Vestibuloplasty is periodontal surgery to the oral vestibule, aiming to increase vestibular depth, the zone of keratinized gingiva and soft tissue thickness for enhanced aesthetics and function. The apically repositioned split thickness flap combined with a collagen matrix is a frequently used vestibuloplasty procedure. Xenogenic collagen matrix is a viable alternative to autogenous gingival graft for increasing the amount of keratinized gingiva11,12,13; however, no data are available on the direction of graft revascularization and on how it affects the microcirculation of the surrounding tissues. Understanding these mechanisms may facilitate proper flap and incision design in periodontal surgery.
A 17 year-old male patient with an inadequate width of keratinized gingiva at the first premolar in the maxilla was treated by vestibuloplasty, using an apically repositioned split thickness flap combined with a collagen matrix. Intraoral photographs (taken by a photo camera) and blood flow (BF) measurements by LSCI were taken before the vestibuloplasty (baseline) as well as 1, 2, 3, 4, 5, 7, 9, 11, 14, 21, 27 days and 2, 3, 4, 5, 6 and 12 months postoperatively. Blood pressure and pulse were evaluated before and after each measurement.
During offline analysis, multiple ROIs were determined in the area of the augmented mucosa; some in the graft region and others in the surrounding mucosa, defined as 'peri' regions. As shown in Figure 3, the 'peri' and graft regions were further split into zones depending on distance from the center of the implanted graft, marked as zone F in the picture. Zones A and B were defined in the 'peri' region and zones C, D and E in the graft region. Each of these zones was delimited separately at all four sides of the graft (mesial, distal, apical and coronal). Each 30-second shot was identified as a TOI (Figure 2). Data at each ROI and TOI were exported into a spreadsheet program. Blood flow curves were constructed by a suitable software used for statistical analysis.
There was no significant change in mean arterial pressure (MAP) during the one-year experiment, either in MAP before or after the blood flow measurements per session. Figure 4 shows a color photo, an intensity image and a perfusion image of the operated gingiva on the representative days of our study. During the first postoperative week complete flap closure, a thick layer of fibrin on the grafted area, and mild erythema and edema in the surrounding gingiva were visible. Blood perfusion images showed ischemia in the operated region and hyperemia in the 'peri' regions. From day 14, the grafted area was clinically erythematous, in parallel with severe hyperemia observed on blood perfusion images. By the third month after graft incorporation, the wound healed, and gingival perfusion was close to preoperative circulation levels.
Figure 5 shows a blurred intensity image and the perfusion graph of the entire image. The sudden peak on the graph indicates movement by the patient. The measurement was repeated immediately, after making sure that the patient is in a comfortable position. Changes in BF in the different zones within the graft and in the 'peri' regions are shown in Figure 6. It is common in all curves that from the fourth month, blood flow did not change any further until the end of the investigation. The average blood flow for this period could be used as a resting blood flow value for the new tissue and the random variation between time points allowed us to calculate the time-based variance component for each ROI respectively, using a linear mixed model. The minimum detectable difference could be calculated then to identify real change (with 95% confidence) between time points during the healing period (before the fourth month) in order to determine the hyperemic and the ischemic phase. The basic characteristics of curves were similar in all ROIs within the graft, starting with an ischemic phase followed by a hyperemic phase. However, the length of these two phases was different (Table 1). Ischemia was longest (7–9 days) in the central and in all coronal zones, with late hyperemia starting between day 11 and 27. In other zones of the graft, ischemia lasted only 4–7 days and hyperemia started earlier, between day 7 and 21.
The BF curves of the zones at the different sides of the graft had unique characteristics (Figure 6). At the apical side, all four zones had similar blood flow curves. At the coronal side, perfusion was regained in the outer zone later than in the inner zones, contrary to the mesial and distal side. At both lateral sides, BF increased first in zone C, then in zone D, followed by BF increase in zone E and finally in the central zone F. In the zones of the surrounding mucosa (zone A and B) no significant ischemia was observed. Instead, hyperemia of a different magnitude and extent was observed at the different sides.
