Potent Transgene Expression in Subpially AAV9-injected Segments:
The analysis of transgene (GFP) expression in spinal cord sections at 14 days after AAV9 delivery showed AAV9-dose dependent GFP expression throughout the spinal parenchyma. First, two bilateral 3 µL injections of AAV9-UBI-GFP injected into the upper lumbar subpial space were associated with the near-complete infection of the white and gray matter in the whole lumbar spinal cord, extending to the upper thoracic segments (Figure 2A and 2B, left and middle columns). Two bilateral 1.5 µL injections of AAV9-UBI-GFP into the upper lumbar subpial space were associated with a similar near-complete infection of the white and gray matter in the whole lumbar spinal cord (as seen after injections of 3 µL); however, the mid-thoracic segments showed only occasionally infected neurons (Figure 2B, right column). Staining with α-motoneuron-specific (ChAT) and neuron-specific (NeuN) antibodies showed consistent GFP expression in the entire population of lumbar α-motoneurons (Figure 2C) and interneurons localized in the dorsal horn (Figure 2D), intermediate zone (Figure 2E), and ventral horn (Figure 2F). Second, two bilateral cervical injections of AAV9 (5 µL for each injection) led to similar GFP expression in the white and gray matter in the whole cervical spinal cord (gray and white matter) and in the upper thoracic segments (Figure 3A and 3B). Analysis of lumbar spinal cord sections in the same animals showed a high density of GFP+ descending axons terminating in the vicinity of the lumbar GFP-negative α-motoneurons and interneurons (Figure 3C and 3D). The delivery of two bilateral cervical and two bilateral upper lumbar injections of AAV9 (5 µL for each injection) was associated with GFP expression in the entire spinal cord, from the upper cervical to sacral segments, and was homogenously present in the white and gray matter (Figure 3E-3H).
Retrograde and Anterograde Transport-mediated Transgene Expression in Supraspinal Motor and Sensory Centers:
Widespread GFP expression in the lumbar or cervical spinal cord after subpial AAV9 delivery was associated with robust retrograde and anterograde infection-mediated GFP positivity in the supraspinal descending axons and their projecting neurons and in axons and terminals of ascending tracts (Figure 4). Thus, intense GFP positivity was seen in neurons localized in the reticular formation (RF), nucleus ruber (NR), and motor cortex (MC) (Figure 4B-4D). Similarly, clear GFP immunoreactivity was seen in the terminals of the spinocerebellar (SCT), spinoreticular, and spinothalamic tracts (STT) (Figure 4B-4D).
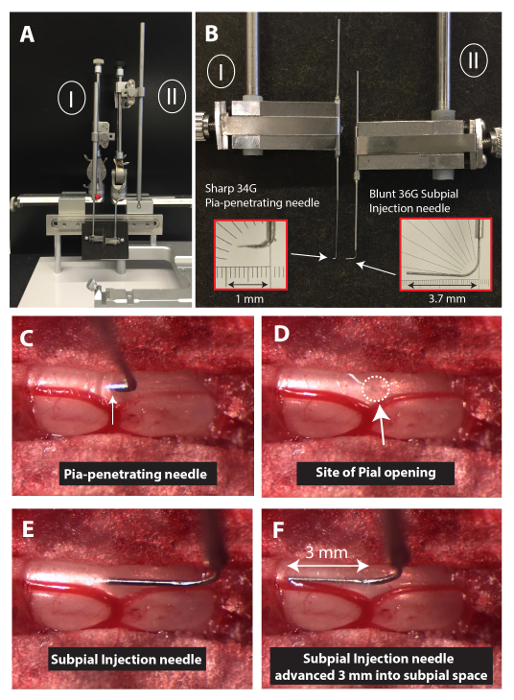
Figure 1: Experimental Setup to Perform Spinal Subpial Injections in an Adult Mouse. (A) To perform spinal subpial injections in adult mice, two separate XYZ manipulators are used (I and II). (B) The Z-arm of each manipulator holds a glass capillary holder. One capillary holder holds the pia-penetrating 34 G needle, and the second one holds the blunt 36 G subpial injection needle. (C, D, E, and F) Images depicting the position of the pia-penetration needle just after the pia puncture (C; dura matter is already removed), after removal of the pia-penetrating needle (D), after the insertion of the tip of the subpial injection needle (E), and after advancing the subpial injection needle 3 mm into the subpial space (F). Please click here to view a larger version of this figure.
