Following the described protocol, an anatomically realistic phantom was fabricated, which consists of a patient-specific skull, brain and tumor. The relevant anatomical structures for the phantom (skull, brain, tumor) are segmented using patient MRI and CT data (Figure 2a,b). The patient intra-operative ultrasound data (Figure 2c; Figure 2d shows the same image as Figure 2c, but with the tumor outlined) was used to compare the phantom images to the real patient images.
Meshes were created for each piece of the model (Figure 3), and these were then used to manufacture the 3D molds. The molds were easily printed on a commercial printer and assembled by slotting the pieces together. The cerebellum mold was the most complex to design and assemble (Figure 4). The skull (Figure 5a) was the most difficult part to print as it required support material, so was a slow process; the whole print took a total of three days to complete, which is a limiting factor in the protocol.
The completed phantom (Figure 5) was a realistic model of a patient skull, brain and tumor. The two brain hemispheres (Figure 5b) were produced separately, and have a realistic appearance, featuring the gyri and sulci of the brain. The whole phantom is white in color, as this is the natural color of PVA-c; this can easily be changed by adding dye but was not necessary for the application. The cerebellum (Figure 5c) fits comfortably into the base of the printed skull and the brain hemispheres sit on top of this. The tumor is easily visible in the cerebellum, as the extra contrast added to the tumor results in it being an off-white color that separates it from the surrounding material, which is it securely attached to.
The phantom was imaged with both CT and ultrasound (Figure 6a,b). Barium sulfate was used to give the tumor appropriate CT contrast, and the phantom image (Figure 6a) shows that this was achieved, as the tumor is clearly visualized. The skull was not printed with 100% infill, in order to reduce the time taken for printing. Therefore, the skull does not look entirely realistic in the CT images, because the lattice structure of the print can be seen. This is not a problem for the application, as only the outline of the skull is needed for the neuronavigation system. The skull could be printed with 100% infill to avoid this reduced accuracy of the CT image, but would add time onto the printing process. Glass microspheres were added to the cerebellum, brain hemispheres and tumor for ultrasound contrast. The results show that the tumor is also visible with ultrasound imaging (Figure 6b) and can be distinguished from the surrounding tissue. On visual inspection, the ultrasound images obtained from the phantom (Figure 6b), and those obtained from the patient (Figure 2c) show that the contrast agents used in the phantom were effective for creating realistic imaging properties.
The phantom was tested during surgical simulation in a virtual operating room (Figure 7). The phantom model was positioned on the surgical operating table using a standard skull clamp and the CT scan of the phantom was registered using a clinical neuronavigation system. A retrosigmoid approach to the tumor was simulated and the tumor was imaged using a clinical ultrasound system with a burr hole ultrasound transducer. During the surgical simulation, the phantom model proved to be stable and no damage was observed from manipulating the phantom in the same way the human brain would be during this procedure, so it could be used repeatedly under the same conditions.
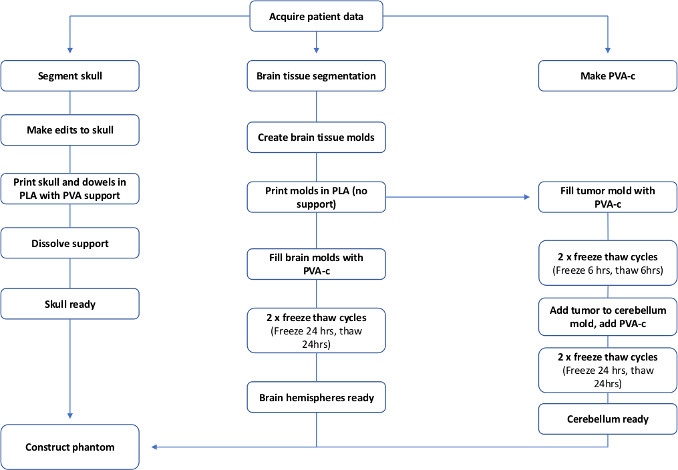
Figure 1: Flowchart to show the steps required to make a patient specific PVA-c brain phantom. Please click here to view a larger version of this figure.
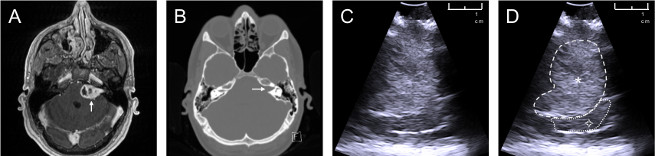
Figure 2: Patient data used to create phantom model. Data sources of a patient with a left sided vestibular schwannoma: (a) axial contrast-enhanced T1-weighted MRI, white arrow pointing towards tumor; (b) axial non-contrast CT scan windowed to highlight bone, white arrow pointing towards an expanded internal auditory meatus caused by the tumor; (c) intraoperative ultrasound image obtained during vestibular schwannoma surgery; (d) annotated intraoperative ultrasound image  : tumor (hyperechoic on ultrasound),
: tumor (hyperechoic on ultrasound),  : brain (cerebellum). Please click here to view a larger version of this figure.
: brain (cerebellum). Please click here to view a larger version of this figure.
