Hemocytometer
A typical image is shown in Figure 1 that is visualized with the microscope using the hemocytometer. Squamous cells are easily identified, as they are much larger than the non-squamous cells. These squamous cells are epithelial cells coming from the mouth. Both types of cells are stained by Trypan Blue when dead. Caution must be taken to avoid counting yeast, bacteria, and scrap.

Figure 1: Hemocytometer picture showing (A) a living non-squamous cell, (B) a dead non-squamous cell, and (C) a squamous cell. Scale bar = 50 µm. Please click here to view a larger version of this figure.
Cytospin slide: Figure 2 shows a representative image of a cytospin slide obtained after sputum processing. The different cell types (neutrophils, eosinophils, macrophages, lymphocytes, and epithelial cells) can be differentiated by means of their morphology and coloration. In some cases, contamination by squamous cells may be important and, if the percentage of squamous cells is greater than 80%, the sample is considered unsuccessful (Figure 3).
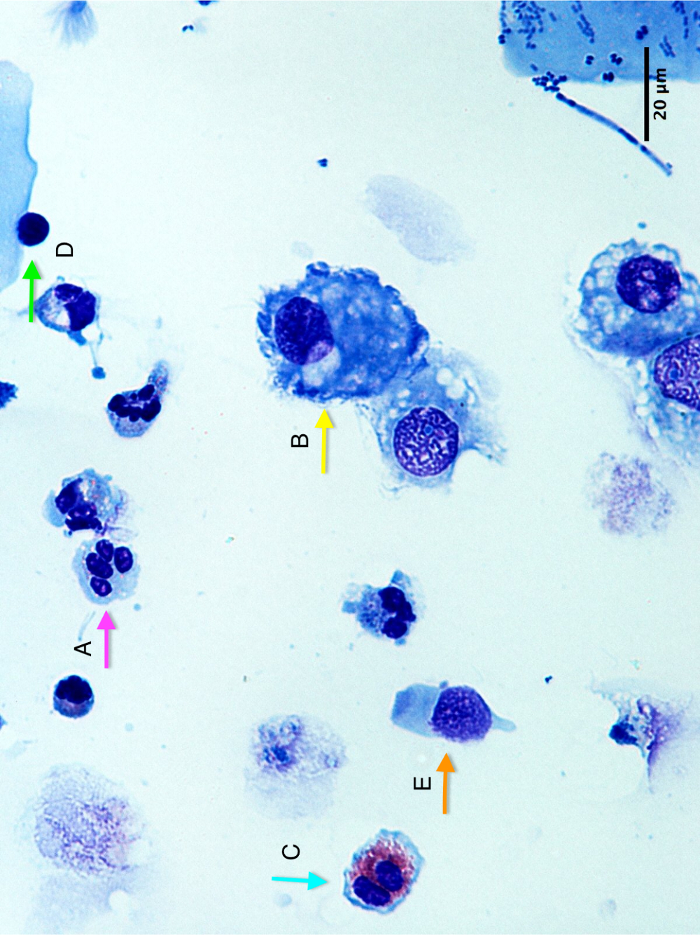
Figure 2: Cytospin slide picture showing (A) a neutrophil, (B) a macrophage, (C) an eosinophil, (D) a lymphocyte, and (E) an epithelial cell. Scale bar = 20 µm. Please click here to view a larger version of this figure.