There were two time points when the BF value did not tally with the overall characteristics of the BF curve. On day 9, there was a sudden drop in most zones and mainly in the 'peri' zones of the apical and distal side. It cannot be stated with certainty that this was a measurement error, as no measurements were taken on the previous and on the following day. However, according to a note in the measurement report, the buccal fold was retracted with too much pressure by the operator, resulting in a drop in BF. This makes sense considering that mainly the circulation of the distal and apical sides could have been affected by pulling the cheek. On day 182 (6 months later), due to longer intervals between measurement times, the patient has forgotten to keep to the agreed restrictions before the measurement. The bleeding of the marginal gingiva on the colored photograph (Figure 6) indicates harsh tooth brushing prior to the measurement. In the meantime, the patient underwent orthodontic treatment, too, and he used intermaxillary elastics. Both factors could greatly increase BF14,15, so the measurement was repeated at a later time under more carefully controlled circumstances.

Figure 1: Experimental LSCI setup and patient preparation for blood flow measurement in the operated area. The lips are retracted by dental mirrors. Please click here to view a larger version of this figure.
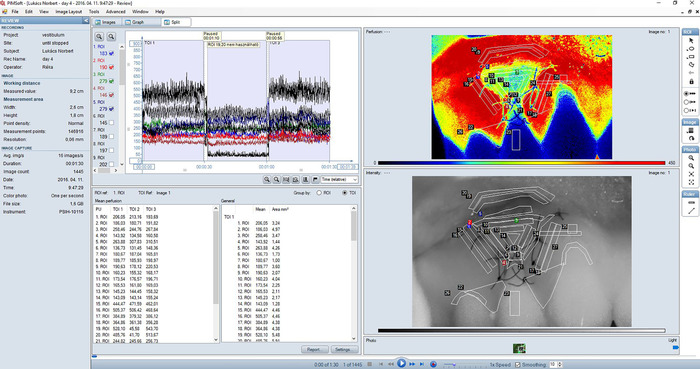
Figure 2: Split view (combination of the Images view and the Graph view) of a typical recording of gingival blood flow in the treated area. Perfusion image (upper right sub-view) is a color-coded representation of blood perfusion in the gingiva. Areas of high perfusion are shown in red while areas of low perfusion are blue. The color range of perfusion images corresponds to 0-450 LSPU; smoothing was set to 10. An intensity image (lower right sub-view) is created by the total backscattered laser light. It corresponds exactly with the perfusion image and is useful for orientation and for identifying details in the perfusion image. Regions of interest (ROI) are always defined in the intensity image. The graph (upper left panel) shows real-time blood perfusion traces for each ROI in the recording. Check boxes to the left can be used to select which traces to show. Three consecutive measurements are shown on the graph. Each 30 s shot was identified as a TOI. A mean value table showing mean perfusion values in each ROI and TOI is also displayed in Split view (lower left panel). Please click here to view a larger version of this figure.
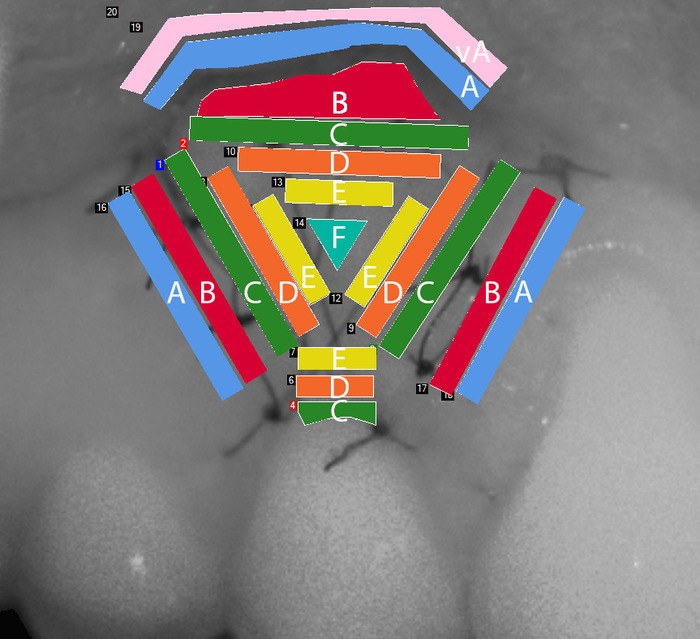
Figure 3: Regions of interest (ROI) defined within the examined gingival area in the intensity image. Zone A and B are in the 'peri' region, while zone C, D and E are in the graft at decreasing distances from the center of the graft, marked as zone F. Zone A is situated on the vestibular surface of the lips. Please click here to view a larger version of this figure.
