This study was undertaken to develop a femur osteotomy model in Wistar albino rats. This model can be used to evaluate bone healing, as well as the osteogenic effect of a promising osteoanabolic drug in bone healing. Standard surgical precautions and protocols were followed. Sterile gowns, drapes, and surgical equipment were used for the procedure (Figure 1). The equipment (Table 1) was sterilized 48 h before surgery. Anesthetic, analgesic, and antibiotics were used as per the protocol to ensure that animals were kept pain- and infection-free at all times. Blood (0.5 mL) can be collected from the tail vein of each rat for baseline analysis and sequential chronological comparative follow-up of different parameters as fracture healing occurs. Hair was removed from the flank region to the knee region using hair removal cream (Figure 2). The osteotomy procedure took approximately 10 min to complete (from the first incision to the suture). Infection and mortality were negligible on following aseptic precautions. An incision was made after local anesthesia (lignocaine), and the shaft of the femur was exposed after retracting the fibers of the vastus lateralis (Figure 3). An indentation (groove) was created in the bone using a surgical blade to ensure that the chisel did not slip. Sterile hard support (marble block) was used to support the bone while fracturing it to ensure a clean break (Figure 1). A complete transverse fracture was induced in the middle third of the shaft of the femur using a chisel and hammer (Figure 4).
The fracture was internally fixed using a sterile K-wire (1.0 mm). The K-wire was passed into the medullary canal of the distal fragment through the fracture site. The K-wire was then drilled out through the distal end of the femur. The fracture was reduced, and then the K-wire was advanced from the distal end into the canal of the proximal fragment until it obtained purchase in the trochanteric region. The distal part of the K-wire that protruded through the skin was cut off. The K-wire acted as an intramedullary splint to keep the fracture in a reduced position (Figure 5).
An X-ray of the fractured area was taken 1 day post surgery and weekly thereafter to evaluate the appearance of the callus (beginning of fracture healing) and appearance of the bridging callus (the first time point when the fracture gap was healed), as evaluated by the radiologist (Figure 6). Two radiological time points for comparative evaluation of fracture healing were the appearance (visualization) of the (soft) callus and the appearance of the bridging (hard) callus.
After sacrifice, the femur was carefully preserved in formalin, followed by the protocol for bone decalcification (Figure 7). The K-wire was removed during the sacrifice, taking care not to disturb the callus. After complete decalcification, the bone was cut into sagittal sections and preserved in paraffin blocks for sectioning (4 µm thick sections) as and when required. A hematoxylin-and-eosin-stained section of the fracture site and callus confirmed cartilage and new bone formation at the end of 5 weeks (Figure 8).
Figure 1: Sterile surgical instruments kept on the surgical drape on the operating table. The surgeon is ready to start the surgical procedure in a sterile environment with sterile instruments. Please click here to view a larger version of this figure.
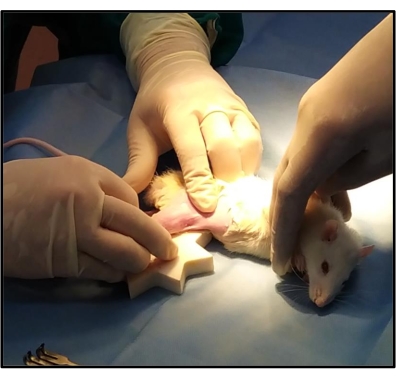
Figure 2: Anesthetized rat kept on the operating table. After giving anesthesia to the rat and removing the hair around the incision site, it is kept on the operating table in a left lateral position, exposing the right leg for osteotomy. Another surgical drape is used to pass the right leg through a hole in that drape to ensure that only the leg is exposed, thereby minimizing wound infections. Please click here to view a larger version of this figure.
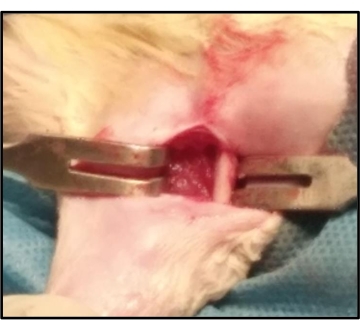
Figure 3: Surgical procedure: Exposure of the shaft of the rat femur. During osteotomy, after the vastus lateralis is exposed, it is split in line with the muscle fibers to expose the shaft of the femur. The bone is freed from the attached muscles using the periosteal elevator. Please click here to view a larger version of this figure.

Figure 4: Creating a complete transverse osteotomy in the middle third of the shaft of the femur using a chisel and hammer. A complete transverse fracture is created in the middle one-third of the shaft of the femur by gently tapping the chisel with the hammer. Please click here to view a larger version of this figure.
