The success of applying reverse genetic tools and techniques to malaria parasites has revolutionized the field of malaria research, with the ability to add, delete, or modify specific genomic segments of several Plasmodium species39. Importantly, dispensable genomic loci have been identified and used successfully to introduce fluorescence protein markers in rodent and human malaria parasites by double homologous recombination, to ensure a stable expression in all life cycle stages40,41,42. An example of these WT-like transgenic parasites is Py230p(-) parasites, which have been generated in our lab, and showed no apparent defect in the development of blood and mosquito life cycle stages15,16,17. These transgenic reporter parasites expressed eGFP, under the control of the strong and constitutive promoter of PyHSP70, in blood stages (Figure 1A) ookinetes (Figure 1B), young oocysts (Figure 1C) on Anopheles stephensi midguts, and in sporozoites isolated from the salivary glands of Anopheles stephensi females (Figure 1D). Thus, the eGFP-expressing blood parasites made it much easier and less time-consuming to evaluate blood-stage parasitemia using flow cytometry between different genotypes of transgenic parasites or between drug-treated and -untreated in drug-targeting assays using transgenic reporter parasites.
In order to confirm that there is no quantitative difference between the use of flow cytometry and the more tedious parasitemia estimation by microscopy, the eGFP-expressing Pyp230p(-) was used to estimate the percentage of parasitized erythrocytes by flow cytometry and by Giemsa-stained thin blood smear in a group of Swiss Webster mice IV-infected with 10,000 parasitized erythrocytes. The flow cytometry parasitemia% values corresponded directly to the estimated parasitemia% by monitoring Giemsa-stained thin blood smears, which were estimated by two expert scientists (Figure 2). This represents a more accurate alternative to the tedious and prone-to-human-error method of microscopy in the determination of the growth rate of blood-stage parasites.
An important discrepancy associated with the infection of rodents with malaria parasites blood stages is the choice of route of infection, with a strong preference in the literature for the IP compared to IV route of infection, as it is less time-consuming. In order to compare these two routes of infection, two groups of five BALB/c mice were infected with 1,000 eGFP-expressing Pyp230p(-) parasitized erythrocytes per mouse, either through IV or IP routes. The parasitemia was monitored daily using flow cytometry for a period of 4 days. A statistically significant decrease in the IP-infected group parasitemia% compared to the IV-infected group was noted on all days tested (Figure 3). This provides evidence that the IV infection route is a more quantitatively accurate route of infection for assays with the malaria parasite blood stages.
Nonetheless, one limitation to the use of flow cytometry to evaluate blood-stage parasitemia is the differentiation between sexual and asexual stages and between male and female gametocytes. Therefore, the estimation of the percentages of each of the different asexual and sexual stages (Figure 4) has to depend on a morphology evaluation of Giemsa-stained thin blood smear. Despite the apparent different morphology of mature male and female gametocytes (Figure 4), immature sexual stages are often indistinguishable from asexual stages.
One essential function of the male gametes upon emergence from male gametocyte in the mosquito midgut is the male gamete exflagellation, which is a very critical step in the transmission that must happen within a very short period of time. Variable methods used to evaluate this in many different systems have been described. Herein, we show a standardized method that can be repeated in any simple lab setting. We evaluated male gamete exflagellation with or without the injection of phenylhydrazine into recipient mice (Figure 5). We could show that the phenylhydrazine treatment significantly (four fold) increased the rate of male gamete exflagellation, which in turn will increase the fertilization rate and the number of all subsequent mosquito stages.
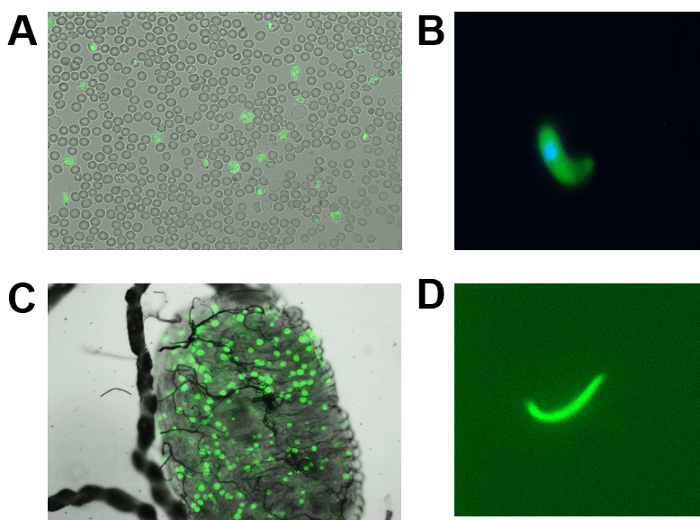
Figure 1: The development of P. yoelii p230p(-) parasites constitutively expressing eGFP in blood and mosquito stages. (A) Image of mixed blood-stage parasites (1,000X magnification). (B) Image of ookinete (400X magnification). (C) Image of an Anopheles stephensi mosquito midgut infected with day 4 pmf early oocysts of live p230p(-) parasites expressing eGFP (100X magnification). (D) This panel shows a live image of a P. yoelii p230p(-) salivary gland sporozoite, dissected out at day 15 pmf, expressing eGFP (400X magnification). Please click here to view a larger version of this figure.