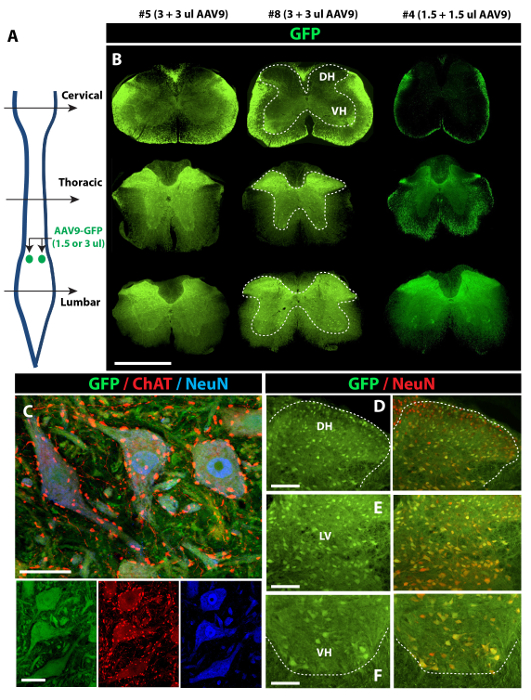
Figure 2: Potent Spinal Parenchymal GFP Expression after Lumbar Subpial AAV9-UBI-GFP Delivery in Adult Mice. (A) Two bilateral injections of AAV9-UBI-GFP (1.5 or 3 µL injections each) were delivered into the upper lumbar subpial space, and animals were perfusion-fixed 14 days after AAV9 delivery. (B) Intense GFP expression in the gray (inside the dotted area) and white matter, extending from the lumbar to the upper thoracic segments, can be seen in animals injected with 3 + 3 µL of AAV9 (left and middle columns). (C, D, E, and F) Co-staining of transverse spinal cord sections taken from the lumbar enlargement in animals injected with 3 + 3 µL of AAV9 show GFP expression in virtually all ChAT (α-motoneuron marker)-positive α-motoneurons (C and F) and NeuN-positive interneurons in the dorsal horn (D) and intermediate zone (E). Scale bars = 1,000 µm (B); 30 µm (C); 100 µm (D-F). DH: dorsal horn; LV: lamina V; VH: ventral horn. Please click here to view a larger version of this figure.
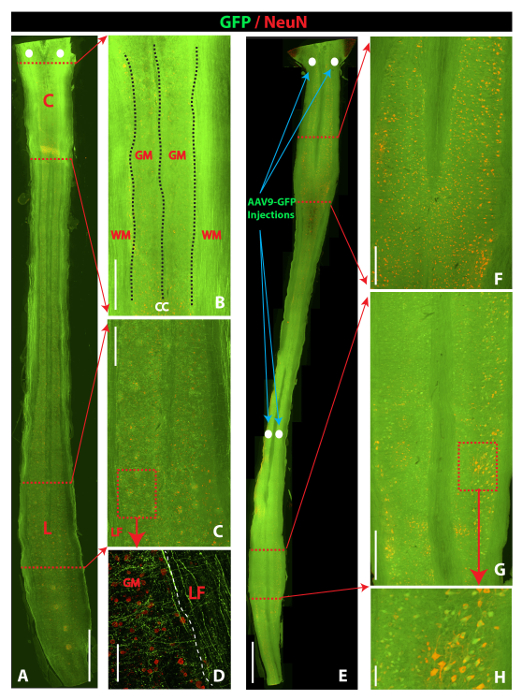
Figure 3: Comparison of Spinal GFP Expression After Spinal Subpial Cervical Versus Spinal Subpial Cervical plus Subpial Lumbar AAV9-UBI-GFP Delivery in Adult Mice. (A, B, C and D) Horizontal section cut through the whole length of the spinal cord in an animal that previously received upper cervical subpial injections of AAV9-UBI-GFP (5 + 5 µL). Intense GFP expression in the white and gray matter in the cervical region can be seen (B). In the lumbar spinal cord, a high density of GFP+ descending axons in the lateral funiculus (LF) and the gray matter between NeuN-positive but GFP-negative neurons can be identified (C and D). (E, F, G, and H) Horizontal section cut through the whole length of the spinal cord in an animal previously receiving upper cervical and upper lumbar subpial injections of AAV9-UBI-GFP (5 + 5 µL at the cervical and lumbar level). Intense GFP fluorescence throughout the whole spinal cord (white and gray matter) can be seen. Individual NeuN-stained interneurons and α-motoneurons co-expressing GFP can readily be identified in cervical (F) and lumbar (G and H) spinal gray matter. Scale bars = 2,000 µm (A and E); 500 µm (B, C, F, and G); 100 µm (D and H). C: cervical; L: lumbar; WM: white matter; GM: gray matter; LF: lateral funiculus). Please click here to view a larger version of this figure.
