All experiments in this protocol have been approved by the University of British Columbia Animal Care Committee under protocol number A17-0110.
1. Tool sterilization
- In a biological safety cabinet (BSC), turn on and preheat the hot bead sterilizer to 250 °C, at least 30 min before use.
- Dip the tools in 70% ethanol.
- Submerge the tools into the preheated hot bead sterilizer for a minimum of 1 min.
NOTE: The handles of the tools will get hot and may burn if left in the hot bead sterilizer for over 1.5 min. - Spray a mat of paper towels with 70% ethanol to sterilize it.
- Remove the tools from the hot bead sterilizer without touching the sterilized part of the tool to the nonsterile handles of other submerged tools and place them on the ethanol-sprayed paper towels.
- Wait for 30 s to 2 min for the tools to cool down before using them for dissection.
2. Cecal slurry preparation
- Preweigh 15 mL centrifuge tubes (one tube for every five mice being euthanized).
- Euthanize cecal slurry donors according to local animal care guidelines or use the protocol below.
NOTE: Up to 40 C57BL/6J mice between 6 and 12 weeks old were used for cecal slurry preparation, with up to five mice being euthanized at a time.- Transfer the mice to the euthanasia chamber and set the isoflurane anesthesia machine to 5% with oxygen perfusion.
- Monitor the mice to observe the loss of the ability to move and to see them entering the surgical plane of anesthesia and finally, stop breathing.
- Remove a mouse from the euthanasia chamber, pinch its paw and observe any leg retraction or inhalation. If either is present, return the mouse to the euthanasia chamber; otherwise, continue.
- Terminally euthanize the mice by sharp cervical dislocation.
- Perform cecum dissection, using presterilized and cooled tools (see section 1) in a BSC.
- Pin the legs of the mouse to an extruded polystyrene foam board using 23 G needles so that the mouse has its abdomen up. Secure and then spray the abdomen with 70% ethanol.
- Using sterile forceps and scissors, cut through the skin, loosen the skin from the peritoneal lining with the scissors, and cut open a rectangular region from groin to sternum, and left side to right side. Remove any fur from the peritoneum.
- Switch to a new pair of sterile tools to cut through the peritoneum, making a rectangular opening as was done for the skin, switching tools if the ones used contact the skin.
- Identify the cecum, which should be running left to right across the body. Disrupt connective tissue to identify the cecum branches from the intestines and cut the cecum away from the intestines. Place the cecum on a sterilized sheet of weighing paper.
NOTE: Weighing paper can be sterilized either by spraying it with 70% ethanol on both sides and leaving it to dry, or by UV irradiation. Alternatively, the cecum can be dissected on a sterile Petri plate.
- Cecal content extrusion
- In a BSC, use sterile tools to cut through both ends of the cecum.
- Hold the middle of the cecum with sterile forceps and use a flat sterile metal spatula to gently push the cecal contents out of the cut ends, using a rolling motion and avoiding a scraping motion that could tear the epithelium. Collect the contents and place them into a preweighed 15 mL centrifuge tube.
- Pool the cecal contents from a maximum of five mice into the same tube. Weigh the tube again once all the contents have been added.
NOTE: Expect an average of 300 mg, and up to 390 mg of cecal slurry per mouse, requiring 1.8 to 2.4 mL of D5W for resuspension per mouse; therefore, using more than five mice during this step can result in overfilling the 15 mL centrifuge tube. - Wipe the tools clean with an ethanol-sprayed paper towel and resterilize them by repeating steps 1.2-1.6.
- Cecal slurry filtration
- Weigh the centrifuge tube filled with cecal contents and calculate the amount of D5W to add to the cecal contents by dividing the weight of the cecal contents by the desired stock concentration in milligrams per milliliter, as in the equation below.

- In a BSC, add the required amount of ice-cold D5W to the 15 mL centrifuge tube containing the cecal contents.
- Vortex the 15 mL centrifuge tube vertically and horizontally for 30 s. Check for particulate of more than 1-3 mm in diameter, and if present, continue vortexing until all large particulate has visibly disappeared.
