This study details a method to create an anatomically realistic neonatal heart model combining MRI imaging, 3D printing, and cold injection molding. The ductus arteriosus as well as foramen ovale were not included in the heart model presented in this paper. The method described in this paper can also be applied to other internal organs, such as lungs, and rib cage structures. Rib cage structures require no molds and can be printed directly using flexible materials. In (Figure 7), we depict several of these examples. Using the heart model in conjunction with these other artificial body parts creates a complete thoracic replica to use as a training tool or testing platform for non-invasive as well as invasive clinical interventions.
The challenge of recreating a complete and anatomically realistic model lies with the fact that four chambers, as well as valves, have to be cast as one part. If separate parts were to be cast and at a later stage glued together, less anatomical accuracy will be retained. Furthermore, gluing segments together using silicone material may cause potential ruptures when using the heart model during compressions.
The resolution of 3D printing intricate parts (Figure 1) is essential for the realization of small organic components such as the heart system. Because the detail in these models' chambers and valves determines the functionality of the final model, then with higher resolution of the print, there will be higher resolution of the final product. This is especially the case with the valves being an integrated part of the mold. If these inner mold parts are not printed facing a direct vertical position, the delicate valves will break during the cleaning process which will result in misshaped valves after casting.
Cleaning of the printed parts should be done using a solution of sodium-hydroxide and left to dry for 48 h afterward. Otherwise, the leftover support material will inhibit the silicone from curing, which will result in failed valve casts as well as an extremely tacky exterior of the heart model.
The use of very flexible inner mold materials using 3D printing offers the possibility of creating organic and complex structures to be released from the final cast part (Figure 4). If these inner mold parts were to be printed in solid materials, the heart model part would be destroyed when removing the inner chambers.
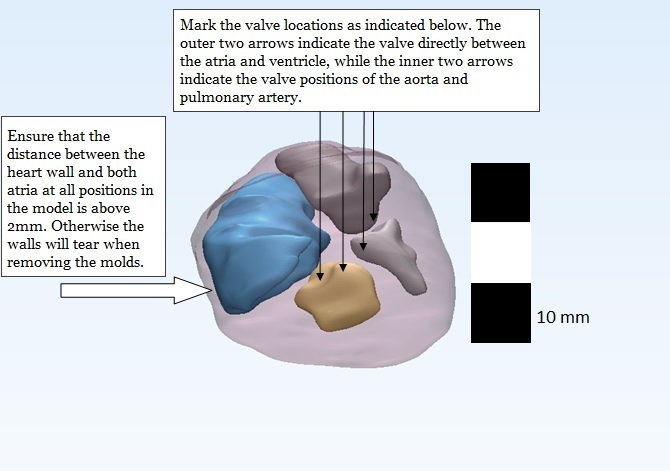
Figure 1: The finished MRI model. The model should contain the following five solids: heart wall, left and right atria, and left and right ventricle. Smoothing these parts is essential for a high-quality print and the subsequently high-detailed cast of the heart model. Notes of the positioning of the heart valves should be used for reference in editing the heart model in CAD software. Also, the space between the atria and heart wall should be a minimum of 2 mm to prevent rupturing of these walls when removing the inner molds.
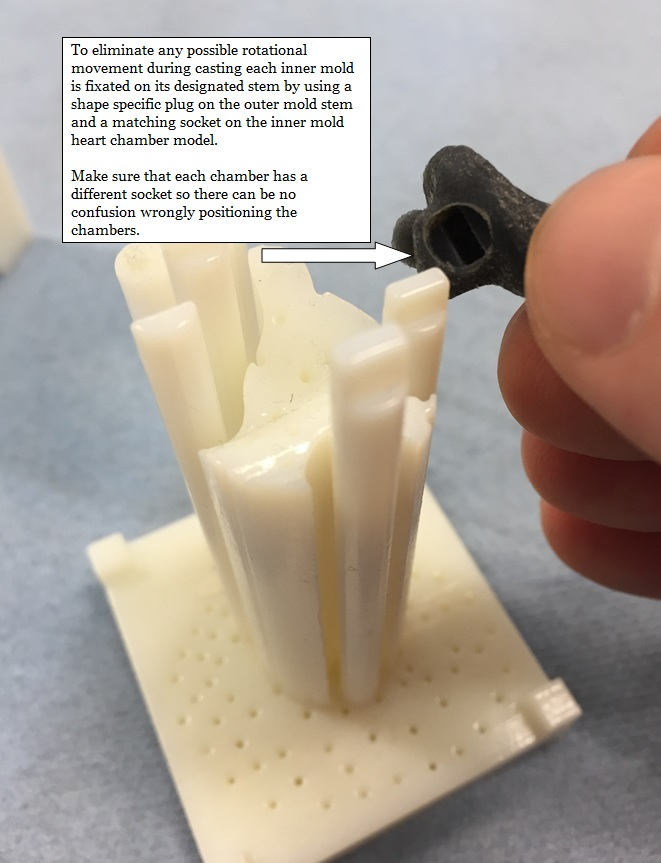
Figure 2: Adding sockets to fixate the inner mold parts is essential for positioning. Without these, the inner molds will drift, and the valves will be a guaranteed miscast. The attachment of sockets in the negative valve parts also is essential for minimizing the inner mold fixation points, providing the least amount of disturbance to the anatomy of the model.
