Procedures involving human subjects have been performed according to the National Guidelines of the Italian Radiological Society
1. Patient preparation
- Help patients to fill in a form which provides information on their history, current symptoms, treatments (either medical or surgical), and prior medical records, if any.
- Obtain each patient's written consent before beginning the examination.
- Clearly explain in advance the characteristics and purpose of the procedure, including the performance of various maneuvers such as squeezing, straining, and rectal emptying.
- Give information on the duration (average time: 25 min) of the procedure and the need for the insertion of a small catheter into the anal canal for contrast administration (acoustic gel).
- Ask the patients to empty their bladder in the toilet just before starting the examination.
NOTE: On the basis of the patients' histories and presenting symptoms, tailor the procedure to each single case with regard to the amount of contrast administered and the number of scan planes and pulse sequences used.
2. Diagnostic room and facilities
- Keep a trolley inside the area of the diagnostic room, equipped with all necessary instruments and supplies, including gloves, syringes, a catheter, lubricant jelly, acoustic gel, etc. (see Table of Materials).
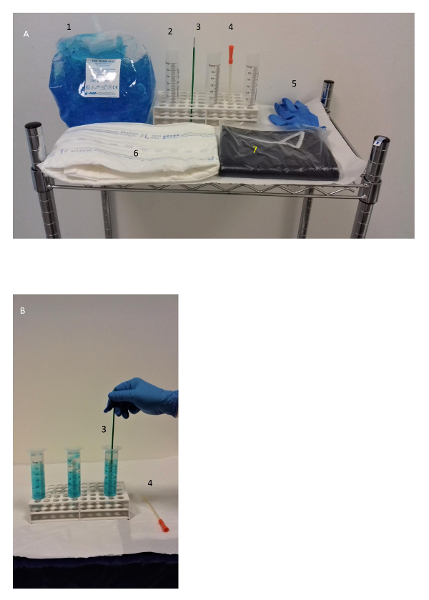
Figure 1: Supplies. This picture shows (A) a trolley with supplies for the MR examination and (B) the dilution of acoustic gel with water (50/30 mL per syringe) in the area adjacent to the diagnostic room before the administration. Please click here to view a larger version of this figure.
- Ask the patient to lay on the diagnostic table of the MR scanner in the left lateral position (Sims' position). Gently insert the catheter into the rectum and administer the contrast administration (acoustic coupling gel) until the patient experiences a characteristic desire to evacuate (the average amount is 250 mL). Turn the patient in the supine position afterward.
- Adjust the absorbent pad beneath the buttocks, and wrap around the patient's pelvis a surface phased-array coil for the image acquisition.
NOTE: In case of anticipated sensation, urgency, discomfort, or involuntary leakage, interrupt the injection and register the total volume injected before the leakage, as well as the volume leaked.
3. Technique and image acquisition
- Acquire a localizer scout scan in the coronal, axial, and sagittal planes (TFE T1 pulse sequence, TR of 8 ms, TE of 5 ms, flip angle (FA) of 25°, thickness of 15 mm, and the number of images: 5-11) to mark the boundaries of the region of interest (ROI).
- Then, obtain three subsequent dynamic series in the midsagittal plane (see Table 1, series 1: TR/TE of 2.7/1.3 ms; FA of 45°) centered over the anorectal junction, with the patient at rest, squeezing his/her anal sphincter, and straining (10 s each).
- Thereafter, instruct the patient to start – at will – the movement of rectal emptying, and notice when it starts (by acoustic device) to allow the simulatenous acquisition of images over an entire time cycle of 58 s (see Table 1, series 1: TR/TE of 2.7/1.3 ms; FA of 45°; thickness of 35 mm; acquisition time of 58 s).
NOTE: If necessary, repeat the series until obtaining an adequate stream of contrast. - Repeat the latter sequence in the coronal plane (see Table 1, series 2: TR/TE of 2.8/1.3 ms; FA of 45°; thickness of 35 mm; acquisition time of 58 s) while the patient is expelling the residual rectal contrast.
- Then, instruct the patient to perform a steady-state Valsalva maneuver without interruption for 9 s.
- Taking the sagittal images acquired during the rectal emptying as a reference, select three horizontal planes in the axial plane (see Figure 3) to image the levator hiatus as follows: the first at the midsymphysis (level I), the second tangent to the inferior border of the symphysis (level II), and the third at the point of the maximal bulging of the anterior rectal wall (level III).
