In mice, the total volume of CSF is approximately 35-40 µL and is produced at a rate of about 350 nL/min; it turns over 12-13 times a day12. For the purpose of visualizing the route of the injection, 2% Evans Blue was injected via the Murine Ommaya model, following which 15 min and 30 min were allowed to elapse before harvesting the brains for analysis. The dye successfully infiltrated the ventricles and the brain in 15 min. Within 30 min, the dye became visible on the spinal cord (Figure 4).
As a proof of concept, BALB/c mice were injected with a luciferase-labeled Her2+ TUBO breast cancer cell line intracisternally, and the Murine Ommayas were implanted. Approximately 1 week after the injection of cancer cells, the mice began to develop LMD. These mice were treated once a week for up to 4 weeks with Her2-antibody immunotherapy, either through systemic therapy via intraperitoneal injection or intrathecally via the Murine Ommaya (Figure 5A).
Although untreated mice died by day 19, all mice that received intrathecal therapy through the Murine Ommaya survived (P = 0.004). By week 4, a complete regression of tumors was observed. In comparison to mice treated with systemic therapy, which had moderate success in treating LMD, mice that received intrathecal therapy had a much longer overall survival (Figure 5B).
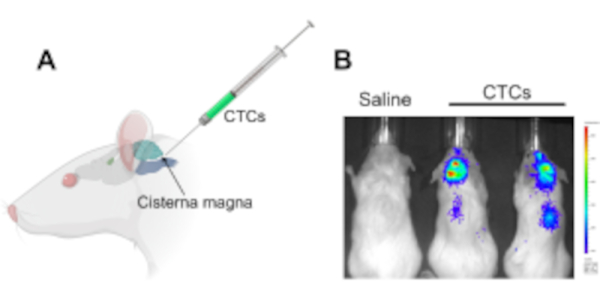
Figure 1: Injection of circulating tumor cells into the cisterna magna in a murine xenograft model to study leptomeningeal disease and central nervous system metastases. (A) An illustration showing the location of the cisterna magna and the CSF accessing site, in which CTCs are injected using a Hamilton syringe. (B) A representative IVIS image of mice that had developed leptomeningeal disease and central nervous system metastases (brain and along the spinal cord) after 2 weeks of injection with circulating tumor cells. Cells were labeled with a luciferase reporter gene. Control animals injected with saline did not develop tumors (n = 3), and the experiment was performed in triplicate. Abbreviations: CTCs = circulating tumor cells; IVIS = in vivo imaging system. Please click here to view a larger version of this figure.
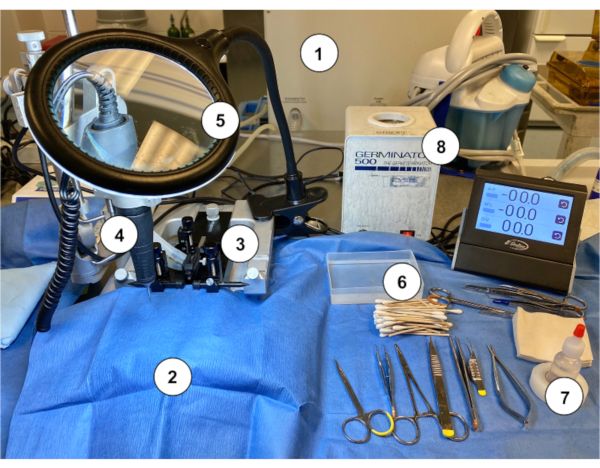
Figure 2: An example of a workstation setup for performing the Murine Ommaya implantation in mice. (1) Gas anesthesia machine/vaporizer. (2) Sterile blue paper drape covering a stereotaxic stand. (3) Stereotaxic device (stand/stage, ear bars, nose cone). (4) Microdrill. (5) Magnifying glass with light. (6) Sterile cotton tapped applicator sticks with sterile saline rinse container. (7) Hydrogen peroxide. (8) Bead sterilizer. Please click here to view a larger version of this figure.
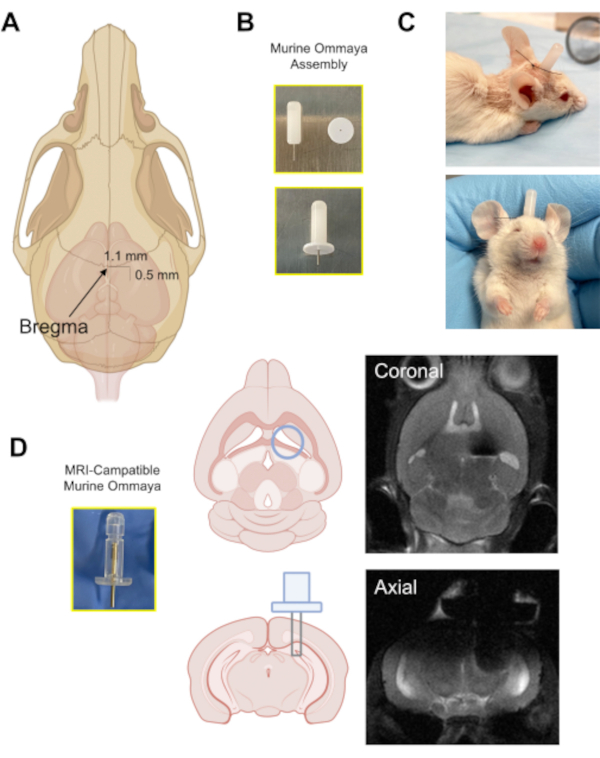
Figure 3: The implantation of the Murine Ommaya device. (A) An illustration with an arrow pointing at the location of the bregma on the skull, and the approximate distance at which a burr hole is drilled in the skull (0.5 mm posterior/1.1 mm lateral) from the bregma using a microdrill. (B) A Murine Ommaya is assembled by combining a metal cannula and a 1 mm spacer as the base for glue attachment to the skull. (C) Representative images of mice that had Murine Ommayas implanted; these mice are monitored to ensure they are bright, alert, and reactive before receiving any injections. (D) An example of the prototype magnetic resonance imaging-compatible Murine Ommaya and representative brain magnetic resonance imaging images of Murine Ommaya implants. Please click here to view a larger version of this figure.
