The establishment of a dual humanized mouse model with human liver and immune cells can be easily monitored at each step with very simple ELISA and flow cytometry, respectively. Flow cytometry is regularly performed to evaluate the development of a functional immune system and to see the effect of HIV infection on immune cells. In dual humanized mice, the development of functional immune cells can range from 15% to 90% of the lymphocyte gate. Representative subsets of immune cells are shown in dot plots (Figure 3). For the evaluation of the engraftment of human hepatocytes, ELISA for human-specific albumin levels is performed monthly on mouse serum. Mice engrafted with both HSPCs and HEPs show human-specific albumin levels ranging from ~7 µg/mL to 377 µg/mL at one month, continuing to grow over the time of observation (6 months) (Figure 4). The effect of HIV infection on human immune cells in the blood of dual humanized mice is monitored by flow cytometry and on HEPs in the liver by human-specific albumin ELISA. By 5 weeks, HIV-1 causes a decrease in human albumin levels in the serum, as assessed by ELISA, and there is a depletion of human CK18+ hepatocytes in the liver sections of dual humanized mice, as evaluated by immunohistochemistry (Figure 5). A lower ratio of CD4:CD8 is typically observed, by flow cytometry, in the blood and liver of HIV-infected mice, compared to levels noted in the same mouse before infection (Figure 6). All reagents and materials important for the protocol are discussed in the Table of Materials.
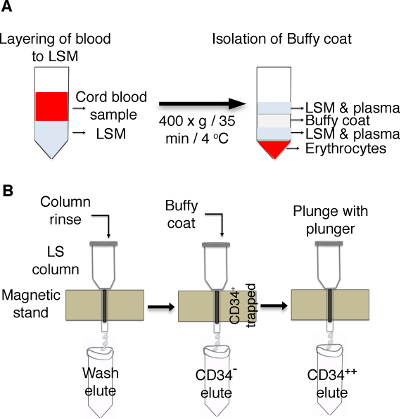
Figure 1: Schematic of the enrichment of CD34+ cells from cord blood. (A) Cord blood is layered on lymphocytes separation medium (LSM) and centrifuged to isolate buffy coat. (B) LS columns are placed on a magnetic stand and rinsed with BSA buffer, followed by adding buffy coat. Cells positive for CD34 are trapped in the columns, and CD34– cells are eluted in separate tubes. Trapped CD34+ cells in column resins are plunged with a plunger, and the cells are collected in a new tube. Please click here to view a larger version of this figure.

Figure 2: Schematic view of the experimental design for the dual reconstitution of humanized liver and immune system mice, followed by HIV-1 infection. TK-NOG mice are injected with ganciclovir (GCV) at a dose of 6 mg/kg, 2x a day, on day -7 and day -5, followed by a treosulfan injection on days -3, -2 and -1. To screen the mice for the transplantation (Tx), an alanine aminotransferase (ALT) assay is performed one day before the surgery, and mice with ALT levels of >200 and <600 U/L are selected. After transplantation, the mice are checked for a reconstitution of the human immune system by flow cytometry (FACS) and for liver reconstitution by assessing their albumin level using ELISA. The mice are infected with HIV-1 5 weeks before they are sacrificed. Please click here to view a larger version of this figure.
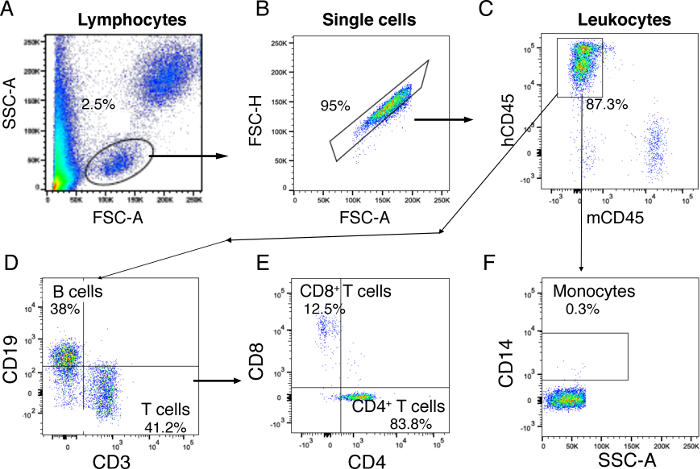
Figure 3: Flow cytometry analysis gating strategy for the human cell distribution of blood. (A) First, lymphocytes are gated on whole blood based on FSC-A and SSC-A. (B) Single cells are gated on lymphocytes. (C) Human CD45+ leukocytes are gated on single cells using mouse CD45 and human CD45. (D) CD3+ T cells and CD19+ B cells are identified on gated CD45+ human leukocytes. (E) CD4+ T helper cells and CD8+ cytotoxic T cells are identified in gated CD3+ T cells. (F) CD14+ monocytes are gated from human CD45+ leukocytes. The results represented here are from one mouse transplanted with dual human hepatocytes and HSPCs. Please click here to view a larger version of this figure.