- Place a sterile 70 µm cell strainer into a 50 mL centrifuge tube that is placed on ice. Pipette 4 mL of resuspended cecal slurry into the cell strainer and, then to the collection tube. Resuspend the particulate by pipetting up and down 2x-3x. Gently extrude bubbles to increase the filtering speed while stirring the contents with the pipette tip until there are no more droplets being filtered.
NOTE: When mixing, there may be particulate large enough to plug the 5 mL pipette. In this case, repeat the vortexing from step 2.5.3, and if the solution still does not break apart, use the pipette to press the particulate against the wall of the centrifuge tube. - Repeat step 2.5.4, changing cell strainers between each tube of cecal slurry, and pool all contents into the same 50 mL centrifuge collection tube kept on ice, or into a second 50 mL centrifuge tube if the volume of the filtrate exceeds the ice level in the ice box.
- Weigh the centrifuge tube filled with cecal contents and calculate the amount of D5W to add to the cecal contents by dividing the weight of the cecal contents by the desired stock concentration in milligrams per milliliter, as in the equation below.
- Aliquot the cecal slurry.
- If applicable, combine multiple 50 mL cecal slurry filtrate tubes from step 2.5.5 into a larger sterile container (e.g., a 1,000 mL storage bottle). Then, vortex for 15 s and place 20 mL into a new 50 mL centrifuge tube.
- Vortex the cecal slurry stock that is in the 50 mL centrifuge tube for 5-10 s, and aliquot 500 µL into three 2 mL cryogenic vials that have a rubber seal, to prevent evaporation over time. Immediately place the master stock and aliquoted cryogenic vial on ice.
- Repeat steps 2.6.1 and 2.6.2 until all of the cecal slurry has been aliquoted, vortexing the master stock after every three cryogenic vials to prevent the settling of any particulate and to maintain a homogeneous mixture.
- Freeze the cecal slurry aliquots at -80 °C.
NOTE: Expect between three to four stock vials at 500 µL from each adult mouse. Each stock vial should be roughly enough to challenge one litter of eight mice at DOL 7.
3. Sepsis challenge of 7-day-old neonatal mice
- Separate, identify, and weigh neonatal mice.
- In a BSC, transfer the neonatal mice to a new cage to keep the mice away from the dam and to reduce stress to the dam.
- Remove and rub part of the nesting material with gloves to transfer the cage's smell to the gloves. Then, mold the nesting material into a smaller nest and place it into a new cage without the dam.
- Transfer the neonatal mice to the nesting material in the new cage.
- Transfer more nesting material to make a second, empty nest in the new cage.
- Close and remove the dam's cage from the hood so that the dam is not stressed from hearing any of the neonatal mice's distress.
- To track individual neonatal mice within the litter over time, use an ethanol-proof marker to mark one to five dots on the front or reverse of the tail, reapplying every 12-24 h as needed.
- Weigh each mouse that will be challenged, placing each into the secondary nest after weighing, and repeat this for all the mice.
- Return the entire litter to the dam before preparing the cecal slurry challenge aliquot.
- Calculate the individual weight-adjusted doses of cecal slurry and required dilution with D5W by completing this step for each litter separately, using the calculations below or using the provided worksheet (see Supplemental File).
- Calculate the milligrams of cecal slurry (a) to be administered to each mouse by multiplying the weight of the mouse in grams (b) by the desired challenge dose in milligrams of cecal slurry per gram of mouse (c).

- Calculate the individual volume of undiluted cecal slurry stock required per mouse in microliters (d) by dividing the milligrams of cecal slurry needed per mouse from step 3.2.1 (a) by the stock cecal slurry concentration, 160 mg of cecal slurry per milliliter of D5W (e), and multiplying by 1,000 µL per milliliter to convert from milliliters to microliters.

- Average the stock volume of cecal slurry required per mouse (g) by summing the volume of cecal slurry stock (d) per mouse in a litter of n mice, divided by the number of mice (n).

- Calculate the average dilution factor for the cecal slurry stock (h) by dividing the average injection volume (100 µL) by the average stock volume of cecal slurry required per mouse (g).

- Calculate each mouse's specific injection volume in microliters (j) by multiplying each mouse's volume of stock cecal slurry required (d) by the average dilution factor (h), and then round it off to the nearest ten (to match the 10 µL increments of the injection syringe).

