We adopted the TNBS colitis mouse model to study and elucidate the underlying mechanisms of intestinal fibrosis8. Here, we performed a detailed time course study of TNBS-mediated colitis, where TNBS was rectally administrated weekly to wild type mice for up to six weeks as represented schematically (Figure 1A). After six weeks of TNBS treatment, we noticed that colonic lengths shorten progressively over the course of the TNBS treatment, from an average of 5 ± 0.5 cm in the control group to 3 ± 0.5 cm in the TNBS group; such quantitative analysis of colon length represents a very apparent reduction in colon length (Figure 1B). To ensure that the TNBS Crohn's disease model is comparable to the human Crohn's fibrosis model and was not an artifact related to the methodology, we analyzed the fibrotic markers at multiple levels in a detailed time course study for the TNBS injection to the wild type. Accumulation of alpha-smooth muscle actin (αSMA) positive cells and collagen deposition within submucosal layers have been reported in most of the fibrosis incidences and is regarded as a hallmark for fibrotic events14. We found that the colon sections of TNBS-treated mice that were stained with αSMA showed a 4-6-fold increase in colonic submucosa layer positively stained with αSMA (Figure 1C). Besides, the Trichrome blue staining for these sections also showed a 2-4-fold increase, suggesting significant collagen deposition, which validates severe intestinal fibrosis (Figure 1D). We further assessed the activation of myofibroblasts by detecting αSMA-positive cells by FACS analysis in TNBS-treated mice colon and found a significant accumulation of αSMA-positive staining (Figure 1E). Furthermore, we found substantial induction in the expression of αSMA, Col-I, and Col-III measured by qPCR analysis in TNBS-treated mice (Figure 1F). Increased expression of αSMA protein in western blot analysis revealed increased fibrosis (Figure 1G). Overall, TNBS kinetics treatment provides an opportunity to access putative immune response in chronic conditions, which closely mimics the CD chronic phase condition and is essential to fibrosis development.
To compare TNBS fibrosis with Crohn's associated fibrosis, we analyzed the expression of fibrosis markers and cytokines in fresh tissue biopsy from the ileum of patients with active CD or under remission. Remarkably, we found marked induction of thickening of αSMA-positive layers and increased collagen deposition as detected by trichrome staining in active CD sections (Figure 2A). We also performed Western blot analysis and confirmed the induction of αSMA expression in active CD samples (Figure 2B). In addition, we observed significant induction of fibrosis markers including αSMA, Col1, as detected by qPCR analysis (Figure 2C).
Next, to determine a mechanism to limit TNBS fibrosis we evaluated the effects of rapamycin, a pharmacological inhibitor of mTOR activity15,16. Accordingly, we treated mice with both TNBS and rapamycin and analyzed αSMA and collagen level in colon histology and have shown quantitative measurement of αSMA and collagen in densitometry plot (Figure 3A). Our data suggests that rapamycin reduces the αSMA-positive staining in submucosal layer and lessens the collagen deposition. To further validate and quantify fibrotic responses, we determined the αSMA, collagen and TGFβ expressions by qPCR, and αSMA expression by flow cytometry in TNBS-treated colon (Figure 3B, 3C). We have also shown Cx3Cr1+ mononuclear phagocytes induce an inflammatory immune response to injury9. Thus, we wanted to see if administration of rapamycin in TNBS-treated mice could reverse the inflammatory and fibrotic effects. Therefore, we purified Cx3Cr1+ resident mononuclear phagocytes from colonic single cell suspensions by using magnetic microbeads (Figure 3D). We found an increased level of p-p70 and p-S6 in Cx3Cr1+ resident mononuclear phagocytes by western blot analysis from TNBS-treated mice, and this level was blocked by rapamycin (Figure 3E). Besides, we found that rapamycin treatment dampens down the IL-23 and IL-1β in the TNBS-treated group (Figure 3F). Moreover, these findings elucidate the effective mechanism involved in the induction of TNBS-fibrosis and have shown that rapamycin attenuates the induction of fibrosis.
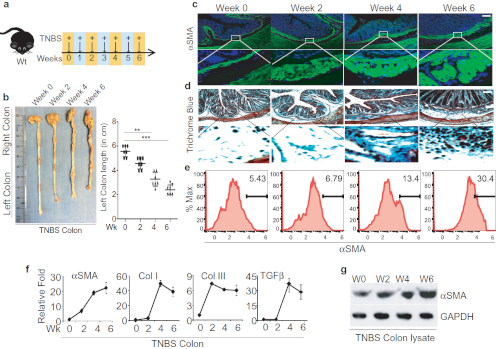
Figure 1: Successful TNBS administration leads to developing intestinal fibrosis in mice. A. Schematic diagram representation of weekly TNBS treatment given to wild-type mice. B. Colon images and measurement of colon lengths from TNBS-treated mice, harvested on weeks 0, 2, 4, and 6 post-TNSB treatment. C-D. Colon sections' histological analysis stained with anti-αSMA antibody for activation of myofibroblasts and trichrome blue staining for collagen; scale bar 100 µm. E. FACS analysis to identify αSMA-positive cells in the colon and quantification of αSMA-positive cells. F. Fibrotic markers and cytokines detected by qPCR. G. western blot analysis of αSMA from colon lysate of TNBS-treated and control mice. This modified figure is being reused with the permission of previous publication9 in Mucosal Immunology, 2019 by Mathur et al. Please click here to view a larger version of this figure.
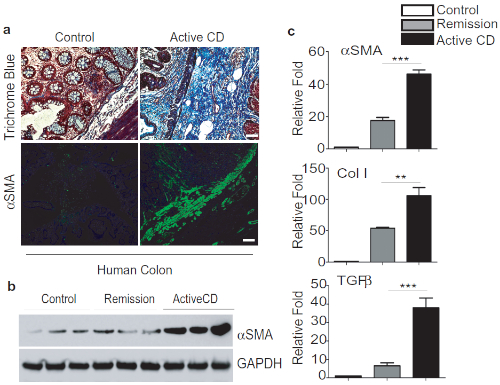
Figure 2: TNBS Fibrosis is comparable to Crohn's-associated Intestinal fibrosis. A. Representative images of colon biopsies of control, active CD showing a significant increase of trichrome blue staining and αSMA-positive staining in submucosal layers, scale bar 50 µm. B. Western blot analysis of αSMA expression and quantification. C. qPCR analysis of fibrotic markers and cytokines. This modified figure is being reused with the permission of previous publication9 in Mucosal Immunology, 2019 by Mathur et al. Please click here to view a larger version of this figure.

Figure 3: Rapamycin treatment effectively ameliorates TNBS-induced fibrosis. A. Colon histological analysis – representative images of myofibroblast staining with anti-αSMA antibody and collagen staining with Trichrome blue, scale bar 100 µm. B. qPCR analysis of αSMA, Collagen and TGFβ expression in Control/TNBS-treated mouse colons. C. FACS analysis of αSMA in single cell suspension from mouse colon treated with Control/TNBS. D. Schematic for purification of Cx3Cr1+ cells from colonic lamina propria fraction and FACS analysis of purified cells. E. Western blot analysis of p-p70 and p-S6 levels in purified Cx3Cr1+ mononuclear phagocytes from mice treated with TNBS and/or rapamycin. F. qPCR analysis of the expression in purified Cx3Cr1+ mononuclear phagocytes, which produces IL-23 and IL-1β. This modified figure is being reused with the permission of previous publication9 in Mucosal Immunology, 2019 by Mathur et al. Please click here to view a larger version of this figure.
