A Reversible Silicon Oil-Induced Ocular Hypertension Model in Mice
Summary
Here, we present a protocol to induce ocular hypertension and glaucomatous neurodegeneration in mouse eyes by intracameral injection of silicone oil and the procedure for silicone oil removal from the anterior chamber to return elevated intraocular pressure to normal.
Abstract
Elevated intraocular pressure (IOP) is a well-documented risk factor for glaucoma. Here we describe a novel, effective method for consistently inducing stable IOP elevation in mice that mimics the post-operative complication of using silicone oil (SO) as a tamponade agent in human vitreoretinal surgery. In this protocol, SO is injected into the anterior chamber of the mouse eye to block the pupil and prevent inflow of aqueous humor. The posterior chamber accumulates aqueous humor and this in turn increases the IOP of the posterior segment. A single SO injection produces reliable, sufficient, and stable IOP elevation, which induces significant glaucomatous neurodegeneration. This model is a true replicate of secondary glaucoma in the eye clinic. To further mimic the clinical setting, SO can be removed from the anterior chamber to reopen the drainage pathway and allow inflow of aqueous humor, which is drained through the trabecular meshwork (TM) at the angle of the anterior chamber. Because IOP quickly returns to normal, the model can be used to test the effect of lowering IOP on glaucomatous retinal ganglion cells. This method is straightforward, does not require special equipment or repeat procedures, closely simulates clinical situations, and may be applicable to diverse animal species. However, minor modifications may be required.
Introduction
The progressive loss of retinal ganglion cells (RGCs) and their axons is the hallmark of glaucoma, a common neurodegenerative disease in the retina1. It will affect more than 100 million individuals 40−80 years old by 20402. IOP remains the only modifiable risk factor in the development and progression of glaucoma. In order to explore the pathogenesis, progression, and potential treatments of glaucoma, a reliable, reproducible, and inducible experimental ocular hypertension/glaucoma model that replicates key features of human patients is imperative.
IOP depends on aqueous humor inflow to the anterior chamber from the ciliary body in the posterior chamber and outflow through the trabecular meshwork (TM) at the angle of the anterior chamber. Upon reaching a steady state, IOP is maintained. When the inflow exceeds or is less than the outflow, IOP rises or falls respectively. By decreasing the aqueous outflow either by occluding the angle of the anterior chamber or by damaging the TM, several glaucoma models have been established3,4,5,6,7,8,9,10. These models are normally associated with irreversible ocular tissue damage, and the high IOP in the anterior chamber also causes unwanted complications such as corneal edema and intraocular inflammation, which make retinal imaging and visual function assays difficult to perform and interpret.
To develop a model that overcomes these shortcomings, we focused on the well-sudocumented secondary glaucoma caused by silicone oil (SO) that occurs as a postoperative complication of human vitreoretinal surgery11,12. SO is used as a tamponade in retinal surgeries because of its high surface tension. However, SO can physically occlude the pupil because it is lighter than the aqueous and vitreous fluids, which prevents aqueous flow into the anterior chamber. The obstruction causes IOP elevation in the posterior chamber due to the aqueous humor accumulation. This motivated us to develop and characterize a novel ocular hypertension mouse model based on intracameral SO injection and pupillary block13, with key features of the secondary glaucoma: effective pupillary block, significant IOP elevation that can return to normal after SO removal, and glaucomatous neurodegeneration.
Here we present a detailed protocol for SO-induced ocular hypertension in the mouse eye, including SO injection and removal and IOP measurement.
Protocol
All procedures have been approved by the Institutional Animal Care and Use Committee (IACUC) of Stanford University.
1. Ocular hypertension induction by intracameral injection of SO
- Prepare a glass micropipette for intracameral SO injection by pulling a glass capillary with a pipette puller to generate a micropipette. Cut an opening at the tip of the micropipette and further sharpen the tip with a microgrinder-beveling machine to make a 35°−40° bevel.
- Polish the edges of the bevel and remove all debris by washing with water. Autoclave the micropipette before use.
- Prepare the paracentesis needle for the corneal entry. To do so, attach a 32 G needle to a 5 mL syringe on a Luer lock, and further secure it with tape. Bend the needle bevel tip face up at 30°.
- Prepare the SO injector by attaching and securing a blunt end 18 G needle on a 10 mL syringe first. Then attach a plastic tube with the 18 G needle on one end and fill up with SO as needed through the other end.