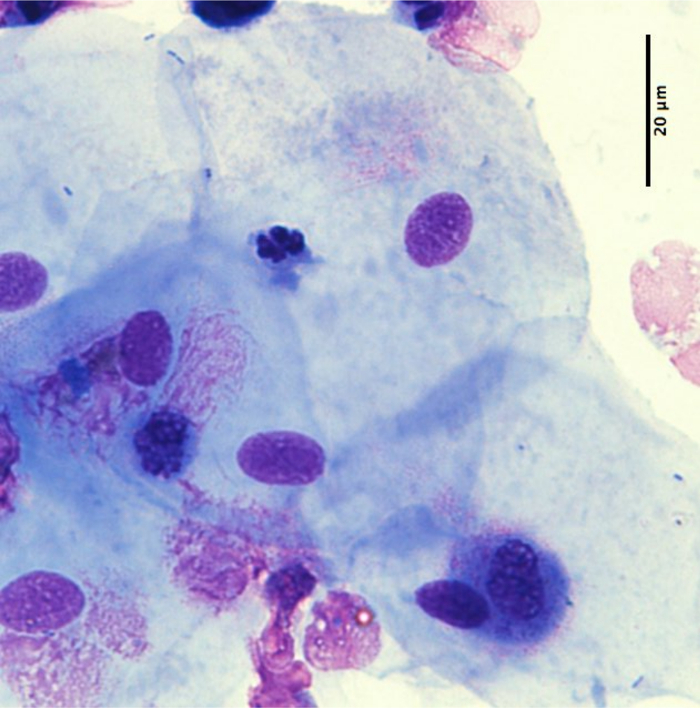
Figure 3: Example of a poor quality cytospin slide with >80% of squamous cells. Scale bar = 20 µm. Please click here to view a larger version of this figure.
Success rate
In our department, the success rate of the procedure (combining a successful induction and a readable cytospin), based on a sample of 1,129 patients (healthy subjects, asthmatics, or COPD patients), is 82% (924/1,129). In a sub-analysis according to the type of patients, the success rate is 75% (57/76) in healthy subjects, 82% (827/1,004) in asthmatics, and 82% (40/49) in COPD patients.
Results in healthy subjects
In a retrospective analysis of a series of 289 healthy subjects from our department, the median (interquartile range) sputum weight was 3.72 g (interquartile range of 2.46 g – 5.54 g) and the median total non-squamous cell count/g of sputum was 0.59 x 106 (interquartile range of 0.37 x 106 – 1.29 x 106).
In those healthy subjects, the proportion of squamous cells is low at 19% (10%-34%) and the viability is high at 66% (54-78%). Regarding the percentage of the different cell types, results are summarized in Figure 4A. We can observe that the percentage of macrophages (49% [31-68%]) is higher than the percentage of neutrophils (34% [14%-60%]), while the percentages of lymphocytes (2% [1-3%]), eosinophils (0% [0%-0%]) and epithelial cells (4% [2-11%]) are low. These results are similar when data are expressed in absolute values (Figure 4B).
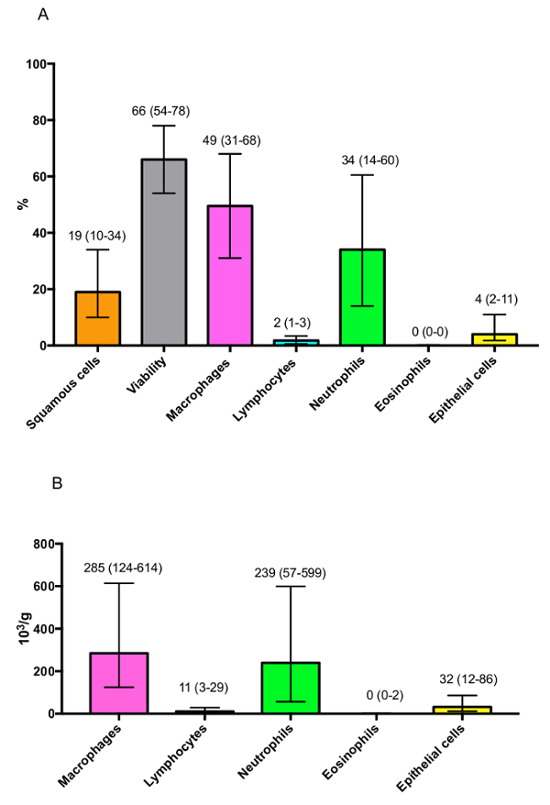
Figure 4: Representative results of the differential cell count observed in healthy subjects expressed as (A) percentages or (B) absolute values. Results are shown as median (interquartile range). Please click here to view a larger version of this figure.