NOTE: The reason for the above is to include most relevant anatomical areas inside and outside the hiatus boundaries of both sexes in the ROI: bladder base, urethra, vagina, cervix, perineal body, anorectal junction, endopelvic fascia, and fat recesses (female), or bladder base, retropubic space, prostate, seminal vesicles, Denonvilliers' fascia, anorectal junction, mesorectal fascia, and presacral space (male). - Acquire a horizontal 1 cm-thick section in the axial plane (see Table 1, series 3: TR/TE of 3/1.5 ms; FA of 45°; thickness of 10 mm; acquisition time of 9 s) from each level during the Valsalva maneuver, leaving the patient a 60 s interval between two subsequent maneuvers to relax.
- Finally, acquire static T2-weighted images when at rest in the axial, sagittal, and coronal planes (see Table 1, series 4, 5, and 6: TR/TE of 3649-4656/100; FA of 90°; thickness/gap of 4/0.4 mm; acquisition time of 3:00-3:44 min) to provide a complete evaluation of the pelvic anatomy.
NOTE: Refer to Table 1 for the technical settings.
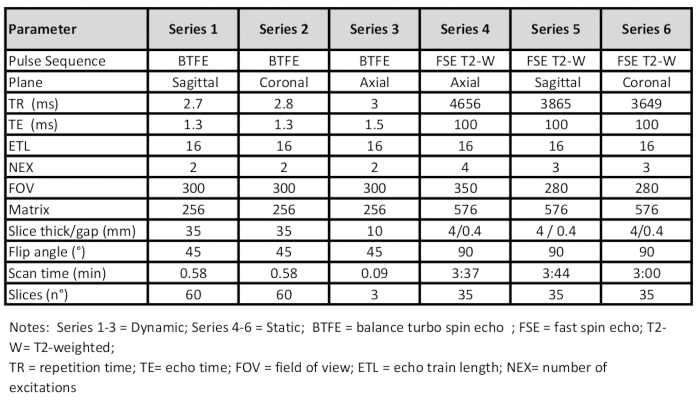
Table 1: Technical settings for MR defecography, using a 1.5 T scanner and an external coil.
4. Image analysis and measurements
- To measure the position of the pelvic organs when at rest and while straining, from midsagittal dynamic MR images in the analysis software, go to the list of toolbar options positioned at the top of the screen and hover over Annotation Tools.
- Then, click on the arrow and select Ruler to obtain a linear measurement in millimeters of the vertical distance of the bladder neck, uterine cervix, prostate base, seminal vesicles, and rectal floor from two reference lines, as follows: express the distances by negative (proximal) or positive (distal) numbers relative to the hymen plane (female) or to a horizontal line drawn tangent to the inferior border of the symphysis pubis (male).
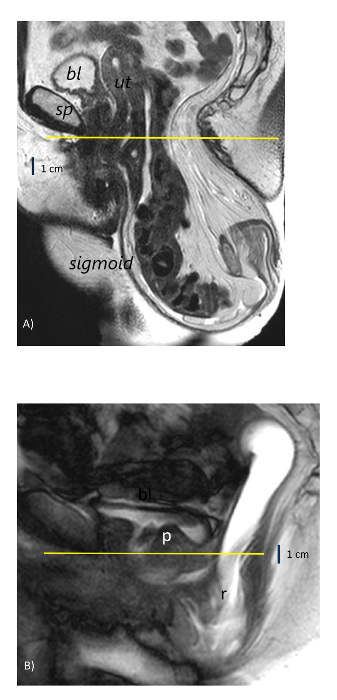
Figure 2: Reference lines for pelvic organ descent on midsagittal MR images. (A) A 61-year-old woman with a rectal descent of >10 cm below the hymen plane (yellow line) and sigmoidocele. (B) A 42-year-old man with rectal intussusception and a descent of >3 cm below the lower border of the symphysis pubis (yellow line). bl = bladder; sp = symphysis pubis; ut = uterus; r = rectum; p = prostate. Please click here to view a larger version of this figure.
- To measure the hiatal anterior/posterior and transverse diameter (in millimeters) from the axial static and dynamic images, repeat the same selection of linear measurements described in steps 4.1-4.2 and calculate the distance from the pubic symphysis to the anterior margin of the puborectalis sling and the distance between the medial borders of the levator ani muscle.
- To measure the hiatal area (in square centimeters) when at rest and during maximum strain, click again on Annotation Tools and choose Free-ROI to select a free-hand contour-tracing technique (see Figure 3).
- Depict the internal area of the levator ani muscle and express the differences between resting and straining measurements as absolute values and an increase in percentage from sections of the same level identified by the recognition of bony landmarks, namely the symphysis pubis and the ischial tuberosities (level 2).