- Calculate the average required volume of D5W to dilute the cecal slurry stock (k) by subtracting the average cecal slurry stock (g) from the average injection volume (100 µL).

- Calculate the total amount of cecal slurry stock in microliters (l) by multiplying the average stock cecal slurry per mouse in microliters (g) by the number of mice in this litter (n) and multiplying by 1.4 to create extra.

- Calculate the total amount of D5W in microliters (m) required to dilute the cecal slurry stock by multiplying the average required volume of D5W (k) by the number of mice (n) and multiplying by 1.4 to create extra.

- Calculate the milligrams of cecal slurry (a) to be administered to each mouse by multiplying the weight of the mouse in grams (b) by the desired challenge dose in milligrams of cecal slurry per gram of mouse (c).
- Prepare the challenge aliquot after calculating the amount of stock cecal slurry required (l from step 3.2.7). In a BSC, thaw the required number of cecal slurry stock vials at room temperature, pipetting its contents to mix.
- When there are no more visible ice crystals present in the thawed cecal slurry, transfer the calculated amount of cecal slurry stock (l from step 3.2.7) to a sterile 1.8 mL microcentrifuge tube.
- Dilute to the required concentration by adding ice-cold D5W as calculated in step 3.2.8 (m). Store the challenge aliquot on ice.
- Before loading the syringe, mix the microcentrifuge tube by flicking it 20x, followed by 3x of drawing up and expelling 300-500 µL of cecal slurry with a 500 cc 28 G ½ inch insulin syringe.
- Draw up roughly 150 µL of diluted cecal slurry into the same syringe.
- Flick the syringe to dislodge bubbles from the plunger, draw back slightly on the syringe, and then expel the bubbles.
- Dispense the excess cecal slurry back into the microcentrifuge tube until the correct amount of cecal slurry for one mouse, as was calculated for individual mice in step 3.2.5 (j), is loaded in the syringe.
- Intraperitoneally inject cecal slurry, according to relevant local animal care institution guidelines, or use the steps outlined below.
- In a BSC, separate the neonatal mice from the dam as described in step 3.1.
- Scruff the mouse by the back of the neck, using the thumb and index finger.
- Secure the mouse's tail across the back of the middle and ring fingers, or on the front of the ring and pinky fingers.
- To minimize leaks, tilt the neonatal mouse so that it faces downward and insert the needle bevel of the needle facing up, between the leg and the genitalia, keeping the needle shallow and subcutaneous.
- When the needle is inserted for 1 cm, press downward and forward to feel the needle puncture the peritoneum. Slowly depress the plunger, keeping the tip of the needle as steady as possible, as lateral movements could damage the mouse's organs.
- Carefully withdraw the needle over 5-10 s, following the same route out as in, relaxing the middle finger during the removal to reduce tension in the mouse's body.
- To check for leaks, hold the mouse for a few seconds after the removal of the needle, to allow time for the injection site to close, and observe any leakage or bulging at the injection site, at which point the mouse should not be used in the analysis.
NOTE: Bulging of the skin at the injection site indicates a failed intraperitoneal injection, with the injectant being subcutaneous. - Place the mouse on a paper towel and allow the mouse to take a step. If the mouse is immobile for 5 s, then lightly press the tail.
- Pick up the mouse and check for any leakage of cecal slurry at the injection site. If there is a leak, exclude the mouse from the analysis and euthanize the mouse.
4. Mouse monitoring
- Monitor the mice regularly to check them for arriving at a humane endpoint.
- Observe the mice 2 h postchallenge for any injection-related complications.
- Monitor the mice 12 h postchallenge for sepsis-related morbidity and the identification of mice at a humane endpoint (see steps 4.2-4.3 for criteria).
- Subsequently monitor every 4-6 h for the first 2 days, except for 8 h overnight, when the neonatal mice are unattended.
- Beyond 2 days postchallenge, monitor 1x-2x per day. If sick mice or mice whose health score decreases are observed, then increase the monitoring frequency to every 4-6 h.
- Monitoring neonatal mice
- For any procedure involving neonatal mice, transfer the bedding material to a new cage as described in step 3.1 (for the same reasons as mentioned there). Carefully check for any neonates that are dragged from the nest while nursing. Any mice that are dragged out of the litter while nursing should not be considered to be scattered mice.
