-middle lobe of the liver and lacerate 75% of the lobe with surgical Iris scissors. Place the lacerated segment in a tube containing PBS.
- Close the abdominal wall with staples via a staple applicator. Grasp the skin and muscle together and fire the staple. Do this as quickly as possible after the liver laceration to avoid blood loss outside of the abdomen. In survival experiments, the abdomen is closed in two layers. A running absorbable suture for the muscle followed by a running layer of non-absorbable suture for the skin provides adequate closure.
- For mice that are for survival timepoints longer than 30 min the femoral catheters should be removed, the artery and vein tied with suture 3 from step 2.2.6. Bilateral groins are then closed in two layers as described in the previous step.
- Following a specified time of interest for hemorrhage (30 min up to 72 h), remove the staples. Remove the absorption triangles and put into corresponding pre-weighed weigh boats. Use additional absorption triangles to soak up any unabsorbed blood.
- Weigh absorption filters to calculate total blood loss.
- Post-operative Care
- Leave mice that are to be sacrificed at 30 min on the surgical board and under constant monitoring and under full anesthesia until the time of sacrifice. Mice are euthanized with a combination of cardiac puncture and an overdose of inhaled isoflurane.
- Place mice that are for longer survival time points in a recovery cage on top of a water-circulating heating pad. Constantly monitor the mice during recovery and do not leave unattended until they regain consciousness to maintain sternal recumbency. Return the mouse to cage space with other mice only once it has recovered from anesthesia.
- Administer post-operative analgesia with 0.1 mg/kg buprenex via subcutaneous injection once awoken from anesthesia and every 12 h after until the time of sacrifice.
- Allow mice free access to food and water after they are returned to their normal cages post-operatively.
- At the time of sacrifice for survival mice, anesthesia is accomplished with inhaled isoflurane. Once under anesthesia blood is collected via a right heart cardiac puncture, blood loss is recorded as described above and finally euthanasia is insured with an overdose of isoflurane.
Representative Results
The liver laceration model results in reproducible and consistent blood loss in mice. Figure 1A demonstrates the consistent weight of lacerated liver that can be obtained with a standard deviation of only 0.02 g. This consistency in lacerated liver weight allows the ability to reproduce the model between mice and in different experimental set-ups such as different resuscitative protocols. As well, the reproducible weight of the lacerated liver, with a standard error of only 0.01 g provides a more standard model for uncontrolled hemorrhage that is often difficult to obtain in animal models.
Validation of the bleeding effects of different treatment protocols in the model are demonstrated in Figure 1B. Mice were pre-treated with heparin (66 units, as a positive control for blood loss), or the anti-fibrinolytic, tranexamic acid (TXA) (as a negative control), and a validated pro-hemostatic nanoparticle previously tested in murine tail vein bleeding assays.15 These results demonstrate the ability of this model to be used to assess the hemostatic or anticoagulant effects in the setting of hemorrhage.
Uncontrolled hemorrhage is often accompanied by hemodynamic derangements that are important to monitor. In Figure 2 the mean arterial blood pressure (MAP) of individual mice following liver laceration demonstrates that precipitous and reproducible drop in MAP after the laceration is performed resulting in a hemorrhagic shock state. This is important as it allows the hemodynamic effects of different resuscitative or interventional measures and allows for important insight into the physiology surrounding various experimental conditions. While there are significant hemodynamic effects following the liver laceration we have found that the model can be used to evaluate survival effects as the model has been evaluated out to 72 h with a survival of 56% at this time point (Figure 3).
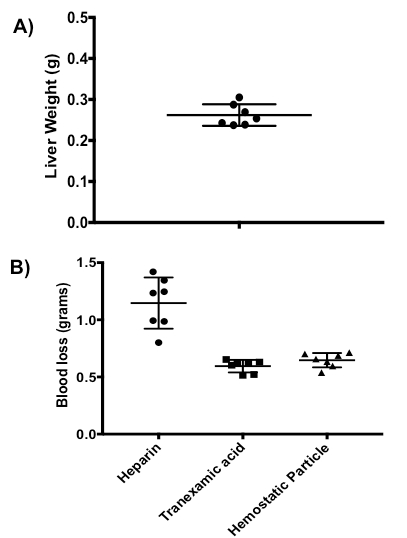
Figure 1: Liver Laceration Validation. (A) Representative weights of the transected liver. The mean liver weight was 0.26 g with a standard deviation of 0.02 g and a standard error of the mean of 0.01 g. These results demonstrate the consistency that can be obtained with visual estimation of our 75% laceration. (B) Blood loss in grams following pre-treatment with heparin, tranexamic acid, and a previously validated hemostatic nanoparticle Mean blood loss was 1.6, 0.60, and 0.65 g respectively. These results validate the utility of this model to test the hemostatic or anticoagulant effects of a drug.

