Mesenchymal stem cells (MSCs) are known to have the capability to regenerate cartilage1,2,3,4,5,6. They can be easily obtained from various sources: bone marrow, cord blood, and adipose tissue among many others. Among these sources, adipose tissue is the only source where a sufficient number of MSCs can be obtained without any culture expansion to regenerate cartilage in clinical settings7,8. Autologous bone marrow stromal vascular fraction (SVF) can be easily obtained as well. However, the number of stem cells contained in the non-culture expanded marrow is very low7,8. Cord-blood may contain a sufficient number of MSCs. However, cord blood is not a readily available source of autologous SVF.
Numerous methods of processing adipose tissue to obtain SVF are available for clinical applications. Among these, the method of obtaining MSCs from adipose tissue using collagenase, developed and confirmed by Zuk et al.5,6, is very well accepted. This method of using collagenase has been modified for clinical applications in orthopedics. In order to be applied to clinical settings, the system must be a closed system to maintain the sterility while keeping the convenience. One particular modification presented in this article involves homogenization of the lipoaspirates. Small sized lipoaspirates are digested relatively faster than the larger ones that are resulting in the uneven breakdown of adipose tissue. Furthermore, these larger sized lipoaspirates may produce fibrous tissues that can clog up the syringes and needles while performing joint injections9,10. In order to prevent these issues, the lipoaspirates may be homogenized by cutting and mincing the lipoaspirates before the incubation with collagenase. The resulting adipose tissue-derived SVF may contain more uniform extracellular matrix (ECM) compared to lipoaspirates that are not homogenized11. The broken-down ECM contained in the SVF may work as a scaffold12.
In 2009, autologous adipose tissue-derived SVF has been allowed by the Korean Food and Drug Administration (KFDA) when processed within a medical facility with minimal processing by a physician13. Afterwards, autologous adipose tissue-derived SVF has been utilized as a potential agent to improve knee functions in osteoarthritis (OA) patients by potentially regenerating cartilage-like tissue10,14,15,16,17,18.
In 2011, Pak showed for the first time that adipose tissue-derived stem cells (ASCs) contained in the adipose tissue-derived SVF can improve knee functions potentially regenerating cartilage-like tissue in human OA patients when injected with platelet-rich plasma (PRP) 14. In addition, Pak et al. have reported safety data in 2013 involving 91 patients. The mean efficacy rate reported in this safety data was 67%15. Subsequently, additional studies by Pak et al. showed improved knee functions potentially due to cartilage-like tissue regeneration in patients with a meniscus tear and chondromalacia patellae10,16,17,18. Based on articles reported, it is known that the number of stem cells contained in 100 g of adipose tissue processed by the protocol presented in this article may range from 1,000,000 – 40,000,000 depending on patients' characteristics8,19,20,21,22,23.
Here, we present a clinical protocol of human knee OA by using autologous adipose tissue-derived SVF with HA and PRP activated with calcium chloride. The first version of this clinical protocol, involving a closed, manual system to maintain the sterility, was reported in 201114. The identical protocol was optimized, maintaining sterility, and was reported in 2013 and 201610,15. Here, the optimized protocol is presented. The schematic overview of the protocol is presented in Figure 1.
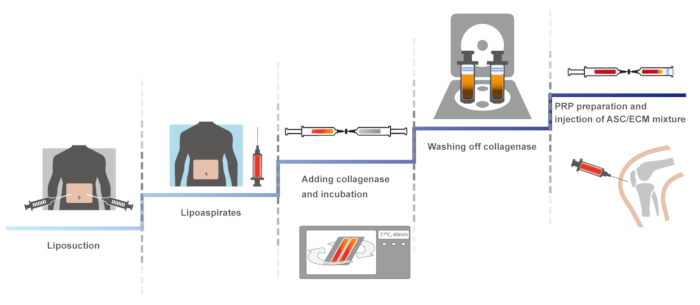
Figure 1: The schematic overview of the protocol. Please click here to view a larger version of this figure.
Three patients (one 87-year-old female with stage 3 OA, one 68-year-old male with stage 3 OA, and one 60-year-old female with stage 3 OA) without any significant past medical history presented to the clinic with persistent knee pain and desired for potential autologous adipose tissue-derived SVF treatment. All three patients had their knee examined by an orthopedic surgeon and were offered to have total knee replacement (TKR) and were reluctant to have the surgery. Prior to the procedure, all three patients had received multiple injections of steroids and HA without any prolonged improvement.
The 87-year-old Korean female patient, at the time of examination, complained of severe pain (VAS score of 8; Figure 2A) while on rest. She described the pain to be increasing ([FRI: 37; Figure 2A) when walking up and down stairs. On physical exam, mild joint swelling with decreased ROM and tenderness with flexion (Figure 2B) were noted. However, no ligament laxity was appreciated. McMurray's and Apley's tests were negative. A before-treatment MRI demonstrated a decreased size medial meniscus along with deformation and maceration. (Figure 2C, 2E, 2G, and 2I).
The second patient, a 68-year-old Korean male, complained of severe left knee pain (VAS score: 7; Figure 3A) while on rest. The pain (FRI: 33; Figure 3A) was described as increasing when walking up and down stairs. On physical exam, there was mild deformity with mild joint swelling. ROM (Figure 3B) was decreased. Further, no ligament laxity was appreciated. McMurray's and Apley's tests were negative. A before-treatment MRI showed cartilage thinning along with a decreased size and deformed medial meniscus secondary to the previous meniscectomy (Figure 3C, 3E, 3G, and 3I). The patient was diagnosed to have stage 3 OA.
The third patient, a 60-year-old Korean female, also reported severe pain (VAS score: 8; Figure 4A) on rest. The pain (FRI: 36; Figure 4A) was described as increasing when walking. The patient also had mild knee swelling and decreased ROM (Figure 4B). No ligament laxity was appreciated. McMurray's and Apley's tests were negative. A before-treatment MRI showed decreased size medial meniscus with deformation and maceration, and there was cartilage thinning (Figure 4C, 4E, 4G, and 4I).
Treatment Plan. All three representative patients were restricted from taking steroids, aspirin, non-steroidal anti-inflammatory drugs (NSAIDs), and Asian herbal medications at least for 1 week prior to the procedure. After taking MRI imaging studies, lipoaspirates were obtained and processed as referenced above. Afterwards, the autologous adipose tissue-derived SVF containing ASCs, ECM, HA, and calcium-chloride-activated autologous PRP were injected to the knees at day 0. There was no complication due to liposuctions and joint injections. Subsequently, the patients returned to the clinic in one week, then 2 weeks, and then 3 weeks for additional injections of HA and autologous PRP activated with calcium chloride.
Outcome. After the second week of the ASC/ECM mixture injection, the 87-year-old female patient's pain and ROM improved (Figure 2A and 2B). By the 16th week, the patient's pain and ROM significantly improved by more than 70% (Figure 2A and 2B). Post-treatment MRI taken after the 16th week showed the increased thickness of hyaline cartilage-like tissue on the medial side of the knee (Figure 2D, 2F, 2H, and 2J). As a comparison, the mean efficacy rate was 67% in data using this clinical protocol, involving 91 patients, and reported in 201315.