NOTE: Register any impingement of the organs within the levator ani hiatus and refer, for organ prolapse definition and grading, to the standards recommended by the international committee on pelvic organ prolapse14,15 and to the traditional "HMO" MRI classification system of pelvic organ prolapse described by Comiter et al.9.
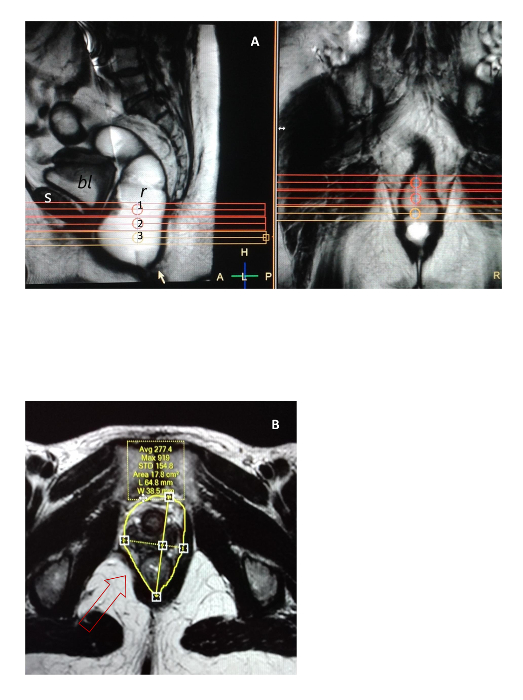
Figure 3: Method for levator ani hiatus imaging and area measurement. (A) A selection of three axial scan sections from a midsagittal image taken relative to the midsymphysis pubis (level 1), tangent to its lower border (level 2), and at the maximal bulging of the anterior rectal wall (level 3) during rectal emptying. (B) An example of an asymmetric area measured when at rest from level 2 with the free-hand contour-tracing method in a 52-year-old woman with a focal defect of the right pubococcygeus muscle (arrow). s = symphysis pubis; bl = bladder; r = rectum.The left panel = a sagittal view;the right panel = a coronal view.The area values are expressed in square centimeters.1 = first level; 2 = second level; 3 = third level. Please click here to view a larger version of this figure.
Between 2012 and 2018, this protocol has been successfully adopted in three different diagnostic centers in Italy at an average cumulative rate of 30 ± 4 exams per month, using the same 1.5 T MR scanner model and technical settings (see Table 1 and Table of Materials). During this period, over 2,000 examinations have been performed in patients of both sexes for the following three main disease categories: pelvic organ prolapse and evacuation disturbances (Group 1), ano-perianal fistula (Group 2), and chronic pelvic pain from known or suspected pudendal neuropathy (Group 3). Most relevant demographic characteristics of the patient population were: a mean age of 48 ± 3.4 years and a range of 25-82 years in males and of 51 ± 4.2 years and 34-88 years in females (Group 1); a mean age of 36 ± 3.2 years and a range of 31-82 years in males and 54 ± 2.5 years and 35-78 years in females (Group 2); a mean age of 43 ± 3.3 years and a range of 27-78 years in males and 41 ± 4.4 years and 28-78 years in females (Group 3). Each disease category led to specific variants of the MR imaging examination. Over time, the huge amount of examinations helped to obtain an almost uniform reproducibility of the protocol in subjects referred for POP and evacuation dysfunctions, until reaching the standard described herein.
The most relevant results can be summarized as follows: pelvic organ prolapse also occurs in males (see Figure 2B), although it is more common in females18,19,20. In addition, regardless of sex, levator ani hiatus ballooning when straining (see Figure 4) has emerged as the most reliable index of the disease. Its area can easily be quantified with axial dynamic MR pelvic imaging and graded as normal (≤20 cm2), as a prolapse of the first or second degree (20-40 cm2), or as a prolapse of the third or fourth degree (≥40 cm2), or it can be described as an increase of >100% compared to the size when at rest. Interestingly, the actual enlargement of the hiatus when straining cannot be predicted based on its size when at rest, as demonstrated in a previous study in nulliparous and parous women18 whose values when at rest did not correlate with those during the Valsalva maneuver (see Figure 5). This, in turn, emphasizes the value of the present protocol. Finally, the evacuation of rectal contrast in the horizontal position is virtually coterminous with the standardization of the maximal Valsalva maneuver. More precisely, the position reached by pelvic organs under its effect can be assumed as representative of the descent reaching the maximal potential extent.