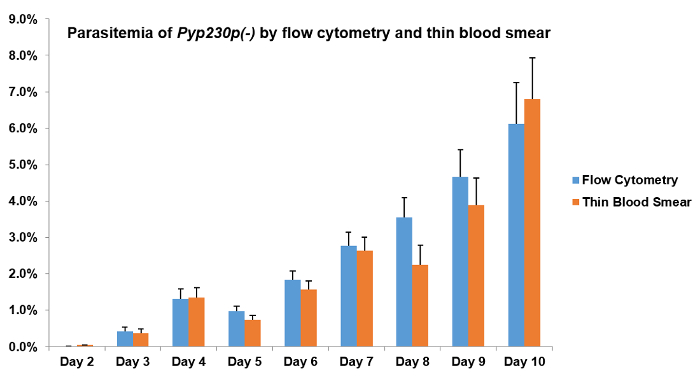
Figure 2: Flow cytometry and microscopy evaluations of average blood-stage parasitemia of P. yoelii p230p(-) parasites are not significantly different. A group of four Swiss Webster mice was intravenously infected with 10,000 parasitized erythrocytes of Pyp230p(-) per mouse and the average blood-stage parasitemias% were recorded daily for 7 days by flow cytometry and by the microscopic evaluation of Giemsa-stained thin blood smears from a total of 20,000 and ~6,000 erythrocytes, respectively. The microscopic examination results shown are the average of two readings by two expert scientists per slide, and the time for evaluating the parasitemia of each slide was at least 10 minutes by each scientist. No significant differences could be detected on any of the days shown here. The mean values for all parasite strains were analyzed with the two-tailed t-test. The error bars represent the standard deviation. Please click here to view a larger version of this figure.
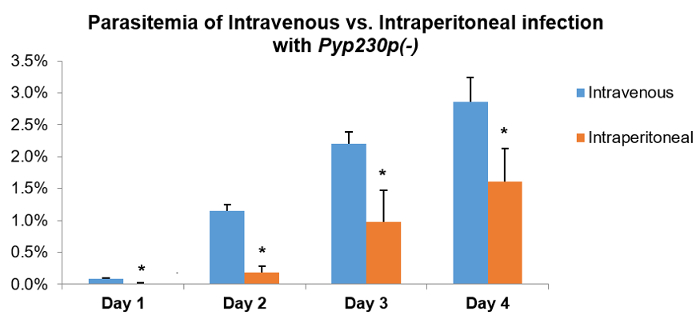
Figure 3: An intravenous injection of P. yoelii p230p(-) parasites yields significantly different blood-stage parasitemia from an intraperitoneal injection. Two groups of five BALB/c mice were infected with 1,000 parasitized erythrocytes of Pyp230p(-) per mouse, either through the intravenous or intraperitoneal route, and the average blood-stage parasitemias% were recorded daily for 4 days by flow cytometry from a total of 20,000 erythrocytes. A statistically significant reduction (denoted by an asterisk) of blood-stage parasitemia could be detected for all days tested in the intraperitoneal route group compared to the intravenous route group. The mean values for all parasite strains were analyzed with the two-tailed t-test. The error bars represent the standard deviation. Please click here to view a larger version of this figure.
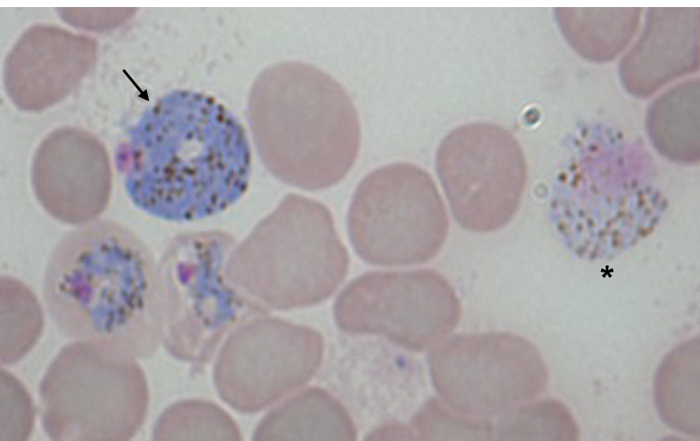
Figure 4: Morphology of P. yoelii gametocytes in a Giemsa-stained thin blood smear. An image of a Giemsa-stained thin blood smear (1,000X magnification) of a Swiss Webster mouse infected with WT P. yoelii 17X-NL strain shows the typical blueish colored female gametocyte on the left side (denoted by an arrow) and the pinkish colored male (denoted by an asterisk) gametocyte on the right side of the image. The other stages shown are asexual blood stages. Please click here to view a larger version of this figure.
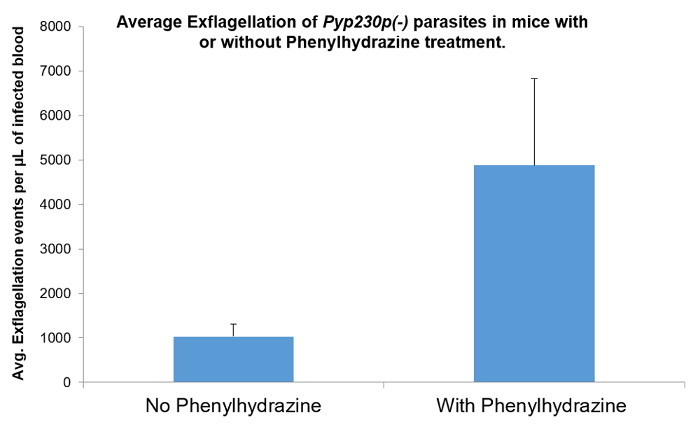
Figure 5: The effect of phenylhydrazine on male gamete exflagellation. The effect of phenylhydrazine injected in recipient mice 5 days prior to the male gamete exflagellation rate estimation of P. yoelii. Phenylhydrazine significantly increases the rate of male gamete exflagellation, which leads to a higher mosquito stages infection post-mosquito-feeding. The mean values for all parasite strains were analyzed with the two-tailed t-test. The error bars represent the standard deviation. Please click here to view a larger version of this figure.