- Attach the sterilized micropipette to the plastic tube and push the syringe plunger to fill the entire micropipette with SO.
2. Intracameral SO injection for one eye
- Place a 9−10-week-old male C57B6/J mouse into an induction chamber with 3% isoflurane mixed with oxygen at 2 L/min for 3 min.
- Intraperitoneally inject 2,2,2-tribromoethanol at 0.3 mg/g body weight.
NOTE: Unlike ketamine/xylazine, 2,2,2-tribromoethanol does not cause obvious pupil dilation. - Check for the lack of response to a toe pinch and the lack of movement of the whiskers or the tail to determine the anesthetic strength.
- Place the mouse in a lateral position on a surgery platform. To reduce its sensitivity during the procedure, apply one drop of 0.5% proparacaine hydrochloride to the cornea before the injection.
- Make an entry incision with the 32 G paracentesis needle at the superotemporal quadrant, about 0.5 mm from the limbus.
- Tunnel through the layers of the cornea for about 0.3 mm before piercing into the anterior chamber. Be careful not to touch the lens or iris.
- Withdraw the needle slowly to release some aqueous humor (about 1−2 µL) from the anterior chamber through the tunnel (paracentesis).
- Wait ~8 min to further decrease the IOP. This can be determined by measuring the contralateral, control eye.
- Insert the glass micropipette preloaded with SO through the corneal tunnel into the anterior chamber, with the bevel facing down to the iris surface.
- Push the syringe plunger slowly to inject SO into the anterior chamber until the SO droplet covers most of the iris surface, ~2.3−2.4 mm in diameter.
- Leave the micropipette in the anterior chamber for 10 s more before withdrawing it slowly.
- Gently push the upper eyelid to close the cornea incision to minimize SO leakage.
- Apply antibiotic ointment (bacitracin-neomycin-polymyxin) to the eye surface.
- Throughout the procedure, frequently moisten the cornea with artificial tears.
- Keep the mouse on the heating pad until fully recovered from anesthesia.
3. SO removal
- Prepare the irrigation system.
- Prepare the irrigating solution according to the manufacturer’s instructions and place it in the irrigation bottle. Elevate the irrigating solution bottle to 110−120 cm (81−88 mmHg) above the surgery platform.
- Attach an IV administration set to the irrigating solution bottle. Remove air bubbles from the IV tubing. Connect a 33 G needle bent to 20° face up to the IV tubing.
- To prepare the drainage system, remove the plunger from a 1 mL syringe. Attach a 33 G needle to the syringe and bend the needle to 20°.
- Remove SO from the anterior chamber.
- Intraperitoneally inject 2,2,2-tribromoethanol (0.3 mg/g body weight). Check for the lack of response to the toe pinch to determine the anesthetic strength and the lack of movement of the whiskers or the tail.
- Place the mouse on a surgery platform and secure it in the lateral position with tape. Apply one drop of 0.5% proparacaine hydrochloride to the cornea to reduce its sensitivity.
- Make two incisions in the temporal quadrant of the cornea between ~2 and 5 o’clock at the edge of the SO droplet using the premade 32 G paracentesis needle.
- Insert a 33 G irrigation needle connected to irrigating solution through one corneal incision, maximum speed.
- Insert another 33 G drainage needle attached to the syringe without a plunger through the other corneal incision to allow the SO droplet to exit the anterior chamber while irrigating with irrigating solution.
- Withdraw the drainage needle, then the irrigation needle.
- Inject an air bubble into the anterior chamber to maintain its normal depth and press to close the corneal incision.
- Apply antibiotic ointment to both eyes.
- Keep the mouse on the heating recovery pad until fully recovered from the anesthesia.
4. IOP measurement once a week
- Place the mouse into an induction chamber perfused with 3% isoflurane mixed with oxygen at 2L/min for 3 min.
- Intraperitoneally inject xylazine and ketamine (0.01 mg xylazine/g, 0.08 mg ketamine/g).
- Keep the cornea moist by applying artificial tears throughout the procedure.
- Wait about 15 min to allow the pupil to fully dilate.
- Measure the IOP of both eyes using a tonometer according to product instructions. Bring the tonometer near the mouse eye. Keep the distance from the tip of the probe to the mouse cornea at about 3−4 mm. Press the measuring button 6x to generate one reading. Three machine-generated readings are obtained from each eye to acquire the mean IOP.