- When removing the top of the nest, identify any scattering of neonatal mice either away from the nest or stuck in the nesting material but away from their littermates, with the exception of mice dragged away from the litter while nursing. Refer to the humane endpoint criteria in step 4.5 if a mouse is found scattered.
- Measure the mice's righting reflexes and mobility.
- On a paper towel, place a mouse on its back and monitor for its ability to right itself within a maximum of 4 s. When placed on its back, the mouse will fall to either the left or right side, which is when the 4 s count begins.
NOTE: To be classified into the "Rights" group, the mouse must be able to get at least three of four paw pads on the paper towel for 1 s. It is still grouped as being able to right itself if it falls over.- If the mouse can right itself, then wait for 8 s to determine its level of mobility.
- Categorize the mouse as "Rights-Mobile" if it can right itself and explore its environment by taking multiple steps in a row.
- Categorize the mouse as "Rights-Lethargic" if it can right itself and take a few steps to explore its environment. The mice in this group may fall over while taking a step, look shaky on their feet, and pause between steps.
- Categorize the mouse as "Rights-Nonmobile" if it can right itself but does not move around a lot. It may still fall over, and if it does not take any steps within 8 s, it is grouped as Rights-Nonmobile.
- If the mouse could not right itself, then categorize its mobility based on the observed hip movement.
NOTE: Avoid repeating the monitoring or increasing the length of time the mouse spends on their back because this could affect the scoring system and humane endpoint, as a mouse that fails to right itself within 4 s can sometimes do so if given more time.- Categorize the mouse as "Fail to right (FTR)-Mobile" if it is unable to right itself and displays hip movement that exceeds 90° angle from horizontal. Some mice can right themselves if given more than 4 s but should still be categorized as FTR, with mobility scores based on hip movement.
- Categorize the mouse as "FTR-Lethargic" if it is unable to right itself and displays hip movement below 90° angle from horizontal.
- Categorize the mouse as "FTR-Nonmobile" if it is unable to right itself and has legs that shake or vibrate but no hip movement. Limbs may extend or retract but do not have lateral movement. The mouse is visibly ill and has reached the humane endpoint.
- On a paper towel, place a mouse on its back and monitor for its ability to right itself within a maximum of 4 s. When placed on its back, the mouse will fall to either the left or right side, which is when the 4 s count begins.
- Repeat step 4.3 on the other side of the mouse, recording both sides.
NOTE: See the Supplementary File for recording observations. - Determine whether the mouse is at a humane endpoint and requires euthanasia as outlined in Table 1, and below.
- Categorize mice into different righting and mobility levels based on the monitoring observations noted in steps 4.3 and 4.4. The mouse's mobility is measured for each side, and the mobile behavior is used to determine whether the mouse requires euthanasia.
- Assign any mice with a righting reflex of either (a) FTR-Nonmobile or (b) FTR-Lethargic and found separated from the nest to be at a humane endpoint.
- In monitoring time points beyond 20 h postchallenge, classify any mouse with a righting reflex of "fail to right" on both sides as being at a humane endpoint, because the presented data predict with high accuracy that these mice eventually succumb to disease, and do not recover.
- Separate mice that are to be euthanized, as determined in step 4.5. If the monitored mouse is not seen as at a humane endpoint, place it into the second empty nest in the new cage without the dam, and continue with the other neonatal mice.
- Once the entire litter has been monitored, move half of the nesting material into the cage with the dam, reforming a nest with room in the middle for the neonatal mice.
NOTE: An improperly formed nest could cause the mice to scatter and reduce the amount of available care that the dam can offer. - Transfer the neonatal mice back into the cage with the dam.
- Enclose the litter in the nest by putting the leftover nesting material over the litter and gently pinching it around the lid to secure the nesting material in place.
- Euthanize the neonatal mice separated in step 4.6 according to local institution requirements.
5. Titration of the cecal slurry
- Challenge the mice at the desired challenge dose (section 3) and monitor the outcomes (section 4).
- Observe whether the final outcome results in the desired LD, and if not, repeat sections 3 and 4 with a new litter at a higher or lower challenge dose, adjusting it by 5%-10%.