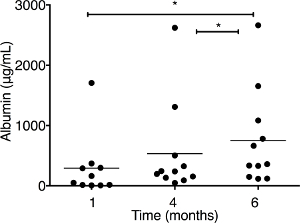
Figure 4: Albumin concentration is measured by ELISA in the serum of dual humanized mice. The mice are transplanted with both human hepatocytes (HEPs) and CD34+ hematopoietic stem/progenitor cells (HSPCs) (n = 11). Serum is collected at different times at 1, 4, and 6 months posttransplantation, and dilutions are made to adjust the unknown sample concentrations in the range of standards. Each symbol represents an individual mouse value. The results represent the median, as well as individual values. * P < 0.05, by one-way ANOVA. This figure has been modified from Dagur et al.8. Please click here to view a larger version of this figure.
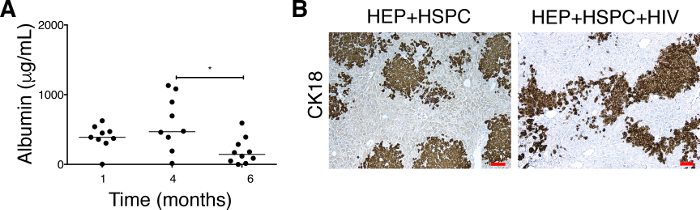
Figure 5: Effect on HIV-1 on albumin levels in serum and the depletion of CK18+ human hepatocytes in the liver of dual humanized mice. (A) Albumin concentrations are monitored in uninfected mice (n = 9) transplanted with both human HEPs and HSPCs at 1 and 4 months. The mice are infected (n = 10) with HIV at 4 – 5 months posttransplantation and sacrificed 5 weeks postinfection. Each symbol represents an individual mouse value. The results represent the median, as well as individual values. * P < 0.05, by one-way ANOVA. This figure has been modified from Dagur et al.8. (B) Five-micron liver sections from uninfected (HEPs + HSPCs, left panel) and HIV-infected TK-NOG mice (HEPs + HSPCs + HIV, right panel) are fixed, paraffin embedded, and stained for anti-human cytokeratin-18 (CK18) antibody. HIV-1 causing a depletion of CK18+ hepatocytes is evidenced by a less occupied area by the CK18+ human cells. The results represented here are from one uninfected and one HIV-infected mouse transplanted with dual human hepatocytes and HSPCs. Scale bars = 100 µm. Please click here to view a larger version of this figure.
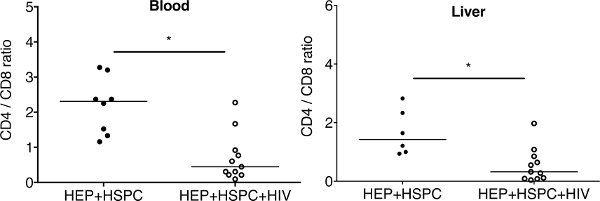
Figure 6: Ratio of CD4+ cells to CD8+ T cells in peripheral blood and in the liver of dual reconstituted uninfected and HIV-1-infected mice. For dual reconstituted uninfected mice: closed circle; HEPs + HSPCs; blood n = 7; liver n = 6. For HIV-1 infected mice: open circles; HEPs + HSPCs + HIV; blood n = 10; liver n = 11. The results represent the median, as well as individual values. * P < 0.05, by one-way ANOVA test between HIV-infected and uninfected mice. This figure has been modified from Dagur et al.8. Please click here to view a larger version of this figure.