It is also important to take the age of patients into consideration. Indeed, a strong correlation is present between a patient's age and the proportion of neutrophils in sputum samples (Figure 5). Likewise, when classifying patients according to 10 year age groups (Figure 6), we observed a significant increase in the neutrophil percentage with increasing age group. Therefore, this variable must be considered when comparing results from different cohorts, and caution must be taken in the matching of subjects.
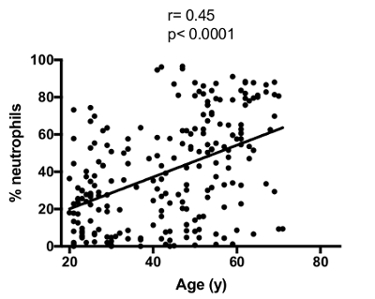
Figure 5: Correlation between age and sputum neutrophil percentage. The correlation was calculated with the Spearman test. Please click here to view a larger version of this figure.
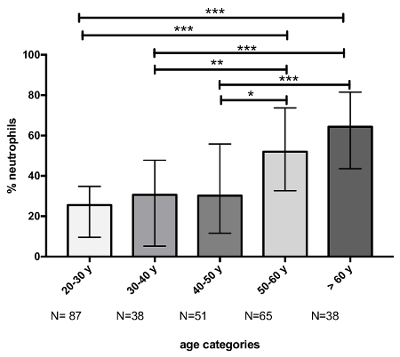
Figure 6: Evolution of the neutrophil percentage according to the age category. The p-value of ANOVA was <0.0001 for the comparison of neutrophil percentage between age classes. Multiple comparisons were made with Dunn's multiple comparisons test. The p-values are represented as follows: * p <0.05, ** p <0.01, and *** p <0.001. Results are shown as median (interquartile range). Please click here to view a larger version of this figure.
Results in patients suffering from respiratory diseases
The technique of induced sputum is commonly used to assess the inflammatory cell profile in asthmatic patients. This technique may also be applied to patients suffering from COPD, another inflammatory respiratory disease. When comparing healthy subjects, asthmatics, and COPD patients (the 3 groups being matched for age, gender, and tobacco habits), we observed that the inflammatory cell profile is quite different between these cohorts (Figure 7). Indeed, asthmatic patients are usually characterized by raised sputum eosinophils, while the proportion of sputum neutrophils is usually higher in COPD patients compared to healthy controls, which is linked to the disease severity.
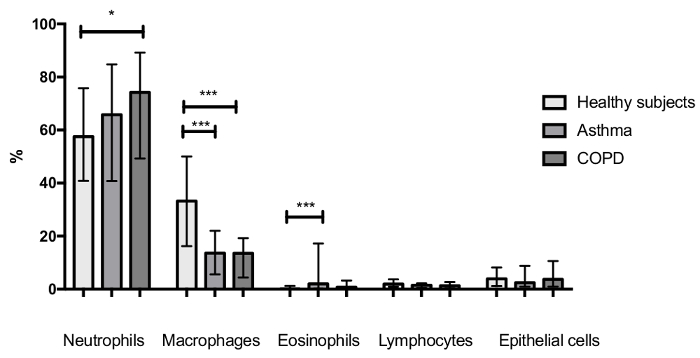
Figure 7: Sputum inflammatory cell profile of healthy subjects (n = 45), asthmatic patients (n = 108), and COPD patients (n = 54). The three groups were matched for gender, age, and tobacco habits. The p-values of ANOVA were <0.05, <0.0001, and <0.0001 for the comparison of neutrophils, eosinophils, and macrophages between groups, respectively. Multiple comparisons were made with Dunn's multiple comparisons test. The p-values are represented as follows: * p <0.05 and *** p <0.001. Results are shown as median (interquartile range). Please click here to view a larger version of this figure.