NOTE: Challenge doses may be similar to Figure 1B but need to be titered in each facility and strain of mice. - Also, observe whether the mice achieve a humane endpoint faster or slower than the expected kinetics in Figure 1B, and repeat sections 3 and 4 with a new litter at a higher or lower challenge dose, adjusting it by 5%-10%.
Cecal slurry viability stored at -80 °C can be tested over time by serially diluting and plating aliquots of cecal slurry stock on 5% sheep's blood tryptic soy agar followed by 24 h of aerobic incubation at 37 °C. Subsequent counting of culturable colony-forming unit (CFU) content of a cecal slurry preparation was found not to change over a 6 month period, and the viability was not affected by prolonged storage at -80 °C (Figure 2). Each donor mouse resulted, on average, in enough cecal slurry to challenge three to four litters (data not shown).
Mice challenged at DOL 7 with cecal slurry to induce polymicrobial sepsis began to reach the humane endpoint within 12 h of the challenge, and polymicrobial sepsis was mostly resolved by 48 h postchallenge, as observed in a Kaplan-Meier survival curve combined from data from over 200 challenged mice (Figure 1A). The lethality was dependent on the challenge dose administered, with a 5% change in challenge dose resulting in a roughly 15% difference in survival rate (Figure 1B). The mouse body weight was measured at each monitoring visit. Weight loss was seen in all challenged animals, being nondiscriminatory between mice that ended up surviving and those that did not during the initial 24 h postchallenge (Figure 1C). After 24 h, most surviving animals began to regain their weight, while all nonsurvivors continued to lose weight and moved to their humane endpoint. However, a small proportion of surviving animals that had retained their righting reflex also continued to lose weight or failed to gain weight, until the end of the experiment, even losing as much as 20% of their initial body weight within 40 h of the challenge. As there was an overlap of weight loss between mice that ended up surviving and those that did not, the change in weight or a threshold of weight loss could not be used as a criterion for humane endpoint while still maintaining the goal of accurately dividing survivors from nonsurvivors.
The behavior of mice was monitored as outlined in the protocol and in Table 2. Snapshots of the health categories are displayed (Figure 3A-C). These photos show the different health categories of mice who failed to right themselves after being placed on their back and outline the difference between FTR-Mobile and FTR-Lethargic, which is an important distinction. Unchallenged healthy mice of this age do not display FTR-Lethargic activity; therefore, this health category is a marker of disease and a response to challenge. Sick mice displayed FTR-Lethargic symptoms (Figure 3B) and could regress toward FTR-Nonmobile (Figure 3C), where the upper leg remains parallel with the bottom leg, with little to zero hip rocking movement, which is one of the criteria for humane endpoint. The mice might also recover, gaining increased hip movement and becoming FTR-Mobile (Figure 3A). The righting reflex and mobility scores were determined for both the left and right side of each mouse, and the highest score was utilized to determine whether the mouse had reached a humane endpoint. Behavioral information was collected from over 240 animals challenged with a lethal dose 60 (LD60) of cecal slurry, and 144 humane endpoints were observed (Figure 3D-F and Table 1). This evidence-driven approach was used to define and refine the humane endpoint across four disease stages, categorized by the experimenters based on both behavioral differences between survivors and nonsurvivors and by the fraction of humane endpoints reached during each time frame. During early experiments, FTR-Nonmobile mice that had no hip movement were consistently found dead within 4-6 h of this behavior being observed. In the collection of the presented information, an FTR-Nonmobile health score was used as criterion for a humane endpoint. From 12-21 h postchallenge, while FTR-Nonmobile mice were euthanized, both surviving and nonsurviving animals displayed very similar behavioral patterns and could not be distinguished in any other way (Figure 3D). From 21-48 h postchallenge, the majority of surviving mice regained their righting reflex, while fewer than 1% of the FTR behaviors observed were in animals that would go on to survive the experiment (Figure 3E). Thus, mice that failed to right themselves from both sides became an additional criterion for humane endpoint during this time. Between 12 and 20 h postchallenge, 12.5% of the total number of humane endpoints were observed, versus 80.5% between 20 and 48 h, and 7% after 48 h (Table 1). A distinguishing feature between mice that ended up surviving and that eventually worsened to a humane endpoint was the loss of the righting reflex, independent of hip mobility (Figure 3F). Indeed, between 20 and 48 h after the challenge, a total of 121 mice had failed to right themselves from both sides, with 116 of these mice eventually progressing to a humane endpoint (which represents a 96% accuracy in identifying mice that would not recover). Beyond 48 h after the challenge, 11 mice were observed to fail to right themselves from both sides, and 10 of these progressed to a humane endpoint (a 91% accuracy). Beyond 20 h after the challenge, the number of mice that lost the righting reflex for both sides predicts the final outcome with an accuracy of more than 90%; therefore, this has been added to the humane endpoint criteria, to identify nonrecovering mice earlier and reduce mouse suffering (Table 1).