- Sacrifice the animals at 8 weeks after SO injection and perform immunohistochemistry of whole-mount retina, RGC counting, optic nerve (ON) semi-thin sections, and quantification of surviving axons, which have been described before13.
Representative Results
Soon after the injection we can easily identify mice that do not produce stable ocular hypertension because of the SO droplets being too small (≤1.5 mm)13. These animals are excluded from subsequent experiments. Following the injection procedures, more than 80% of SO injected mice end up with droplets larger than 1.6 mm. We measured the IOP of these mouse eyes once a week for 8 weeks after a single SO injection. The IOP of the eye receiving SO remained high, generally double the IOP of the contralateral control eye, indicating effective pupil blocking (Figure 1). Edema in the mouse cornea can be checked under a light dissection microscope after an intracameral injection that normally takes 2−3 days for recovery. The pupil dilation takes time, and one must wait for pupil dilation before taking the IOP measurement. Thus, we try to not measure the IOP too soon after an injection. For the same reason, we do not recommend measuring the IOP too often. With another group of mice, we flushed out the SO from the anterior chamber 2 weeks after SO injection, and we waited for another week to allow the cornea to recover before measuring IOP, which stably returned the IOP to normal (Figure 1).
To determine the effects of ocular hypertension induced by SO injection on RGCs, we quantified the surviving RGC somata in the peripheral regions of the retinal wholemounts by RBPMS staining14,15 and the surviving axons in the ON semithin cross sections by PPD staining16 at 8 weeks after SO injection. Glaucomatous RGC death and axon degeneration were dramatic in SO-induced ocular hypertension under-detected eyes (SOHU) (Figure 2). Further details on this is provided in the discussion section.
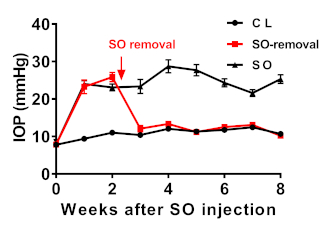
Figure 1: IOP measurements in SO eyes and contralateral control eyes, with or without SO removal. SO = SO injected eyes; CL = contralateral control eyes. Data are presented as means ± S.E.M, n = 12. Please click here to view a larger version of this figure.
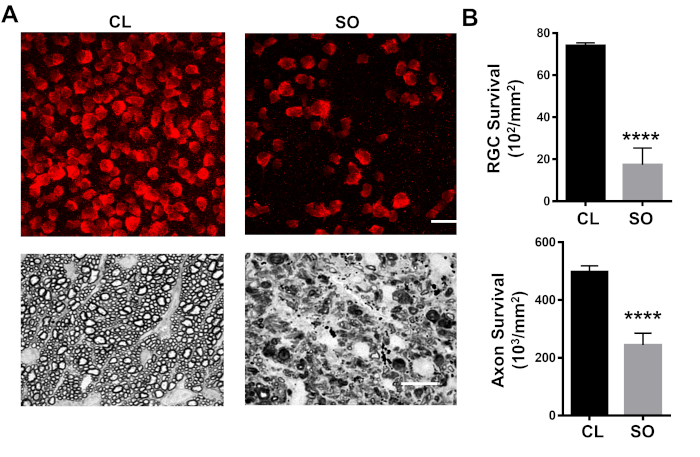
Figure 2: Glaucomatous RGC soma and axon degeneration in SOHU. (A) Upper panel depicts the peripheral region showing RGCs (RBPMS+, red) at 8 weeks after SO injection of whole-mounted retinas. Scale bar = 20 µm. Lower panel depicts semi-thin images of cross sections of the ON stained with PPD at 8 weeks after SO injection. Scale bar = 10 µm. (B) Quantification data of surviving RGCs in the peripheral retina (n = 12) and axons in the ON (n = 10) at 8 weeks after SO injection compared to contralateral control (CL) eyes. Data are presented as means ± S.E.M. ****: P < 0.0001; Student’s paired t test. RGC = retinal ganglion cell; ON = optic nerve. Please click here to view a larger version of this figure.
