To assess the impact of biopsy on brain tumor cell behavior, we performed the procedure described in this protocol. Glioma—GL261 cells—expressing a nuclear fluorescent protein (H2B-Dendra2) were injected in the brain of C57BL/6 mice, and a chronic CIW was implanted. Time-lapse intravital imaging was performed on the same animal pre- and post-biopsy-like injury to the tumor (Figure 1A,B). The migration of individual tumor cells was determined by tracking the migration path over time in different xy planes of the z-stack (Figure 1C) and plotted as a percentage of migratory cells pre- and postbiopsy (Figure 1F). The tumor cell proliferation rate was quantified based on H2B-tagged Dendra2 condensation upon mitosis (Figure 1D) and plotted as a percentage of dividing cells pre- and postbiopsy (Figure 1E). We compared the distribution of migration velocity before and after biopsy in the same tumor and found that the number of migratory cells (velocity > 4 µm/h) increased after the intervention, with an associated decrease in the number of slow-/nonmigratory cells (velocity < 4 µm/h) (Figure 2A). On average per tumor, we observed a 1.75 (SD = 0.16)-fold increase in the percentage of migratory cells when a biopsy-like injury was performed, compared to control mice that were not biopsied (Figure 2B). We monitored tumor cell behavior for another week and found that, although the percentage of migratory tumor cells eventually decreased in both the control and the biopsied mice, the biopsied mice still exhibited a higher migratory capacity than the control mice (Figure 2C). The analysis of tumor cell proliferative behavior over time showed a 1.52 (SD = 0.26)-fold increase in the number of mitotic events upon biopsy, relative to nonbiopsied control mice (Figure 2D).
To test whether the observed effects of biopsy on tumor cell proliferative and migratory behavior was an artifact due to CIW replacement surgery (required to perform a biopsy-like injury), we monitored tumor cell behavior in a group of mice that underwent CIW replacement without a biopsy. In this group, we did not observe any induction of migration or proliferation of tumor cells, indicating that the boost in tumor cell proliferation and migration rates were specifically triggered by biopsy-like injury (Figure 3A, B).
Stable photo-convertibility of the fluorescent protein Dendra2 allows for studying tumor cell infiltration over several days. Upon exposure to ultraviolet/blue light, Dendra2 is irreversibly switched from green to red. Using this property, a square region of the tumor was illuminated and ~200 Dendra2-expressing tumor cells were photo-marked before biopsy (Figure 4). One day after the biopsy, we relocalized the photo-switched region and measured the volume of tumor cells that had infiltrated into the surrounding tumor tissue. We found that the infiltration area was 1.72 (SD = 0.41) times larger in tumors after a biopsy-like injury compared to nonbiopsied control tumors (Figure 4). Although this approach only provides information on tumor cell bulk infiltrative behavior and not on a single cell level, it is less time-consuming than the time-lapse imaging approach and can be the method of choice for research questions focused exclusively on studying infiltrative behavior.
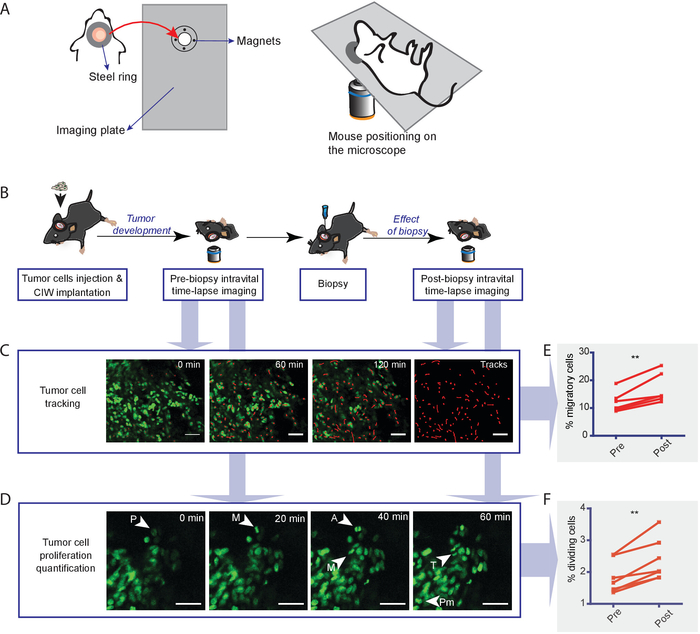
Figure 1: Experimental setup for longitudinal intravital imaging of the biopsy effect on tumor cell behavior. (A) Diagram showing the design of the ring and the magnetic holder. (B) Schematic representation of the experimental workflow. Tumor cells are injected into the brains of mice and a CIW is established. Upon tumor development, a first (prebiopsy) time-lapse imaging session is performed. The next day, the biopsy and CIW replacement are implemented. The day after imaging (postbiopsy), a second time-lapse imaging session is performed. For long-term effects, subsequent imaging sessions can be done. (C) Images show representative snapshots of a time-lapse movie where GL261 H2B-Dendra2 tumor cells were tracked. Red lines depict individual tumor cell tracks. The scale bar = 50 µm. (D) Representative in vivo time-lapse images displaying dividing cells in GL261 H2B-Dendra2 tumors. Different stages of mitosis are indicated: prophase (P), prometaphase (Pm), metaphase (M), anaphase (A), and telophase (T). The scale bar = 50 µm. Graphs indicate the percentage of (E) migratory and (F) dividing cells pre- and postbiopsy. Each dot indicates the percentage of migratory cells in all the positions measured in an individual animal. The data are shown as mean ± S.E.M. of six mice (**P < 0.01, paired t-test). This figure has been modified from Alieva et al.4. Please click here to view a larger version of this figure.