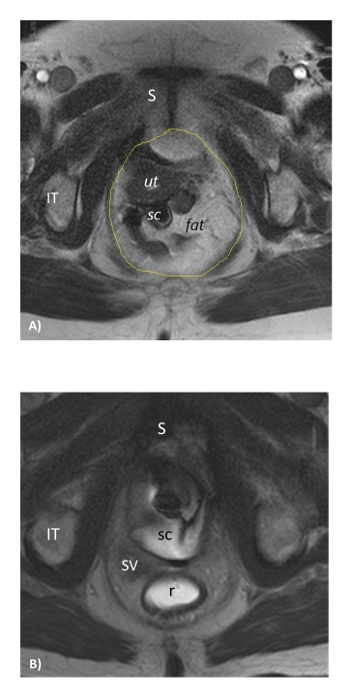
Figure 4: The ballooning of the levator ani hiatus. Depicted in the steady-state Valsalva maneuver, as seen (A) in a woman and (B) in a man with rectal prolapse (i.e., the same patients as depicted in Figure 2). S = symphysis pubis; IT = ischial tuberosity; ut = uterus; sc = sigmoid colon; sv = seminal vesicles; r = rectum. Please click here to view a larger version of this figure.
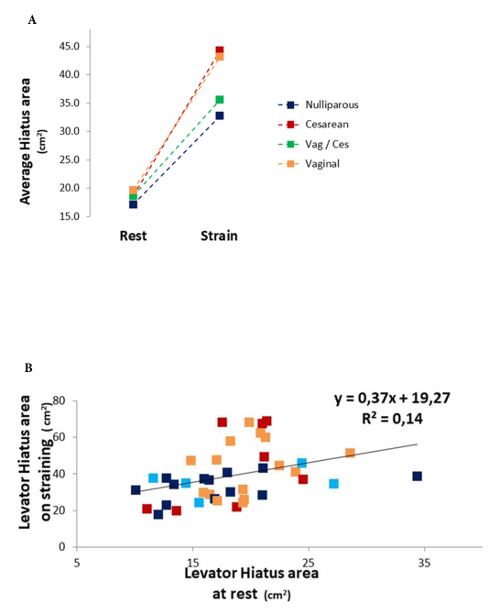
Figure 5: Results of the hiatus area measurement. (A) The graph shows an overlap of the hiatus area when at rest in nulliparous and parous women who delivered vaginally or via a cesarean section. (B) Moreover, the lack of correlation between the values when at rest and when straining indicates the inability to predict the actual enlargement in singular cases. This picture has been reproduced from Piloni et al.18 with permission. Please click here to view a larger version of this figure.
This method has an overt advantage over pelvic examinations that are limited to the assessment of the urogenital hiatus in only females. In contrast, the method presented here examines the entire levator ani hiatus in both sexes. Moreover, although easily examined by palpation by the gynecologist, the female hiatus can be calculated only approximately with a ruler, to produce the area of an oval1. Similarly, an advantage does exist over 2- and 3-D TPUS4,5, which are not suitable for male patients. However, a more important advantage of this protocol is the unique ability to document the rectal emptying function, which is peculiar to MR defecography and is done with no interference due to the proximity of the examiner or the ultrasonographic probe held close to the labia, both of which may prevent maximal pelvic organ descent. A limitation of this MR protocol, which requires the patient to be in a horizontal position, is that the absence of gravity may lead to the patient's inability to adequately empty their rectum and to a potential underestimation in the depiction of various abnormalities, due to the fact that the examination is not physiologic. It can be argued, however, that the extraordinary effort of the patient to relieve themselves of the rectal contrast in a horizontal position helps to standardize the maximal Valsalva maneuver, eliminating the uncertainty which always remains after pelvic examinations and TPUS.
For a successful performance of this protocol, the acoustic gel contrast in the syringe is diluted with water (see Table 1), added just before the administration in the area adjacent the diagnostic room, as shown in Figure 1B. In addition, it is also mandatory to follow the next recommendations. (a) Coach the patient carefully on how to produce his/her maximal pelvic strain without moving the position of the pelvis relative to the diagnostic table and without interrupting the Valsalva maneuver until they are told to breathe again and relax. (b) Select the axial MR sections relative to consistent bony landmarks (i.e., the symphysis pubis) without tilting the scan planes. This will prevent the addition of undesired factors of variability when measuring various parameters of biometry. (c) Compare the values of the hiatus diameters and the areas when at rest and when straining on axial sections identified on the basis of the same bony landmarks. This strategy is crucial for the exact spatial localization of a given change and for biomechanical inferences (see Figure6). (d) Use the hymen plane (female) and the tangent to the lower border of the symphysis pubis (male) as reference lines on sagittal MR images, instead of the more traditional pubococcygeal line (PCL)9. This will avoid discrepancies between radiologists and clinicians who are unaware of the PCL during pelvic examinations14,15.