Discussion
Here we demonstrate a simple but effective procedure for inducing sustained IOP elevation in the mouse eye by intracameral injection of SO. This procedure can be learned quickly by anyone with experience in microdissection under a microscope. The primary potential risk of failure is the leakage of SO from the corneal incision. However, one of the advantages of using SO is that because the oil droplet is visible and measurable, we can easily identify mice that received droplets too small to induce stable ocular hypertension soon after injection and exclude them from subsequent experiments. We have routinely achieved an 80% success rate and excluded about 20% of mice due to a small SO droplet (≤1.5 mm)13. However, an experienced surgeon who can make a relatively long tunnel (0.3 mm) within the layers of the cornea before penetrating the cornea into the anterior chamber with the beveled tip can almost prevent any SO leakage by making the inner opening of the corneal tunnel much smaller than the outer opening. Therefore, almost all of the mice were injected with a SO droplet larger than 1.8 mm. In addition to the length of the tunnel, some other critical points are worth emphasizing. First, it is important to keep the IOP low in the injected eye to avoid pushing the SO out of the anterior chamber. One common mistake is to inject too much SO, which makes leakage easier. We limit the volume of SO in the anterior chamber so that it almost, but not entirely, covers the iris surface. The diameter of this SO droplet is ~2.3−2.4 mm. Second, the corneal tunnel incision is made as close as possible to the limbus to allow the incision to get close to the iris but not hurt it, so that the iris can easily take the incision. Third, the injection speed should be as slow as possible to avoid excessive overflow of SO into the anterior chamber. Fourth, the upper eyelid massage after the injection helps the corneal incision to close and sometimes assists the anterior synechiae of the peripheral iris to close the corneal incision, and therefore to avoid oil leakage.
There is an increase in the IOP only in the posterior part of the eye, but not in the anterior chamber, making it a unique feature of this model. Pupil blocking prevents aqueous humor inflow into the anterior chamber and therefore increases IOP only in the posterior part. The physical barrier formed by the SO together with the iris and large eye lens may disconnect the anterior chamber from the posterior segment, which may limit IOP elevation only in the posterior segment, where the aqueous material accumulates. When the mouse pupil is larger than the SO droplet after dilation, the anterior and posterior chambers are reconnected, allowing a quick increase of IOP in the anterior chamber by aqueous flooding into it. Therefore, a tonometer can only detect the increased IOP after removing the pupillary block, so the true IOP in the posterior segment is undoubtedly underestimated. Therefore, we named this model the SO-induced ocular hypertension under-detected model (SOHU), which more accurately and usefully reflects this key feature of the model. It would be best to be able to measure the IOP in the posterior segment directly, but so far it is not possible. This unique pathogenesis of the SOHU model has two advantageous characteristics: First, the experimental eyes have clear ocular elements that allow in vivo assessment of visual function and morphology and second, the severe glaucomatous neurodegeneration allows any benefit of testing neuroprotectants to be detected.
SO injection can cause corneal edema temporarily and we recommend not performing IOP measurements too early or too often. We did not detect any inflammation in the anterior chamber or cornea in SOHU eyes, although we encountered two instances of cornea neovascularization in the more than 100 mice receiving SO injections.
Because SO causes ocular hypertension in both human patients and mice, it is reasonable to postulate that this conceptually novel and practically significant glaucoma model can be adapted for larger animals that are more suitable for preclinical applications. The characterization of the deficits in neural function and morphology of this model will certainly encourage other investigators to take advantage of it to pursue important questions regarding glaucoma and, even more broadly, diseases that induce RGC and ON degeneration.
In summary, this is a straightforward animal glaucoma model that does not require special equipment or repeat injuries and may be applicable to other animal species. Intriguingly, the IOP elevation of SOHU model can be reversed by removing the oil from the anterior chamber, thus it is useful for screening the neuroprotective treatment combined with IOP lowering therapies.
Divulgations
The authors have nothing to disclose.
Acknowledgements
This work is supported by NIH grants EY024932, EY023295, and EY028106 to YH.
