A positive result, as shown in Figure 2 and Figure 3, will be a direct translation of the volume rendering as defined in steps 1.2.5 or 2.1.1.4. The final model should visually match the volume rendering in size, shape, and color. Along this process, there are numerous steps where an error can occur, which will affect one or more of the properties listed above.
Issues related to the uniform scaling, as shown in Figure 4, of the printed models can be a result of the imaging, the computer hardware, and/or default software settings. Hospitals use a variety of techniques to produce and render images from a range of possible scanners. As this method works directly from the source images, which can expose metadata not typically utilized, it is important to be familiar with the nuances of the imaging workflow. Issues of scale can arise when 'transformation' is baked into the metadata, which can artificially adjust layer height and rotation.
Scale issues can also be a result of the computer monitor size. Some versions of Slicerfab have been set to slice the volume rendering and save the resulting PNG to the size of the active screen. In these versions of Slicerfab, images that are larger than the monitor will be cut off. Finally, various updates in Photoshop have resulted in scale issues when the updates modify the defaults to the image import resolution. When the default is set to anything other than 600 DPI, the images will not maintain the same scale of images produced by the medical image computing software. They will result in distortions to the X-Y dimension while the z height of the model will remain correct.
Issues related to irregular shapes and unexpected geometries can result when working with opacity in the medical image computing software. The volume properties tab contains the ability to modify both color and opacity channels. When the opacity channel is set below 50%, the rendering algorithms produce visualizations that are difficult for the user to perceive, particularly surrounding complex structures. This can result in additional data being parsed in the process and can lead to unwanted data being 3D printed.
Issues related to color can result from software graphics and user errors in both image editing software and print software. The medical image computing software has numerous choices for adjusting the volume rendering. Although the current version of Slicerfab has hard-coded rendering settings, modifications can still be made. Activating light and shade settings, as well as GPU rendering settings, can produce unexpected and irreproducible results. Finally, the dithering steps starting at step 4.1.2.3 can impact color based on the options for color synthesis, which is determined by the number and relative concentrations of the available base materials in the printer.
The 'local perceptual' dithering algorithm attempts to produce a visual approximation of the source color from the available colors defined in the 'color picker.' Modifying the number and color of the base materials will modify the resulting hue and color accuracy of the printed model. Furthermore, if clear is used as a base material, as shown in Figure 5, issues surrounding surface and subsurface light scattering through the printed model often result in unfaithful color translations from the digital rendering to the printed model6.
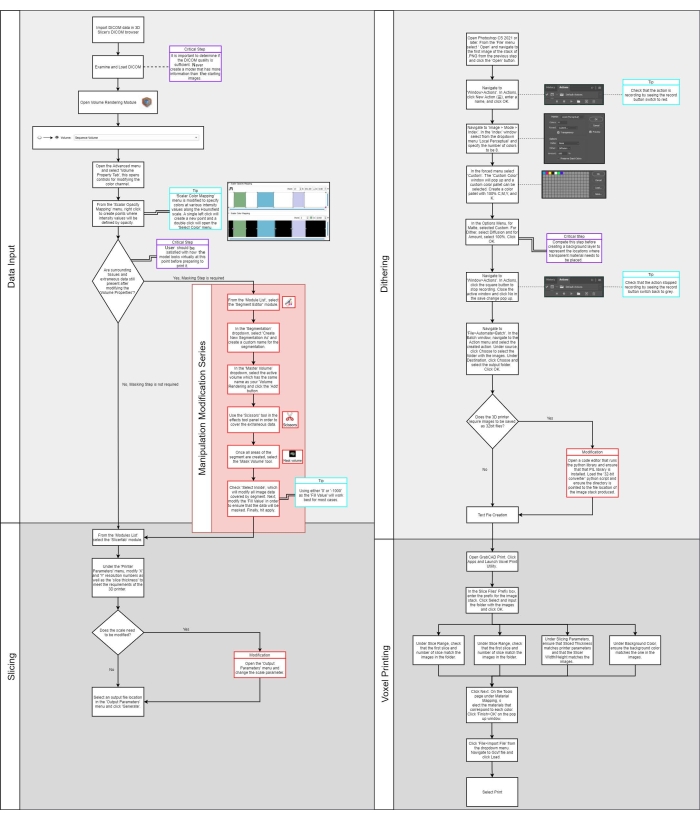
Figure 1: Flow diagram. Please click here to view a larger version of this figure.