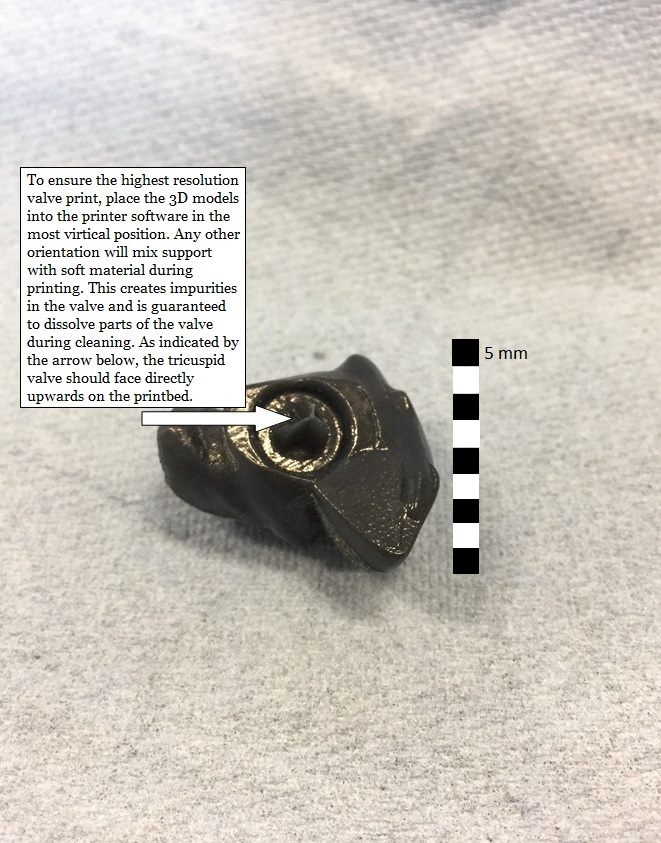
Figure 3: When printing the molds, the heart valve parts should always be printed facing an upward position in the glossy mode to guarantee accurate geometry. This also prevents support material from clogging up the cavities of the valve, which might disrupt the geometry after the cleaning process is complete.
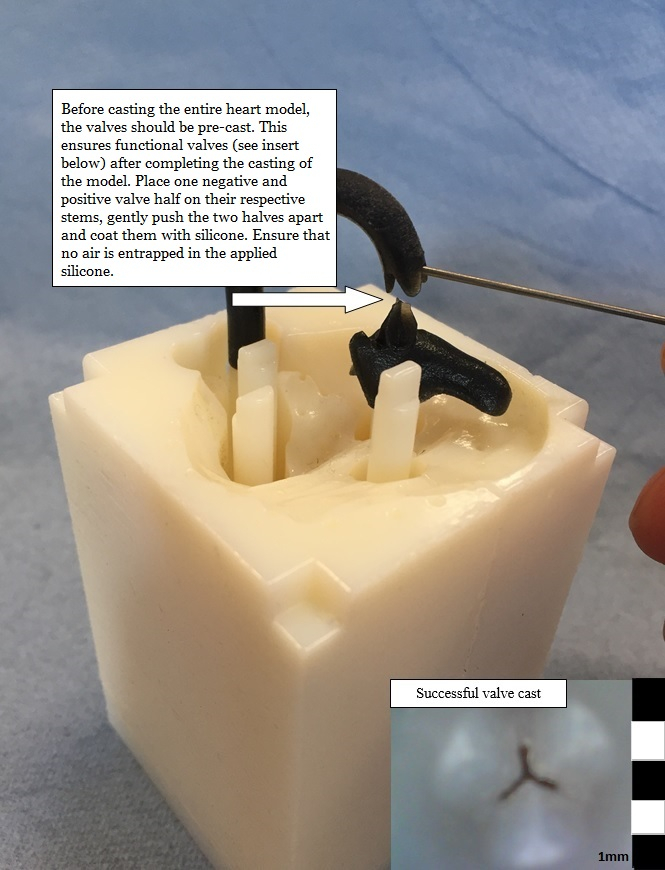
Figure 4: Adding silicone to the valves before cold injection molding the rest of the model is crucial. Assembling the valves and applying silicone for every valve separately is essential to prevent air entrapment, which would render the valve's functionality useless. Due to the extremely narrow channels between the valve halves, as well as the lack of air vents in these locations, it is otherwise impossible for silicone to reach the entirety of all semilunar valves during cold injection molding.