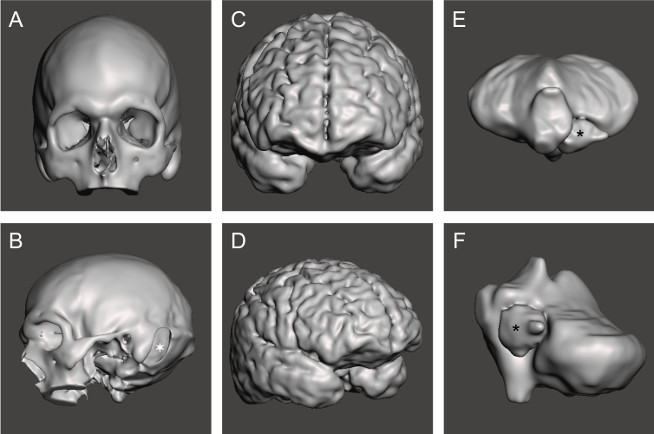
Figure 3: Completed meshes for each section of the phantom. STL mesh for (a,b) skull,  : left sided retrosigmoid craniotomy; (c,d) cerebral hemispheres; (e,f) tumor and cerebellum, : tumor. Please click here to view a larger version of this figure.
: left sided retrosigmoid craniotomy; (c,d) cerebral hemispheres; (e,f) tumor and cerebellum, : tumor. Please click here to view a larger version of this figure.
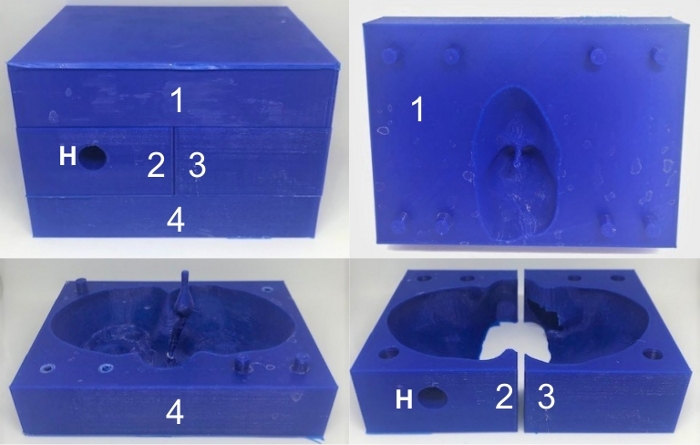
Figure 4: 3D printed cerebellum mold. 3D printed cerebellum mold fully constructed (top left) and the separate pieces, which are numbered from 1 to 4. The hole in piece 2 (denoted by ‘H’) enables the PVA-c to be poured into the mold. Please click here to view a larger version of this figure.
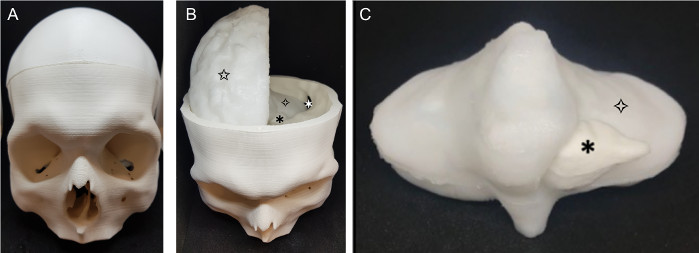
Figure 5: Completed phantom. The finished phantom (a) skull (b) phantom with skull top removed: : retrosigmoid craniotomy, : tumor, brain (cerebellum),  brain (right cerebral hemisphere); (c) cerebellum and tumor: : tumor, brain (cerebellum). Please click here to view a larger version of this figure.
brain (right cerebral hemisphere); (c) cerebellum and tumor: : tumor, brain (cerebellum). Please click here to view a larger version of this figure.
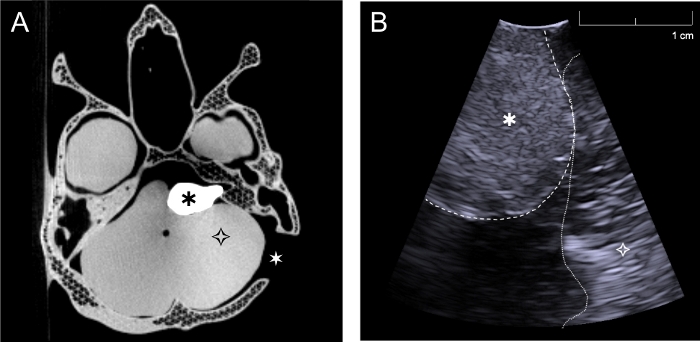
Figure 6: CT and ultrasound images acquired with the phantom. (a) Axial CT image of complete phantom through the level of the skull base and tumor, (b) Intraoperative ultrasound image of phantom acquired with burr hole ultrasound probe through the retrosigmoid craniotomy in a plane approximately perpendicular to the skull (Simulating surgery, the cerebellum was retracted slightly in order to image directly on the tumor). : tumor, brain (cerebellum), : left sided retrosigmoid craniotomy. Please click here to view a larger version of this figure.

Figure 7: Testing the phantom during surgical simulation. Testing the phantom model through surgical simulation in a virtual operating room.  : neuronavigation system displaying the registered scan of the CT phantom model,
: neuronavigation system displaying the registered scan of the CT phantom model,  : ultrasound system used to image the phantom with a burr hole ultrasound transducer (seen positioned next to the ultrasound monitor). Note the model pictured here is based on data acquired from different patient with a right sided tumor. Please click here to view a larger version of this figure.
: ultrasound system used to image the phantom with a burr hole ultrasound transducer (seen positioned next to the ultrasound monitor). Note the model pictured here is based on data acquired from different patient with a right sided tumor. Please click here to view a larger version of this figure.