Materials
| 0.5% proparacaine hydrochloride | Akorn, Somerset | ||
| 10mL syinge | BD | Luer-Lok Tip | |
| 18G needle | BD | with Regular Bevel, Needle Length:25.4 mm | |
| 2,2,2-Tribromoethanol (Avertin) | Fisher Scientific | CAS# 75-80-9 | 50g |
| 32G nano | BD | 320122 | BD Nano Ultra Fine Pen Needle-32G 4mm |
| 33G ophalmology needle | TSK/ VWR | TSK3313/ 10147-200 | |
| 5mL syinge | BD | Luer-Lok Tip | |
| AnaSed Injection (xylazine) | Butler Schein | 100 mg/ml, 50 ml | |
| artificial tears | Alcon Laboratories | 300651431414 | Systane Ultra Lubricant Eye Drops |
| BSS PLUS Irrigating solution | Alcon Laboratories | 65080050 | |
| Dual-Stage Glass Micropipette Puller | NARISHIGE | PC-10 | |
| EZ-7000 Classic System | EZ system | ||
| Isoflurane | VetOne | 502017 | isoflurane, USP, 250ml/bottle |
| IV Administration sets | EXELint/ Fisher | 29081 | |
| KETAMINE HYDROCHLORIDE INJECTION | VEDCO | 50989-996-06 | KETAVED 100mg/ml * 10ml |
| microgrind bevelling machine | NARISHIGE | EG-401 | |
| Miniature EVA Tubing | McMaster-Carr | 1883T4 | 0.05" ID, 0.09" OD, 10 ft. Length |
| silicon oil (SILIKON) | Alcon Laboratories | 8065601185 | 1,000 mPa.s |
| Standard Glass Capillaries | WPI/ Fisher | 1B150-4 | 4 in. (100mm) OD 1.5mm ID 0.84mm |
| TonoLab tonometer | Colonial Medical Supply, Finland | ||
| veterinary antibiotic ointment | Dechra Veterinary | 1223RX | BNP ophthalmic ointment, Vetropolycin |
References
- Chang, E. E., Goldberg, J. L. Glaucoma 2.0: neuroprotection, neuroregeneration, neuroenhancement. Ophthalmology. 119 (5), 979-986 (2012).
- Tham, Y. C., et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 121 (11), 2081-2090 (2014).
- Pang, I. H., Clark, A. F. Rodent models for glaucoma retinopathy and optic neuropathy. Journal of Glaucoma. 16 (5), 483-505 (2007).
- Morrison, J. C., Johnson, E., Cepurna, W. O. Rat models for glaucoma research. Progress in Brain Research. 173, 285-301 (2008).
- McKinnon, S. J., Schlamp, C. L., Nickells, R. W. Mouse models of retinal ganglion cell death and glaucoma. Experimental Eye Research. 88 (4), 816-824 (2009).
- Chen, S., Zhang, X. The Rodent Model of Glaucoma and Its Implications. Asia Pacific Journal of Ophthalmology (Philadelphia). 4 (4), 236-241 (2015).
- Sappington, R. M., Carlson, B. J., Crish, S. D., Calkins, D. J. The microbead occlusion model: a paradigm for induced ocular hypertension in rats and mice. Investigative Ophthalmology and Visual Science. 51 (1), 207-216 (2010).
- Chen, H., et al. Optic neuropathy due to microbead-induced elevated intraocular pressure in the mouse. Investigative Ophthalmology and Visual Science. 52 (1), 36-44 (2011).
- Cone, F. E., Gelman, S. E., Son, J. L., Pease, M. E., Quigley, H. A. Differential susceptibility to experimental glaucoma among 3 mouse strains using bead and viscoelastic injection. Experimental Eye Research. 91 (3), 415-424 (2010).
- Samsel, P. A., Kisiswa, L., Erichsen, J. T., Cross, S. D., Morgan, J. E. A novel method for the induction of experimental glaucoma using magnetic microspheres. Investigative Ophthalmology and Visual Science. 52 (3), 1671-1675 (2011).
- Ichhpujani, P., Jindal, A., Jay Katz, L. Silicone oil induced glaucoma: a review. Graefes Archieves for Clinical and Experimental Ophthalmology. 247 (12), 1585-1593 (2009).
- Kornmann, H. L., Gedde, S. J. Glaucoma management after vitreoretinal surgeries. Current Opinion in Ophthalmology. 27 (2), 125-131 (2016).
- Zhang, J., et al. Silicone oil-induced ocular hypertension and glaucomatous neurodegeneration in mouse. Elife. 8, (2019).
- Kwong, J. M., Caprioli, J., Piri, N. RNA binding protein with multiple splicing: a new marker for retinal ganglion cells. Investigative Ophthalmology and Visual Science. 51 (2), 1052-1058 (2010).
- Rodriguez, A. R., de Sevilla Muller, L. P., Brecha, N. C. The RNA binding protein RBPMS is a selective marker of ganglion cells in the mammalian retina. Journal of Comparative Neurology. 522 (6), 1411-1443 (2014).
- Smith, R. S. . Systematic evaluation of the mouse eye : anatomy, pathology, and biomethods. , (2002).