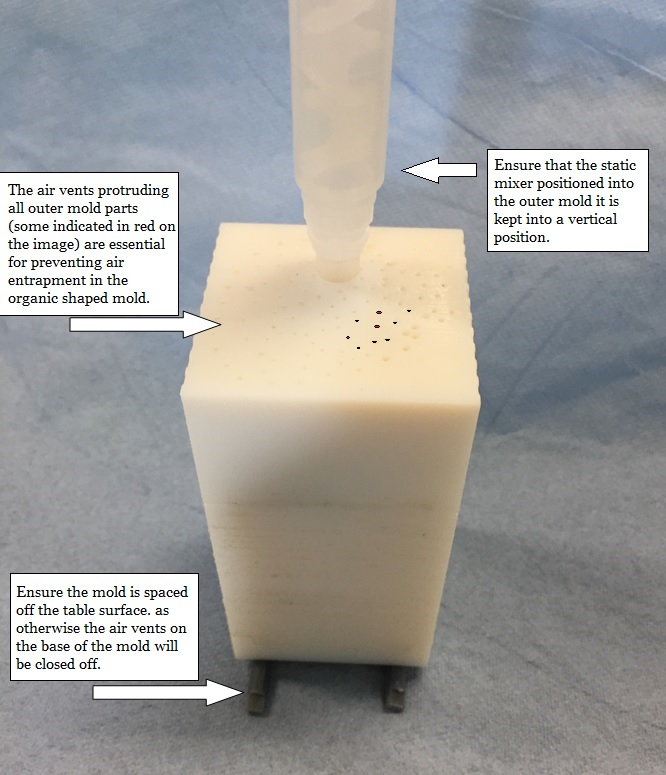
Figure 5: Mount the mold on spacers to ensure the air vents can function during the molding process. While one person holds the mold in place, as well as counts the minutes into the casting process, the second should slowly and steadily inject the silicone into the mold using the ejector gun. The lower the speed at which the silicone is injected into the mold, the less air entrapment will be present in the final heart model.
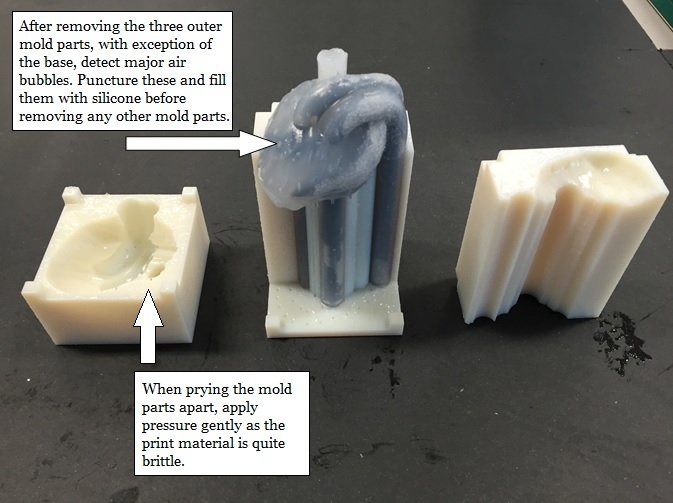
Figure 6: After releasing the top and side parts of the mold, inspect the heart for any air entrapments. These entrapments should be punctured and filled with silicone using a toothpick and left to cure for another 30 min before the final stages of demolding are performed.
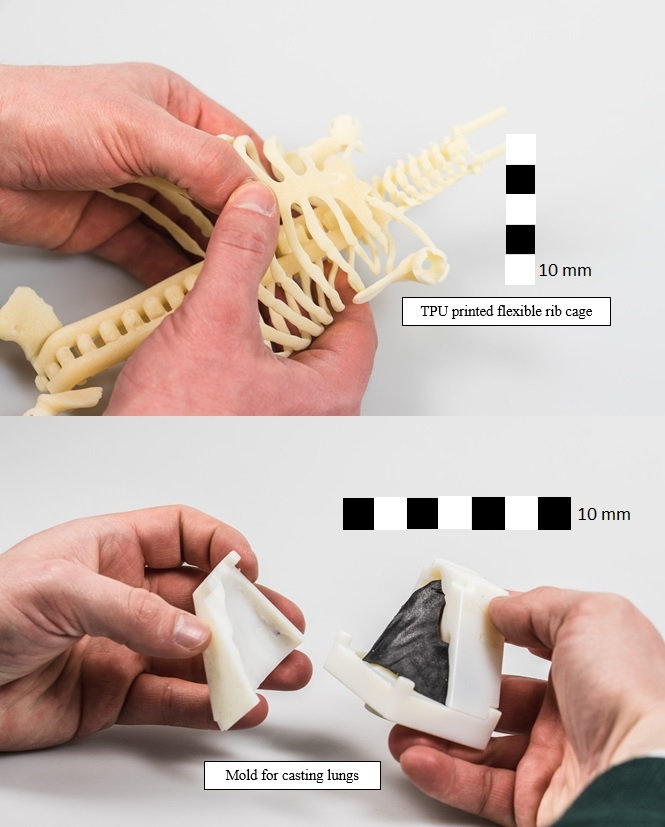
Figure 7: The additionally modeled and printed lung mold (following this manuscript's protocol) and rib cage (printed in thermoplastic polyurethane (TPU)). These models enable the replication of a complete neonatal thoracic model for use during training of clinicians in the fields of anatomy, surgery, or to visualize the effects of chest compressions on the neonatal thorax. The organs produced using the method described in this paper have a perfect anatomical fit with each other as they all are based on the same MRI scan.