Another limitation of the present protocol comes from the comparison with 3-D computational models21,22, which are overtly superior in depicting the pelvic floor anatomy in its entirety. However, 3-D imaging results in an overload of image analysis and interpretation which cannot be sustained equally by all examiners. Although admitting the inferiority of the present 2-D protocol due to a lack of anatomical information, we emphasize the greater ease associated with its use. As a matter of fact, it can be applied to routine assessments of the levator ani hiatus performed by all radiologists in the clinical practice, even if said radiologists are not familiar with the use of sophisticated and expensive software applications or complex mathematical formulas.
The hard limitation of this protocol for calculating the levator hiatus area remains the excessive intra-observer variation of the free-hand contour-tracing method, as shown by the fact that it is almost impossible to obtain the same result in two subsequent measurements by the same examiner. Referring to the hiatal area, the so-called "20-40-60 cm2" has been developed to discriminate patients with normal pelvic support (20 cm2 or less) from those with prolapse (between 20 and 40 cm2) and those with recurrence after prolapse repair (between 40 and 60 cm2). Rather than relying on such absolute area values, its percentage increase when straining, relative to resting values, is recommended as a more reliable index of the hiatal defective function. The most striking result obtained by this protocol is the levator ani hiatus ballooning and the pelvic organ impingement that could be demonstrated equally in nulliparous and multiparous women with pelvic prolapse and also in those who delivered their child by cesarean section. This observation partially contradicts the role of birth injury and the theory that the lateral separation of hiatal structures mainly occurs due to abnormal laxity in the vagina or its supporting ligaments, leading to organ prolapse.
This conviction is reinforced by the fact that a similar enlargement, combined with an excessive descent of the prostate base and seminal vesicles, has been demonstrated in men20. This indicates the need to consider several other factors, such as the combination of fat and the pelvic connective network as a whole, which might be seen as a sort of "interlock mechanism" responsible for the reciprocal cohesion among organs.
Conceptually, it may be hypothesized that the overcoming of such cohesive forces will lead to excessive slide motion and pelvic organ descent due to repetitive load. Under certain aspects, the quantitative analysis of the geometrical and structural deformity of hiatus boundaries, as seen with this protocol, closely reflects the action of a vector force from above which determines the displacement of pelvic organs. In the case of a decreased resistance of hard (bone) and soft tissues (skin, tendon, muscle, and fat), the application of the present protocol might contribute to a better understanding of the pathophysiology of pelvic organ prolapse.
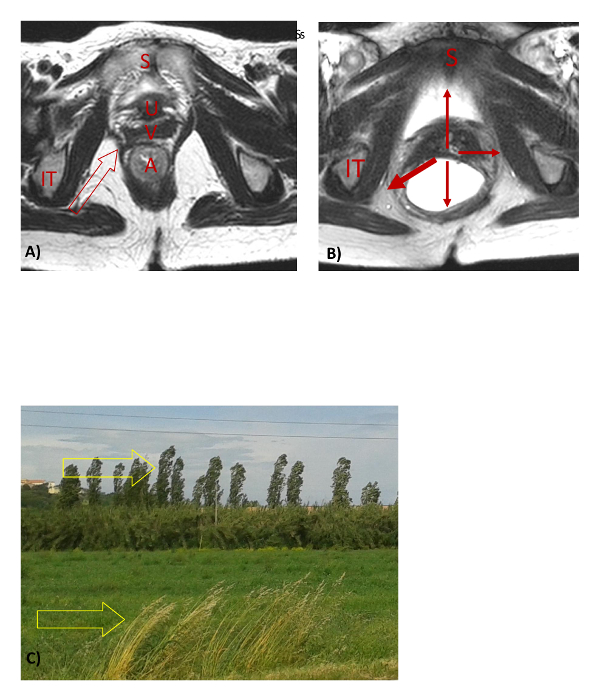
Figure 6: Effect of vector forces on solid materials. (A) A T2-weighted MR image showing a childbirth focal defect (red empty arrow) of the levator ani muscle at rest; (B) when straining, despite their equal intensity, the vector forces from the intra-abdominal pressure produce a different geometrical deformity on the hiatus boundaries (thicker red arrow) and an asymmetric hiatus ballooning. (C) The same vector force of wind (yellow empty arrows) bends trees in different ways, depending on their cross-section diameter, structure, and elastic properties. S = symphysis pubis; u = urethra; v = vagina; a = anus; IT = ischial tuberosity. Please click here to view a larger version of this figure.