Figure 2: Mean Arterial Blood Pressure following Liver Laceration. Graphical tracings of individual mice mean arterial blood tracings over 20 min who either underwent a sham operation or liver laceration. The liver laceration is followed by a characteristic and precipitous drop in the mean arterial blood pressure (MAP) of the mice that is absent in sham operated mice.
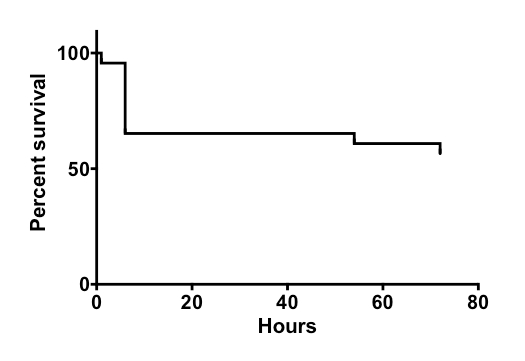
Figure 3: Kaplan-Meier Survival Curve following Liver Laceration. The 72 h survival in mice that underwent the liver laceration without any treatment was found to be 56%.
Discussion
The murine liver laceration model described here provides a reliable, consistent model of uncontrolled hemorrhage. This model is straightforward to perform but there are important steps that require meticulous consideration. The most technically challenging part of the model is cannulation of the femoral vessels for hemodynamic monitoring and fluid/drug administration. Care must be taken during the dissection of the nerve and the arteriotomy/venotomy. It is important to not touch the nerve during the dissection of the vessels to avoid resulting nerve damage and possible paralysis, especially for survival models. The arteriotomy and venotomy require delicate handling of the vessel. We suggest use of microvascular scissors to prevent accidental transection of the vessel.
While the liver laceration is less technically challenging it is important to be consistent in the part of the model to ensure reproducible and consistent hemorrhage in the mouse. Our model was developed with the intent of testing pro hemostatic agents in resuscitation and therefore an important placement consideration includes ensuring the absorption triangles are placed away from the laceration site to avoid a packing or mechanical hemostatic effect. Avoid unnecessary manipulation of other organs and other lobes of the liver to prevent unintentional injury or bleeding during this part of the surgery. The abdomen should be quickly closed following the laceration to avoid blood loss outside the abdomen.
The mice should be monitored closely throughout the procedure but most importantly after the laceration is performed given the significant hemodynamic changes they experience as we demonstrated in Figure 2. Our experience with these significant hemodynamic changes is that the mouse is unlikely to survive if their MAP drops below 10mmHg for > 30 s and we recommend sacrifice of the mouse in which this occurs. If a fluid or drug is to be tested for its hemostatic effects we recommend administration soon after the laceration, as the mice tend to clot the lacerated area quickly. Use of pain management is essential if interested in performing longer observation time-points than described here. As well, the hind limbs should be monitored for signs of ischemia following ligation of the femoral vessels. Due to the extensive experience with these surgical procedures, the incidence of this complication in our lab is less than 1% of all animals tested.4,6
This model has a number of important limitations, including the aspect of uncontrolled hemorrhage. While we see consistent hemorrhage in mice in terms of blood loss some mice respond differently and will die quickly following the laceration. Another limitation in the model is the size of the liver laceration. While our data demonstrates a narrow standard error in the weight of the resected liver, when performed by different individuals the possibility for greater variability in resection size and therefore hemorrhage certainly exists. Additionally, the learning curve for the microvascular dissection and cannulation can be technically challenging, and we estimate a learning curve of 50 animals from our experience, with an estimated learning curve of 10 mice for reproducibility of the liver laceration as described. From our experience a survival of 56% at 72 h can be expected. When performing the model for survival analysis close attention to recovery from anesthesia and proper pain management are crucial. In our current model, we have not performed any supplemental fluid or drug resuscitation to the mice beyond what they receive prior to liver laceration. It is important to note that animals should be monitored closely for signs of distress in the survival portion of the model and treated appropriately for pain. Pentobarbital is our anesthetic of choice for the time points we were interested in but other choices of anesthesia are possible and may affect results. Pain control is important to monitor so that the mice are able to freely eat and drink, which if not controlled can lead to variability outside of the hemorrhage and treatment of interest. This model also lends itself to be combined with other models such a soft tissue injury, pseudofracture, or a polytrauma model. As well, this model could easily be adapted to study the effects of topical hemostatic agents compared to intravenous. Multiple alternative modifications of this model are possible but remain untested. Although animals in this model were matched for age and weight, it is possible that animals of different weights could be utilized and the size of the liver laceration chosen based on weight. Similar results may be expected from splenic laceration for investigators who may not want to injure the liver depending on endpoint of interests. Similar uncontrolled hemorrhage models have been used in other animals7,8,9,10,11,12 providing potential alternative modifications to the present model. Finally, the size of the laceration can be increased to maximize blood loss, however, we have found that this substantially increases mortality and that damage to main hepatic veins with extended models have a higher degree of variability.