The frequency that mice need monitoring changes over time, due to different rates of death postchallenge, and is outlined in Table 1. A mouse was considered to be at its humane endpoint at any point if it had failed to right itself and displayed nonmobile hip movement on both sides, or if the mouse was found scattered from the nest, was unable to right itself, and had lethargic hip movement. Mice with either of these conditions were not expected to be able to rejoin the litter and have been observed to be FTR-Nonmobile within 4-6 h. Starting 20 h after the challenge, a new humane endpoint was added because the presented information shows that the vast majority of mice that FTR from both sides ends up succumbing to disease.
The videos, tables, and resources presented in this manuscript are an effective teaching resource for the correct behavioral assignment of challenged mice. Seven experimenters were asked to watch the training video and read both the protocol and the tables before assigning behaviors to 60 challenged animals. The identification of humane endpoint assignment was accurate both for distinguishing FTR-Nonmobile mice from mice that displayed the other behaviors (Figure 4A) and FTR mice from mice that were able to right themselves within the allowable time frame (Figure 4B).
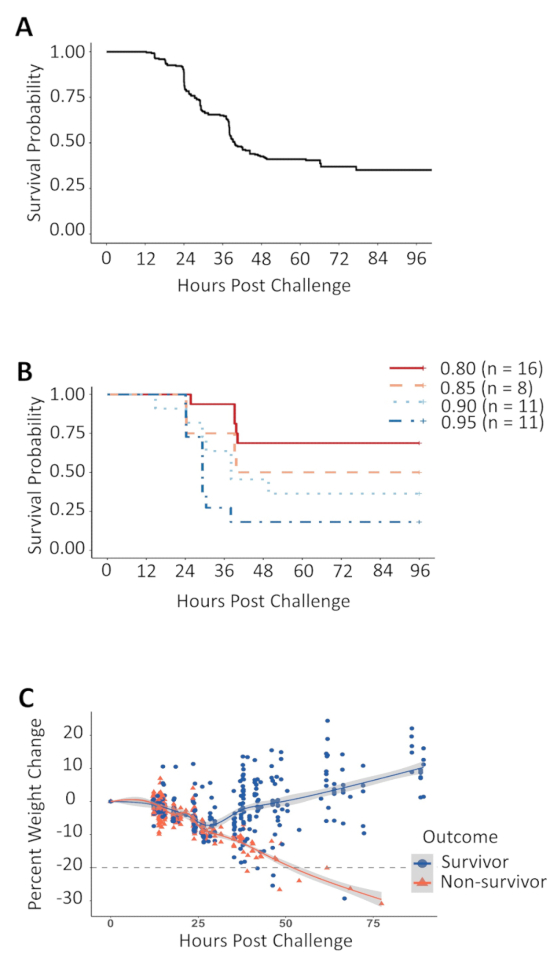
Figure 1: Kaplan-Meier survival curve, cecal slurry dose titration, and weight change following the cecal slurry challenge. (A) Survival outcome of neonatal C57BL/6J mice challenged with an intraperitoneal cecal slurry injection at DOL 7. The data for this figure were combined from independent experiments using multiple challenge doses, ranging from 0.7 to 1.3 mg of cecal slurry per gram body weight was administered to these mice. (B) Neonatal mice challenged with 0.80 to 0.95 mg of cecal slurry per gram body weight from one cecal slurry preparation display a dose-dependent relationship between the amount of cecal slurry given and the percentage of survival.(C) The percentage of change in weight compared to the challenge weight, with the dotted line denoting a 20% loss of weight from the time of the challenge. Please click here to view a larger version of this figure.