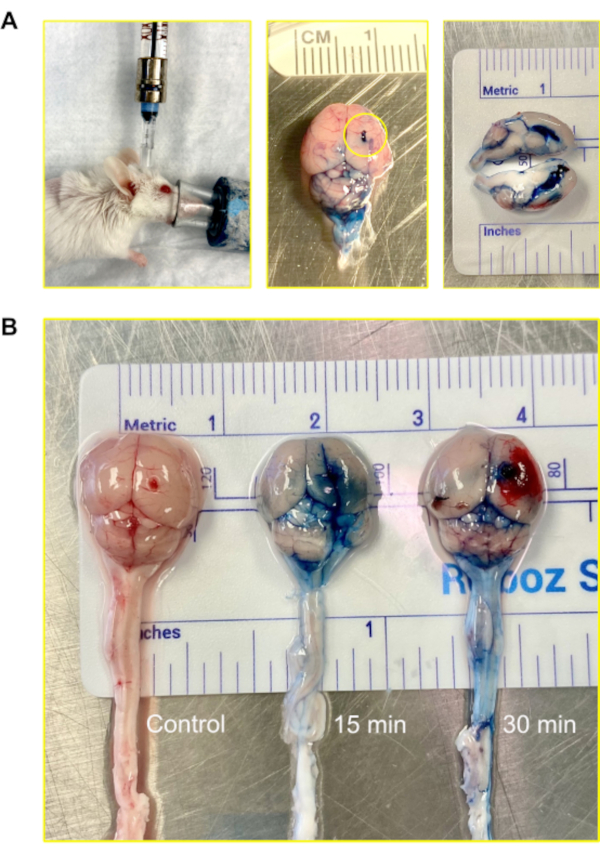
Figure 4: Intraventricular (central nervous system) injection using the Murine Ommaya. (A) An image of an injection, accessing the ventricle and central nervous system via the Murine Ommaya. Mice remain under anesthesia during the injection. In the example, the Murine Ommaya is connected to the miniature port that is attached to a prefilled Hamilton syringe. Injections are performed using an automatic injection set at an infusion rate of 1 µL/min and a volume of 5-7 µL. An image of a mouse brain injected with Evans Blue is shown. The circle shows where the Murine Ommaya was attached. No leakage of the dye was observed on the exterior of the brain. A cross section of the brain shows the lateral ventricles were filled with the dye; the dye did not penetrate brain parenchyma. (B) Images of mouse brains after 15 and 30 min following the injection of Evans Blue dye. The dye infiltrated the brain (15 min) and began to circulate on the spinal cord (30 min). Out of 5 mice, 4 received dye for visualization, and 1 served as control. The experiment was repeated in triplicate. Please click here to view a larger version of this figure.
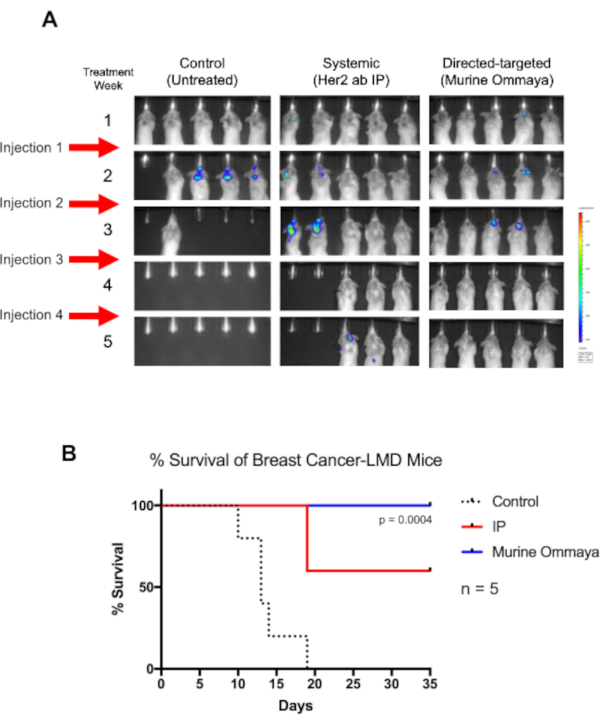
Figure 5: Direct-targeted immunotherapy using the Murine Ommaya increases the overall survival of breast cancer-associated leptomeningeal disease mice. (A) BALB/c mice were injected with luciferase reporter-labeled human epidermal growth factor receptor 2-positive TUBO cells, a murine breast cancer cell line. Three days after cisterna magna injections, Murine Ommayas were implanted. Mice began to develop leptomeningeal disease (LMD) 1 week after injection. LMD mice were treated with either a human epidermal growth factor receptor antibody systemically via intraperitoneal injection or via intrathecal (Murine Ommaya) as a direct-targeted approach. Injections were given once a week for up to 4 weeks. Compared to untreated mice, mice receiving immunotherapy survived much longer. Murine Ommaya mice had complete disease regression by the fourth week, and these mice were eventually cured of disease. (B) These mice also had significantly better median survival (Mantel-Cox test; P = 0.004; n = 5 mice per treatment arm) and better overall survival than systematically treated LMD mice. Abbreviations: LMD = leptomeningeal disease; IP = intraperitoneal. Please click here to view a larger version of this figure.