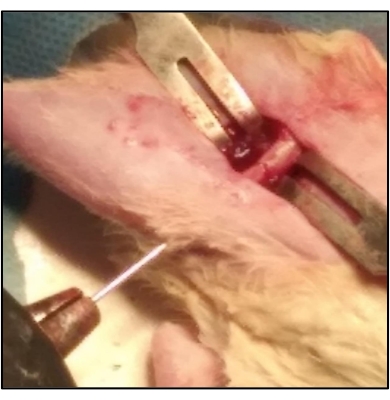
Figure 5: K-wire acts as an intramedullary splint for keeping the fracture in a reduced position. The K-wire is passed into the medullary canal of the distal fragment through the fracture site. The K-wire is then drilled out through the distal end of the femur. The fracture is reduced and then the K-wire is advanced from the distal end into the canal of the proximal fragment until it obtained purchase in the trochanteric region. This is done using a battery-operated power drill. Please click here to view a larger version of this figure.
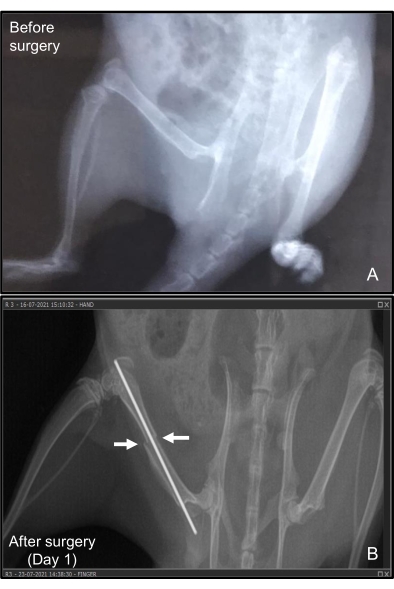
Figure 6: X-ray of the femur of the rat with the K-wire in situ. (A) Before inducing the fracture and (B) 1 day after surgery. The fracture healing is monitored radiologically by taking sequential weekly X-rays of the operated site to radiologically assess callus formation. The fracture remains reduced and immobilized with the intramedullary K-wire. The before and after representative data are not from the same animal. Please click here to view a larger version of this figure.
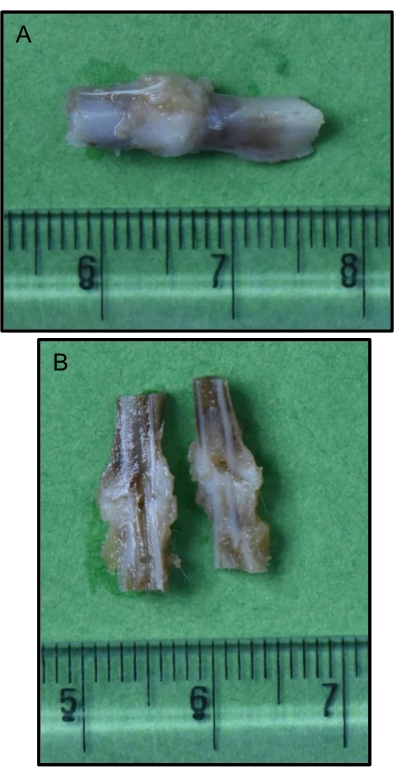
Figure 7: Bone with callus (after optimal decalcification) obtained after sacrificing the animal at a pre-determined time point. (A) Intact callus; (B) Sagittal section of the callus. After sacrificing the animal, the area of the fracture site is obtained, preserved, and decalcified using the described methodology. The callus is intermittently assessed to ensure optimal decalcification before evaluating it by any other techniques (reference scale in centimeters). Please click here to view a larger version of this figure.
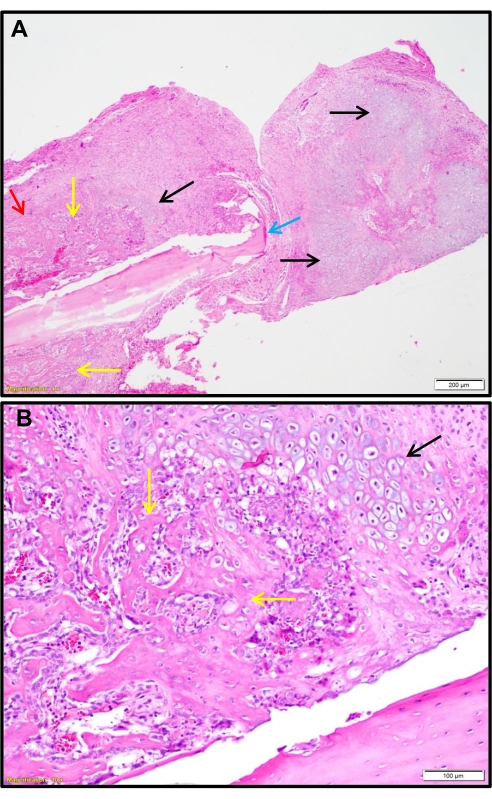
Figure 8: Hematoxylin-and-eosin-stained section of the fracture site showing a hard callus with the formation of cartilage and new bone. (A) Low magnification; (B) High magnification. The hematoxylin-and-eosin-stained sections of the fracture site show a hard callus with the formation of cartilage (black arrows) and new bone (yellow arrows) (A: 40x; B: 100x). The blue arrow shows the fracture end of the bone, and the red arrow shows the second cortical region. Please click here to view a larger version of this figure.