Figure 2: Outcome of pain measurements (A) and range of motion (B); and MRI sagittal (C-F) and coronal (G-J) sequential T2 views of the knee from the patient case 1.* indicates a statistically significant finding (p < 0.05). Pre-treatment MRI scans (C: sequential image, 5/20; E: 6/20; G: 10/20; and I: 11/20) show cartilage lesions (arrows). Post-treatment MRI scans at 16 weeks (D: 6/20; F: 7/20; H: 10/20; and J: 11/20) indicate cartilage-like tissue regeneration (arrowhead) that has been repaired by ASC/ECM mixture-based treatment. This figure has been modified from the previous report of Pak et al.10. Please click here to view a larger version of this figure.
The 68-year-old male patient's pain and ROM improved after the second week of the ASC/ECM mixture injection (Figure 3A and 3B). By the 18th week, his pain and ROM significantly further improved to 80% (Figure 3A and 3B). Repeated MRI taken after 18th week showed an increase in the height of hyaline cartilage-like tissue on the anterior medial side of the knee (Figure 3D, 3F, 3H, and 3J).

Figure 3: Outcome of pain measurements (A) and range of motion (B); and MRI sagittal (C-F) and coronal (G-J) sequential T2 views of the knee from the patient case 2.* indicates a statistically significant finding (p < 0.05). Pre-treatment MRI scans (C: sequential image, 6/20; E: 7/20; G: 13/20; and I: 14/20) show cartilage lesions (arrows). Post-treatment MRI scans at 16 weeks (D: 6/20; F: 7/20; H: 13/20; and J: 14/20) indicate cartilage-like tissue regeneration (arrowhead) that has been repaired by ASC/ECM mixture-based treatment. This figure has been modified from the previous report of Pak et al.10. Please click here to view a larger version of this figure.
The 60-year-old female patient's pain and ROM improved approximately 50% after the second week of the ASC/ECM mixture injection, (Figure 4A and 4B). By the 22nd week, the pain and ROM significantly improved over 80% (Figure 4A and 4B). Repeated MRI taken after the 22nd week showed an increase in the height of the hyaline cartilage-like tissue on the medial side of the knee (Figure 4D, 4F, 4H, and 4J).

Figure 4: Outcome of pain measurements (A) and range of motion (B); and MRI sagittal (C-F) and coronal (G-J) sequential T2 views of the knee from the patient case 3.* indicates a statistically significant finding (p < 0.05). Pre-treatment MRI scans (C: sequential image, 4/20; E: 5/20; G: 10/20; and I: 11/20) show cartilage lesions (arrows). Post-treatment MRI scans at 16 weeks (D: 4/20; F: 5/20; H: 10/20; and J: 11/20) indicate cartilage-like tissue regeneration (arrowhead) that has been repaired by ASC/ECM mixture-based treatment. This figure has been modified from the previous report of Pak et al.10. Please click here to view a larger version of this figure.