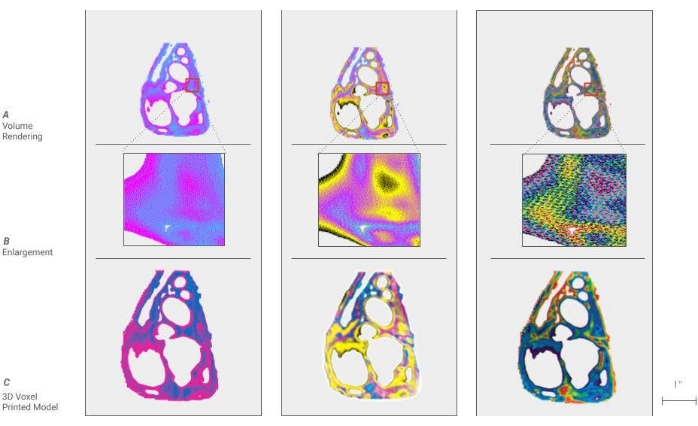
Figure 2: Voxel digital to physical dithering of color. (A) a cross-section of a cardiac model is shown by dividing the density ranges of the anatomy into 2, 4, and 10 colors. (B) An enlargement of a portion of each model is called out, showing the individual pixels, which will be processed to droplets of materials in the 3D printing process. (C) Shown here are cross-sectional 3D printed models using the voxel technique, demonstrating the translation from an image to the model. Please click here to view a larger version of this figure.
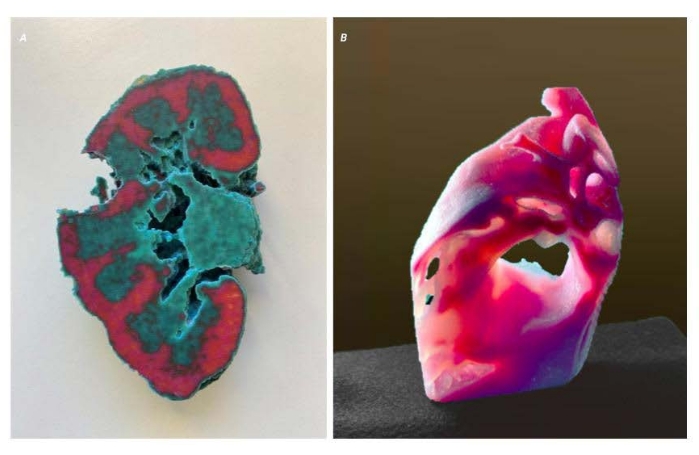
Figure 3: Voxel representative results. Two models displaying representative results of a successful method. (A) A cross-sectional kidney model of an adult with clear cell carcinoma. The tumor on the right side has been removed to show the interface between the kidney and tumor. This allows a surgeon a better understanding of the morphology of the tumor and its relationship to critical elements to be avoided. (B) A sectioned cardiac model showing the variation in tissue density. Please click here to view a larger version of this figure.