The liver has been used in prior uncontrolled models; however, most of these models were performed in a rat model. Our development of an uncontrolled liver laceration model in mice allows investigators to take advantage of the wealth of genetically modified breeds. Other advantages of murine models include the ability to perform high-throughput testing, cost-effectiveness, and ease of handling. Our model allows hemodynamic monitoring, quantification of blood loss, and evaluation of mortality which prior studies often only include one of these aspects of evaluation. We are able to perform this model on multiple mice simultaneously allowing not only high-throughput but decreased variability in the model.
In conclusion, we present here a reproducible model of uncontrolled hemorrhage utilizing a standard liver laceration in a murine model. Our model is ideal for evaluating new hemostatic drugs in the setting of hemorrhage or trauma and can be utilized in a short-term evaluation of blood loss or carried out to evaluate survival effects.
Divulgations
The authors have nothing to disclose.
Acknowledgements
The work of this manuscript was supported by funding to Dr. Neal by the Vascular Medicine Institute Pilot Project Program in Hemostasis and Vascular Biology (P3HVB) and the AAST Research Fellowship. This work is supported by U.S. National Institutes of Health grants 1 R35 GM119526-01 and UM1HL120877-01.
Materials
| SS/45 dumonts | Fine Science Tools | 11203-25 |
| surgical scissors | Fine Science Tools | 14068-12 |
| hemostats | Fine Science Tools | 13009-12 |
| microscissors | Fine Science Tools | 15000-08 |
| 0.8mm curved forceps | Fine Science Tools | 11009-13 |
| suture reel 6-0 | Fine Science Tools | 18020-60 |
| suture 4-0 silk w/ needle | Owens Minor | K188H |
| gauze 4×4 | can be purchased through any global vendor | |
| cotton-tip applicator | can be purchased through any global vendor | |
| 30G needle | can be purchased through any global vendor | |
| 23G needle | can be purchased through any global vendor | |
| 10cc syringe | can be purchased through any global vendor | |
| 50cc conical tube | can be purchased through any global vendor | |
| 1cc syringe w/ 25G needle | Fisher Scientific | 14-826-88 |
| Polyethylene 10 tubing 100`(PE-10) | Fisher Scientific | 14-170-12P |
| Polyethylene 50 tubing 100`(PE-50) | Fisher Scientific | 14-170-12B |
| 3-way stopcock | Fisher Scientific | NC9779127 |
| surgical blue pad | Fisher Scientific | 50-7105 |
| Sterile Field dressings | Fisher Scientific | NC9517505 |
| tape rolls 1" | Corporate Express | MMM26001 |
| straight side wide mouth jars | VWR | 159000-058 |
| stainless steel tray 8" x 11" | VWR | 62687-049 |
| male-male leur lock 3-way | VWR | 20068-909 |
| sterilization pouch 3"x8" | VWR | 24008 |
| sterilization pouch 5"x10" | VWR | 24010 |
| absorption triangles | Fine Science Tools | 18105-03 |
| 7mm wound clip applier | Fisher Scientific | E0522687 |
| 1000 7mm wound clips | Fisher Scientific | E0522687 |
| betadine (4oz) | can be purchased through any global vendor | |
| sterile gloves | can be purchased through any global vendor | |
| eppendorfs | can be purchased through any global vendor | |
| 1/2cc Lo-Dose insulin syringe | Fisher Scientific | 12-826-79 |