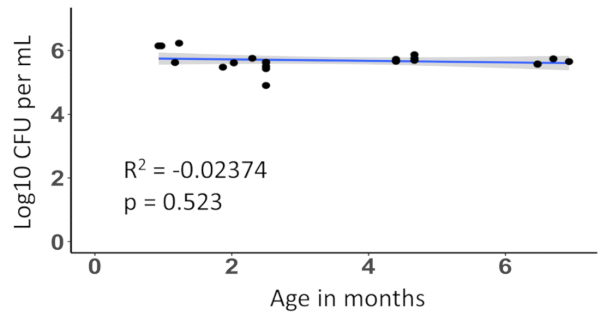
Figure 2: CFU concentration in cecal slurry stock stored at -80 °C does not change over a 6 month period. The effect of the cecal slurry age on CFU concentration was tested using linear regression. Each point represents one aliquot of the same cecal slurry preparation, serially diluted and plated over a 6 month period. Please click here to view a larger version of this figure.
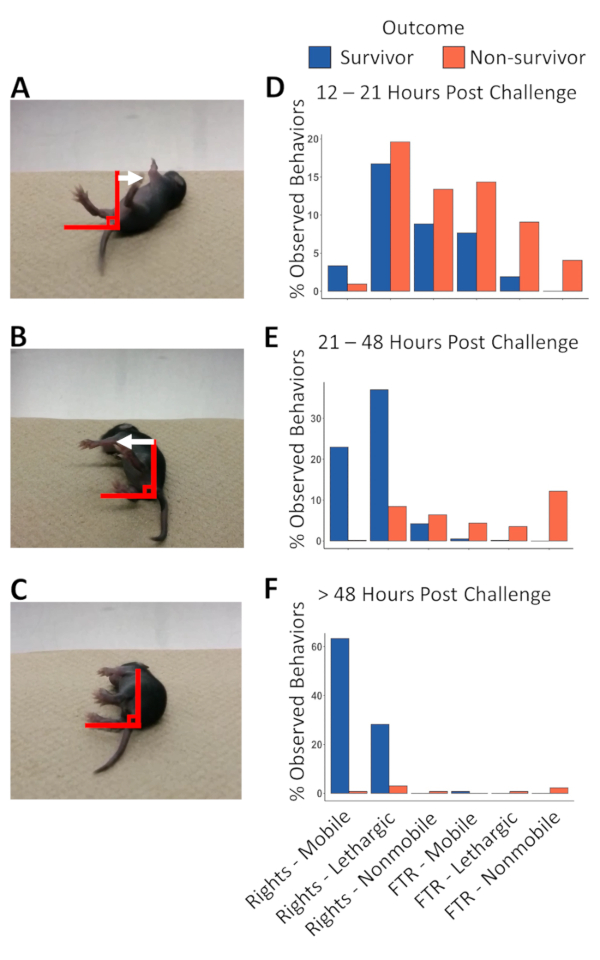
Figure 3: Hip mobility categories of mice that fail to right themselves and of animal behaviors at various times postchallenge. Mice that have been challenged with sepsis, when placed on their back, will display signs of morbidity that can be measured by the degree of hip movement. (A) A fail to right (FTR)-Mobile mouse shows hip rocking movement of their upper leg exceeding 90° angle from horizontal. (B) An FTR-Lethargic mouse shows hip rocking movement but does not exceed 90° angle from horizontal at any point during the 4 s of monitoring. (C) Some FTR-Nonmobile mice will extend their leg, bending at the knee, but will show very little (less than 10° angles) to zero hip rocking movement, and the legs will remain parallel to each other. (D) Animal behaviors 12-21 h postchallenge show that only FTR-Nonmobile behaviors separate survivors from nonsurvivors. (E) From 21 to 48 h postchallenge, only 4 out of the 592 observed FTR behaviors (0.67%) belong to survivors, allowing the righting reflex to predict the final outcome and be used as a new criterium for humane endpoint. (F) Beyond 48 h postinfection, 6 out of 131 mice (4.55%) that had a righting reflex went on to become part of the FTR group and were sacrificed by the end of the experiment, justifying sustained monitoring throughout the course of recovery. Please click here to view a larger version of this figure.