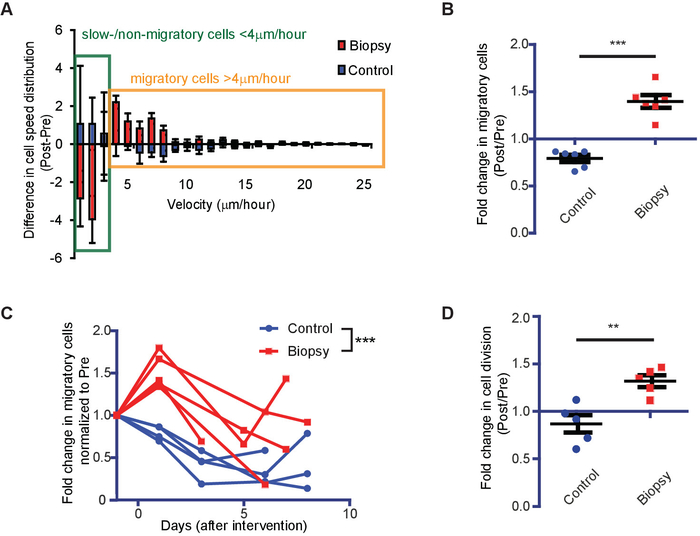
Figure 2: Representative results showing the impact of biopsy on tumor cell migration and proliferation rates. (A) Waterfall plots showing the change in cell velocity distribution relative to basal migration in individual mice. The data are shown as mean ± S.E.M. of five mice. (B) The number of migratory cells in control (blue) and biopsied (red) animals normalized to the number of migratory cells preintervention (n = 6 mice, ***P < 0.0001, Student's t-test). (C) Tumor cell behavior was tracked over several days. Shown are the normalized (relative to preintervention) number of migratory cells in individual mice over time (n > 4 mice per condition, ***P < 0.0001, two-way ANOVA). (D) The normalized number of dividing cells in control (blue) and biopsied (red) animals. Per individual animal, the values postintervention were normalized to the values preintervention (n = 5 mice, **P < 0.01, Student's t-test). This figure has been modified from Alieva et al.4. Please click here to view a larger version of this figure.
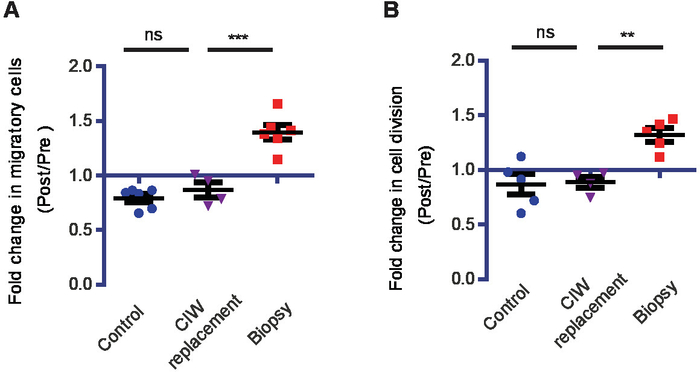
Figure 3: CIW replacement has no effect on tumor cell behavior. Longitudinal intravital imaging shows that the replacement of the CIW without biopsy has no effect on migration and proliferation rates. (A) The increase in the number of migratory cells for the indicated conditions. Every symbol represents the mean of an individual mouse, and n≥ 4 mice. (B) The increase in the number of proliferating cells for the indicated conditions. Every symbol represents the mean of an individual mouse (n≥ 4 mice, **P < 0.01,***P < 0.001, ns = nonsignificant, one-way ANOVA with Newman-Keuls post hoc test). This figure has been modified from Alieva et al.4. Please click here to view a larger version of this figure.
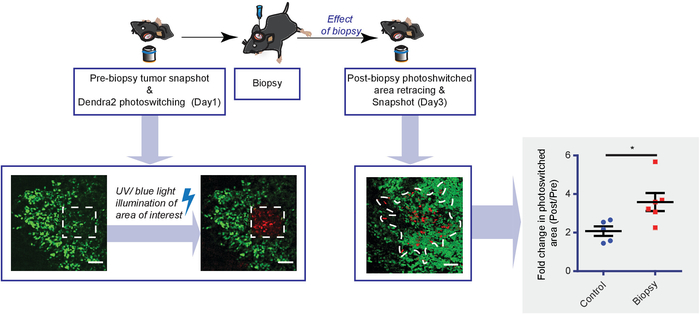
Figure 4: Diagram showing the experimental setup and representative results obtained with Dendra2 photo-switching. To monitor tumor cell infiltration upon biopsy, Dendra2-expressing tumor cells are photo-switched in a square region by UV/blue light illumination and imaged, 1 day before the biopsy. One day after the biopsy, the photo-switched region is relocalized and reimaged. Shown are representative Dendra2 images of tumor cell infiltration, corrected using channel subtraction. The white dotted line represents the infiltration area. The scale bar = 50 µm. The graph shows the increased photo-switched area plotted for biopsied (red) and control (blue) mice. Every dot represents the mean value of an individual mouse (n≥ 5 mice, *P < 0.05, Student's t-test). This figure has been modified from Alieva et al.4. Please click here to view a larger version of this figure.