| small weigh boat | can be purchased through any global vendor | |
| lactated ringers | can be purchased through any global vendor | |
| hepranized saline solution (.1µ hep + 9.9µNaCl) | can be purchased through any global vendor | |
| phosphate buffered saline | can be purchased through any global vendor | |
| pentobarbital | can be purchased through any global vendor | |
| Wild M650 microscope w/ boom stand | Leica | |
| Digi-Med BPA-400 analyzer & systems integrator | Micro-Med | SYS-400 |
| TXD-310 (Digi-Med Transducer) | Micro-Med | TXD-300 |
| Computer | Dell | |
| microbead instrument sterilizer | VWR | 11156-002 |
| Oster A5 clippers w. size 40 blade | VWR | 10749-020 |
| circulating heating pad 18×26 | Harvard | py872-5272 |
| rectal thermometer | Kent Scientific | RET-3 |
References
- Chang, R., Cardenas, J. C., Wade, C. E., Holcomb, J. B. Advances in the understanding of trauma-induced coagulopathy. Blood. 128 (8), 1043-1049 (2016).
- Kutcher, M. E., et al. A paradigm shift in trauma resuscitation: evaluation of evolving massive transfusion practices. JAMA surgery. 148 (9), 834-840 (2013).
- Tsukamoto, T., Pape, H. C. Animal Models for Trauma Research. Shock. 31 (1), 3-10 (2009).
- Darwiche, S. S., et al. Pseudofracture: an acute peripheral tissue trauma model. J Vis Exp. (50), (2011).
- Lomas-Niera, J. L., Perl, M., Chung, C. -. S., Ayala, A. Shock and Hemorrhage: an Overview of Animal Models. Shock. 24, 33-39 (2005).
- Kohut, L. K., Darwiche, S. S., Brumfield, J. M., Frank, A. M., Billiar, T. R. Fixed volume or fixed pressure: a murine model of hemorrhagic shock. J Vis Exp. (52), (2011).
- Matsuoka, T., Hildreth, J., Wisner, D. H. Liver injury as a model of uncontrolled hemorrhagic shock: resuscitation with different hypertonic regimens. J Trauma. 39 (4), 674-680 (1995).
- Komachi, T., et al. Adhesive and Robust Multilayered Poly(lactic acid) Nanosheets for Hemostatic Dressing in Liver Injury Model. J. Biomed. Mater. Res. Part B Appl. Biomater. , (2016).
- Orfanos, N. F., et al. The effects of antioxidants on a porcine model of liver hemorrhage. J Trauma Acute Care Surg. 80 (6), 964-971 (2016).
- Morgan, C. E., Prakash, V. S., Vercammen, J. M., Pritts, T., Kibbe, M. R. Development and validation of 4 different rat models of uncontrolled hemorrhage. JAMA Surgery. 150 (4), 316-324 (2015).
- Rosselli, D. D., Brainard, B. M., Schmiedt, C. W. Efficacy of a topical bovine-derived thrombin solution as a hemostatic agent in a rodent model of hepatic injury. Can J Vet Res. 14 (14), 303-308 (2015).
- Sheppard, F. R., et al. Development of a Nonhuman Primate (Rhesus Macaque) Model of Uncontrolled Traumatic Liver Hemorrhage. Shock. 44, 114-122 (2015).
- Nemzek-Hamlin, J. A., Hwang, H., Hampel, J. A., Yu, B., Raghavendran, K. Development of a murine model of blunt hepatic trauma. Comp Med. 63 (5), 398-408 (2013).
- Vogel, S., et al. Platelet-derived HMGB1 is a critical mediator of thrombosis. J Clin Invest. 125 (12), (2015).
- Modery-Pawlowski, C. L., Tian, L. L., Ravikumar, M., Wong, T. L., Sen Gupta, A. In vitro and in vivo hemostatic capabilities of a functionally integrated platelet-mimetic liposomal nanoconstruct. Biomaterials. 34 (12), 3031-3041 (2013).