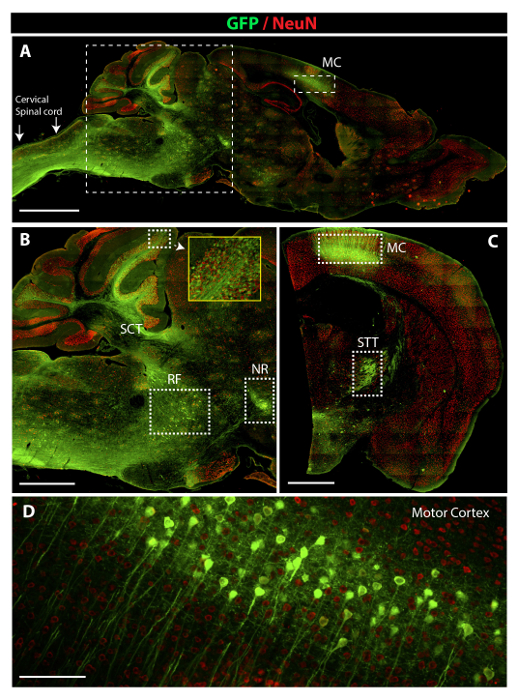
Figure 4: Potent Retrograde and Anterograde AAV9-UBI-GFP-mediated GFP Expression in Brain Motor and Sensory Centers. (A) A low-power image depicting the presence of intense GFP positivity in the cervical spinal cord, medulla oblongata, cerebellum, and motor cortex (MC). (B) A higher-power image taken from a sagittal brain section and showing the presence of GFP fluorescence in neurons in the reticular formation (RF), nucleus ruber (NR), and axons of the spino-cerebellar tract (SCT). (C) A lower-power image taken from coronal brain sections showing the presence of GFP fluorescence in pyramidal neurons in the motor cortex (MC) and in the terminals of the spinothalamic tract in areas of the reticular thalamic nuclei (STT). (D) A high-power image demonstrating an intense GFP expression in pyramidal neurons in the motor cortex. Scale bars = 2,000 µm (A); 1,000 µm (B and C) ; 60 µm (D). Please click here to view a larger version of this figure.
| Experimental Groups | Site/level of AAV9 delivery (*) | Volume of AAV9 inj, infusion rate | Survival time | Tissue analysis |
| Group A (n = 7) | C2 (bilateral) | 5 µL/5 min | 14 days | Brain + spinal cord |
| Group B (n = 12) | L1-L2 (bilateral) | 1.5 µL or 3µL, 60 sec/µL | 14 days | Brain + spinal cord |
| Group C (n = 6) | C2 + L1-L2 (bilateral at each level) | 5 µL/5 min | 14 days | Spinal cord |
| * – bilateral = two subpial injections one delivered into the right and one to the left subpial space of injected segment(s) are performed. | ||||
Table 1: Experimental Groups. All experiments were performed in adult C57BL/6J mice.
