The rat VCA heterotopic hindlimb osteomyocutaneous flap model allows for long-term allograft survival under immunosuppression. The model is reliable, reproducible, and simple to perform. The flap is well hidden in the groin area and constitutes minimal morbidity and discomfort to the animal. The skin presentation is a clinical manifestation of the allograft’s survival and rejection (Figure 1). The flap design allows for gross clinical monitoring and creates an opportunity for various imaging techniques, such as laser Doppler (Figure 2). Serial biopsies of the skin, muscle, and arteries make it possible to achieve histopathological follow-up and analysis at different rejection stages (Figure 3).
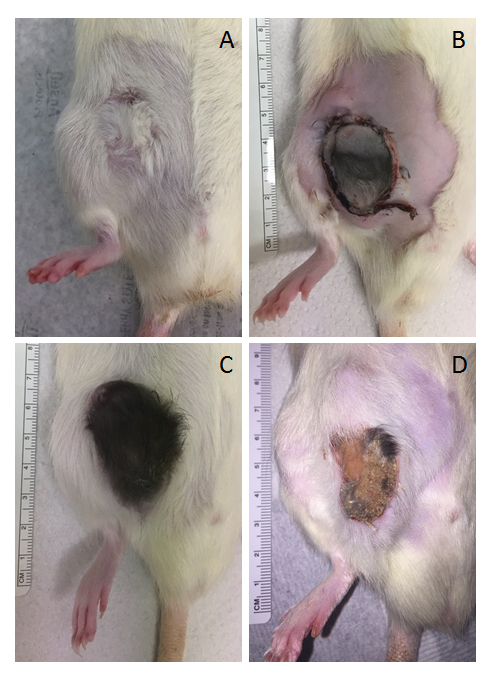
Figure 1: Representative images from transplanted animals. (A) Syngeneic VCA long-term survival, without immunosuppression treatment, on postoperative day 45 (POD 45); note the difference in direction of fur growth due to the graft’s inverted orientation. (B) Allogeneic VCA, treated daily with an immunosuppressant drug, on POD 5. (C) Allogeneic VCA long-term survival, treated daily with an immunosuppressant drug, on POD 40; note normal fur growth indicating proper perfusion of the graft, without signs of rejection. (D) Allogeneic VCA in rejection on POD 33. Immunosuppression treatment was stopped completely on POD 14; note the clinical signs of rejection (skin atrophy, desquamation, loss of fur). Please click here to view a larger version of this figure.
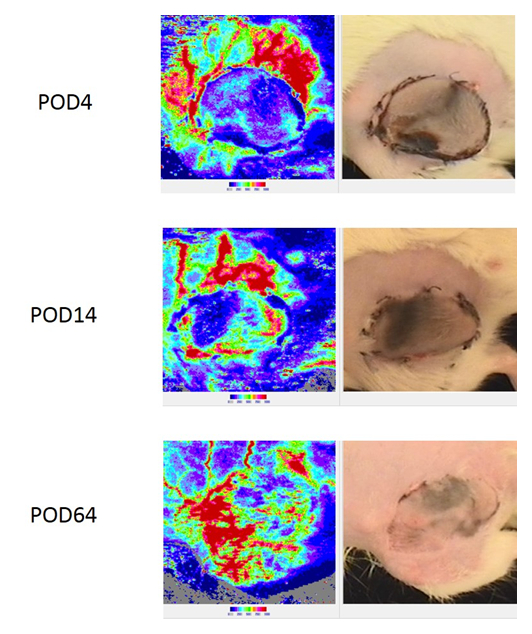
Figure 2: Laser Doppler imaging system to monitor superficial skin revascularization of the allograft. The allograft presented was monitored on postoperative days 4, 14, and 64. The panels on the left show blood perfusion as measured by Doppler imaging, while the panels on the right show the area being imaged by the Doppler. Note the shift from minimal blood perfusion immediately post-VCA to full revascularization of the flap on day 64. This allograft was kept under proper immunosuppression without signs of rejection. Please click here to view a larger version of this figure.
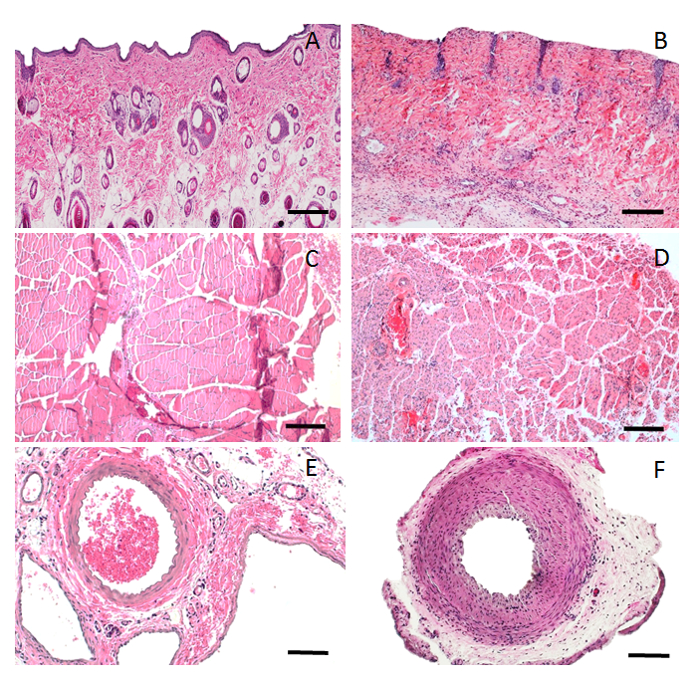
Figure 3: H&E histopathology of allograft in syngeneic vs. allogeneic transplants. (A) Skin biopsy of a syngeneic allograft on POD 45 (10x magnification); note the normal morphology of the skin components (epidermis, adnexa, and no sign of mononuclear cell infiltration). (B) Skin biopsy of an allogeneic allograft in rejection on POD 75, treated daily with a lower dose of an immunosuppressant (10x magnification); note epidermal atrophy, adnexa atrophy, mononuclear cell infiltration, perivascular infiltration, and capillary thrombosis. (C) Muscle biopsy of a syngeneic allograft on POD 45 (10x magnification); note the normal morphology of the striated muscle. (D) Muscle biopsy of an allogeneic allograft in rejection on POD 98, treated daily with a lower dose of an immunosuppressant (10x magnification); note the muscle atrophy and mononuclear cell infiltration. (E) Femoral artery biopsy of a syngeneic allograft on POD 45 (20x magnification); note the normal morphology of the artery. (F) Femoral artery biopsy of an allogeneic allograft in rejection on POD 98, treated daily with a lower dose of an immunosuppressant (20x magnification); note the intimal hyperplasia, narrow lumen, and perivascular infiltration. Scale bar = 200 µm (A–D); 100 µm (E and F). Please click here to view a larger version of this figure.