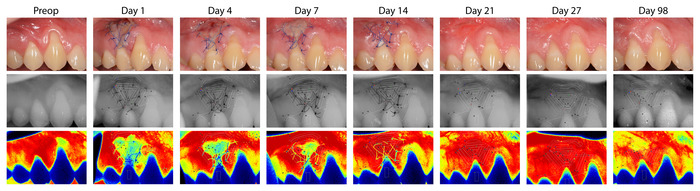
Figure 4: Representative photographs (upper line), LSCI intensity image (middle line) and LSCI perfusion image (lower line) of the operated gingiva. The images represent the preoperative state and perfusion, and wound healing and perfusion 1, 4, 7, 14, 21, 27 and 98 days postoperatively. Please click here to view a larger version of this figure.
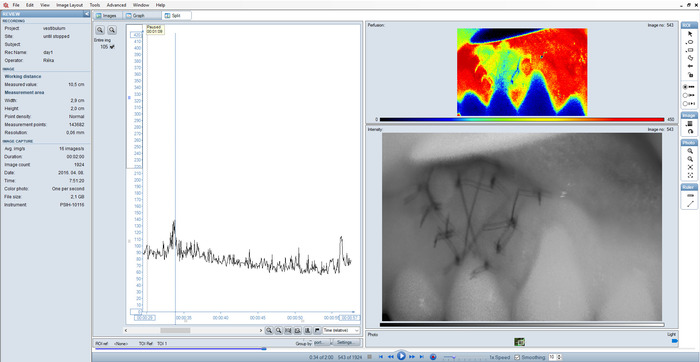
Figure 5: Split view of a sub-optimal recording. Blurred intensity image and outlying peaks on the graph as a result of incorrect setting. Please click here to view a larger version of this figure.
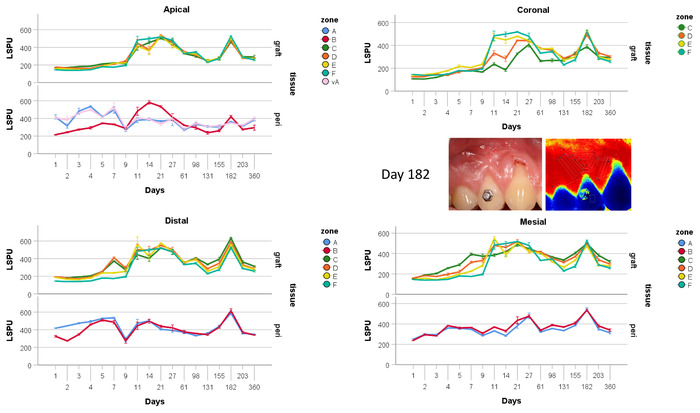
Figure 6: Scatter plot of BF over time at the coronal (a), mesial (b), distal (c) and apical (d) side of the graft. The central part of the graft (zone F) was depicted in all graphs to serve as a reference for more external zones. Please click here to view a larger version of this figure.
| Side | Zone | Ischemia end | Hyperemia start | Hyperemia end |
| coronal | c | 9 | 27 | 27 |
| coronal | d | 9 | 21 | 27 |
| coronal | e | 7 | 11 | 98 |
| central | f | 9 | 11 | 98 |
| mesial | c | 5 | 21 | 27 |
| mesial | d | 5 | 11 | 61 |
| mesial | e | 7 | 11 | 61 |
| distal | c | 5 | 11 | 27 |
| distal | d | 4 | 7 | 98 |
| distal | e | 4 | 11 | 98 |
| apical | c | 4 | 11 | 27 |
| apical | d | 5 | 11 | 61 |
| apical | e | 5 | 11 | 61 |
Table 1: Time frame of the ischemic and hyperemic phase in the various zones in the graft, in days