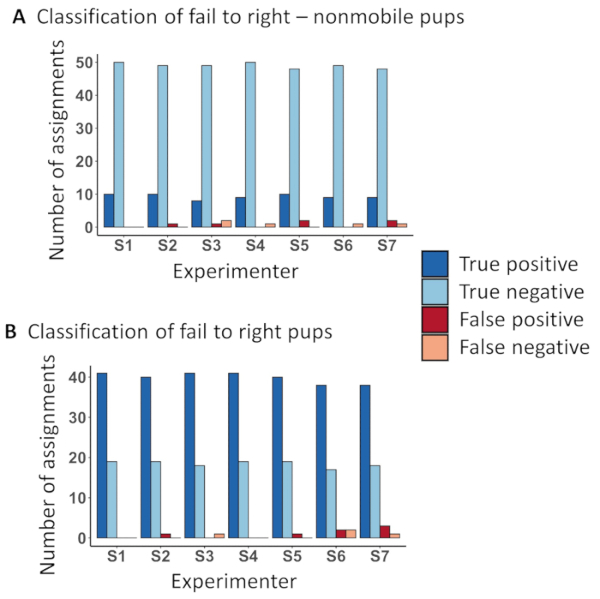
Figure 4: Instructional resources result in accurate behavioral classification by independent experimenters. Experimenters trained by watching video accompanying this protocol categorized videos of 60 neonatal mice into different health groups. (A) The ability to distinguish a humane endpoint was determined and an average of 97% of behaviors was accurately categorized as FTR-Nonmobile or not, while only 1% of FTR-Nonmobile mice were misidentified. Two percent of the mice were falsely identified as FTR-Nonmobile. (B) The identification of the second humane endpoint criterium of correctly distinguishing between FTR mice or those having the ability to right themselves within 4 s of being placed on their back was assigned correctly in 97% of the scorings, while only 0.96% of the mice were incorrectly assigned as righting themselves and 2% of mice were incorrectly assigned as FTR. Please click here to view a larger version of this figure.
| Disease Stage | A: High morbidity, no mortality | B: High morbidity, low mortality | C: High morbidity, high mortality | D: Low morbidity, low mortality |
| Hours post challenge | 0−12 | 12−20 | 20−48 | >48 |
| Monitoring frequency | 2 h post challenge | every 4−6 h | Every 4−6 h, 8 h, unattended overnight | 1−2 times daily, more if needed |
| Proportion of total humane endpoints observed | 0/144 | 18/144 | 116/144 | 10/144 |
| Percentage of humane endpoints observed | 0% | 12.5% | 80.5% | 7% |
| Humane endpoint criteria | 1. FTR−Nonmobile on both sides | 1. FTR−Nonmobile on both sides | ||
| 2. Scattered from nest and is FTR−Lethargic | 2. Scattered from nest and is FTR−Lethargic | |||
| 3. FTR on both left or right side (with any mobility score) | ||||
Table 1: Frequency of monitoring and humane endpoint criteria in the different stages of disease. Monitoring frequency, humane endpoints observed, the percentage of humane endpoints, and humane endpoint criteria during different stages of disease.
| Righting Reflex | Mobility | Time limit to right after being placed on back | Time limit to measure amount of movement (mobile / lethargic / nonmobile) | Mobility scoring Criteria |
| Rights | Mobile | 4 s | An additional 8 s | The mouse takes multiple steps in a row, maintaining forward momentum, and explores its environment. Pup will not fall over. |
| Lethargic | The mouse can take a step but will stop and pause before taking another. Pup may fall over. | |||
| Nonmobile | The mouse does not take any steps after righting itself. Pup may fall over. | |||
| Fail to right | Mobile hips | The same 4 s used to measure righting reflex | Has energetic hip movement with the upper leg rotating beyond 90° from horizontal at least once within 4 s. | |
| Lethargic hips | Hip movement up to but not beyond 90° from horizontal. | |||
| Nonmobile hips | Limbs may move by extending and retracting but the hips will not rotate. Pup looks very sickly. |
Table 2: Monitoring table and criteria in determining the health score of mice. The provided criteria were used to define health category groups to mice, and to reduce individual variance in assigning health scores.