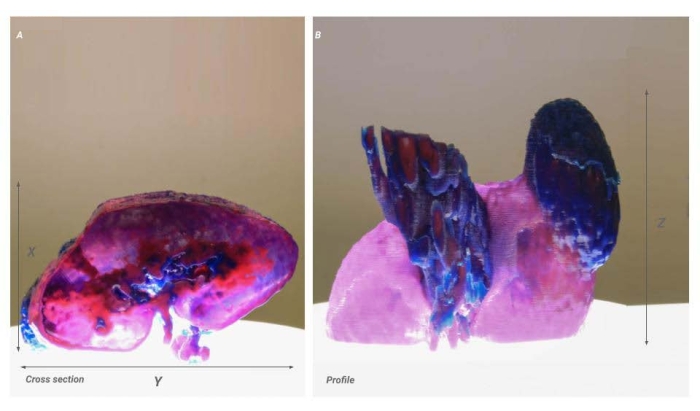
Figure 4: Voxel scale issue. Two images of the same model showing the result of a scaling issue. (A) Cross-sectional image of the kidney. The X-Y resolution is shown proportionally but is 50% of the intended product (B) Profile view of the kidney. The X-resolution remains accurate from the source data and results in a model that appears stretched in the X-direction. Please click here to view a larger version of this figure.
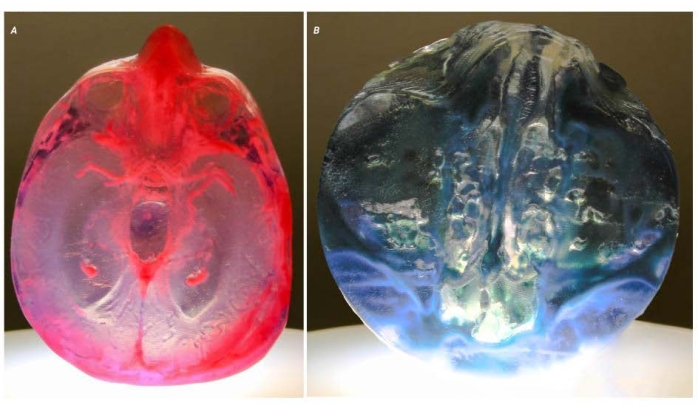
Figure 5: Potential problems. Two images of two different models demonstrate the issues around the clarity of working with translucent materials. (A) This model shows the result of enclosed voids within the model that have been filled with a 'support' material by the printer. In this model, the voids were intentionally created to create a variation in optical properties. (B) This model shows open voids that run deep into the model. The voids are tortuous, making standard postprocessing techniques, which polish the surface, impossible. The resulting optical distortion has rendered the model unusable for clinical applications. Please click here to view a larger version of this figure.
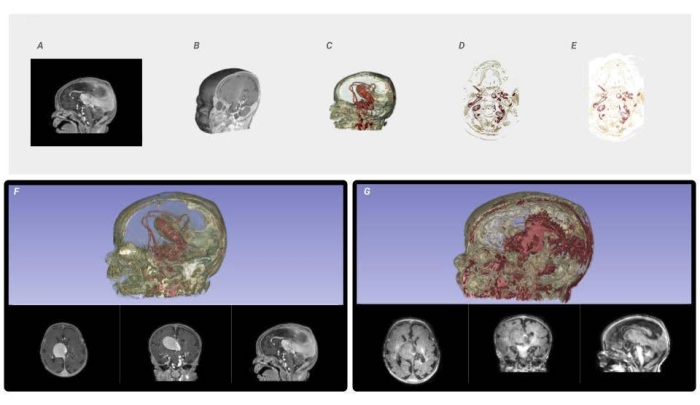
Figure 6: Voxel processing workflow and image quality comparison. From the input DICOM data, (A) a mask is created to isolate the area of interest and reconstruct it into a 3D Volume Rendering, (B) from which a histogram is analyzed to parse the ranges of intensity values. The shape channel of the voxel-based volume rendering is activated to visualize the form of the resulting masked DICOM. The material channel of the voxel-based volume rendering is modified, through lookup tables, which map color to the specified intensity ranges (C). The volume rendering is sliced as full-color PNG files to the required constraints and resolution of the printer (D). Every PNG slice is dithered into the material descriptions needed to fabricate the medical data. (E) The resulting color-composite PNGs are sent to the printer. (F) A visualization of a high-resolution data set compared to a low-resolution data set (G) using the same technique to demonstrate the need for the highest quality source data. Please click here to view a larger version of this figure.
